Interstitial lung disease Paul Swift What the 1




 Ø ABG sats Ø RR")


























 Can’t be cleared by")


 (Fuse to multinucleated")


 ESR Serum Ca 2+ Serum")







- Slides: 47
Interstitial lung disease Paul Swift
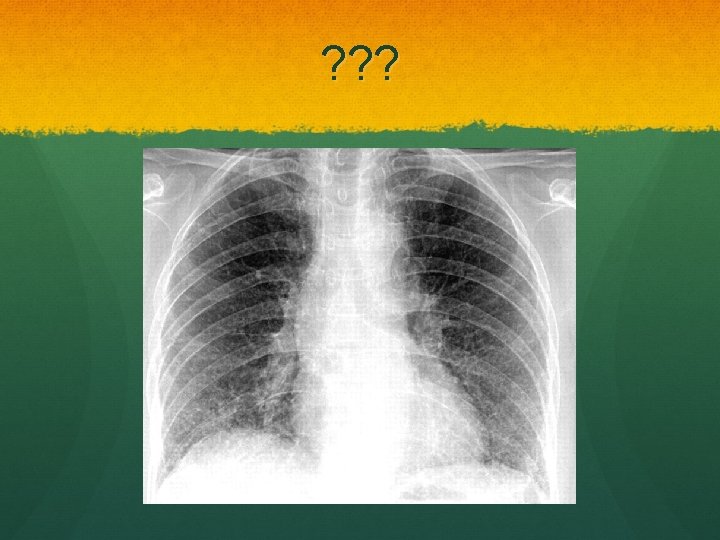
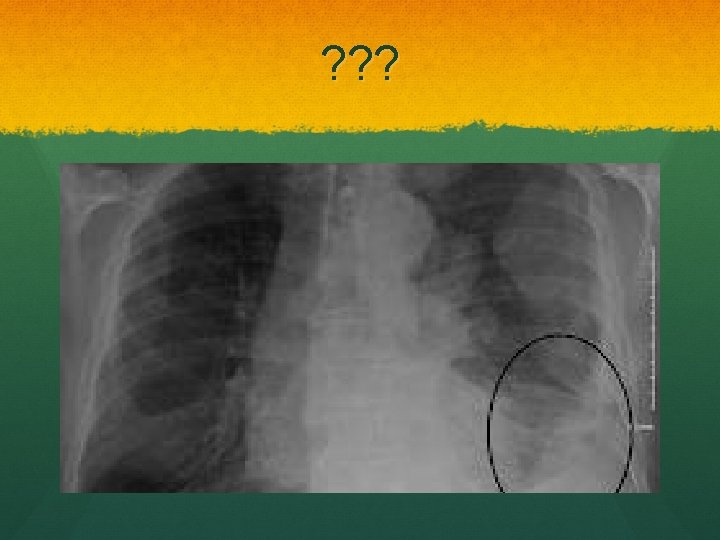
What the? 1. Extrinsic Allergic alveolitis 2. Idiopathic pulmonary fibrosis 3. Industrial dust disease 4. Organic dust disease 5. Sarcoidosis
What’s important Pathophysiology Clinical features Investigation Management Prognosis
Expaaaaand Pathophysiology Varies: inflammation scarring fibrosis Presentation Variation on a theme SOBOE, lethargy, dry cough SMOKING, PETS, OCCUPATION O/E Tachypnoea, clubbing Cyanosis Fine end inspiratory creps
Investigation Investigations 1. Bedside Ø PEF (work v. home) Ø ABG sats Ø RR 2. Blood Ø FBC, U&Es, LFTs, CRP, ESR Ø ANA and Rf in IPF sometimes 3. Imaging Ø CXR Ø HRCT
Special tests Lung function tests Restrictive defect FVC is reduced FEV 1 is reduced in proportion or slightly less FEV 1: FVC ratio normal or raised TLCO the key! Thickened fibrotic alveolar walls shit for gas transfer Others: Bronchoscopy, bronchoalveolar lavage
Lung function
Treatment Conservative Weight loss Increased exercise Smoking cessation Medical Oxygen Steroids Surgical Transplant
Extrinsic allergic alveolitis AKA- hypersensitivty penumonitis Type III hypersensitivity reaction Ø Prior sensitisation to inhaled antigen Examples 1. 2. 3. 4. Mould hay (farmer’s lung) Bird faeces (bird fancier’s lung) Cotton fibres (byssionosis) Sugar can fibres (bagassosis)
Famer’s lung
Bird fancier’s lung
EAA- why, why Antigen exposure Hypersensitivity reaction Neutrophil activation Infiltration of small airways and alveolar walls Neutrophils 1 st Then lymphocytes/macrophages Non-caseating granulomas Resolve Organise pulmonary fibrosis
Clinical features Standard stuff Ø Ø Cough SOB Fever Malaise Acute onset hours after exposure Ø More insidious if long-term exposure to small amounts O/E: Coarse end inspiratory crackles- upper lung Ø http: //www. youtube. com/watch? v=HTNo_ovhcv 8
Investigations Bedside Bloods Neutrophil & leukocyte count Ig. G antibody titres
Investigations Imaging CXR Often normal in acute form Subacute- reticular nodular Shadowing Chronic- fibrosis with volume loss HRCT Special Lung function Bronchoalveolar lavage Hisolopathological diagnosis
Treatment Conservative Antigen avoidance!!!! Medical: ? Corticosteroids Yup, severe disease Speed initial recovery Prognosis Variable, depends on antigen avoidance
Idiopathic pulmonary fibrosis AKA- Cryptogenic Fibrosing Alveolitis, Usual Intersitial Pneumonitis Rare progressive chronic pulmonary fibrosis of unknown aetiology Peak @ 45 -65 yrs
IPF- patho Alveolar walls thickened because of fibrosis Predominantly lower lobes Number of chronic inflammatory cells in alveoli and interstitium Usual interstitial pneumonitis Other patterns: Desquamative interstitial pneumonitis Bronchiolitis obliterans
Clinical features Same old SOB Dry cough Fatigue Can get considerable weight loss More chronic/late stage Cyanosis Pulmonary hypertension/cor pulmonale Resp failure
Resp failure
On examination O/E Clubbing 2/3!! Chest expansion reduced Fine-end inspiratory crackles N/B. Associations
Investigations Bedside ABG resp failure Bloods Autoantibodies ANA +ive in 1/3 Rf +ive in ½ Raised ESR
Investigations Imaging CXR HRCT Special Lung function BAL Neutrophils Transbronchial or open lung biopsy for histological diagnosis
Treatment Conservative Stop smoking Weight Exercise Medical 50% respond to immunosuppression with combo therapy recommended: Prednisolone 0. 5 mg/kg 1/12 Azathioprine 2 -3 mg/kg (can sub in cyclophosphamide for azathioprine) Oxygen Surgical Transplant
Prognosis 50% 5 year survival
More dust disease The pneumoconioses CABS Coal Worker’s pneumoconiosis Asbestosis Berylliosis Silicosis Group of disorders due to inhlation of mineral or biological dusts
Coal Worker’s pneumoconiosis Dose dependent Simple Coal dust deposition in the lung Asymptomatic Diagnosis made by several small round opacities on CXR Caplan’s Severe disease may progress to progressive massive fibrosis
Progressive massive fibrosis Large round fibrotic nodules >10 mm Upper lobes Scarring Dyspnoea, cough, sputum May be black if cavitating lesions
PMF
PMF treatment Progresses when exposure removed Unlike simple Prognosis is poor, no treatment Coal Workers Pneumoconiosis Scheme Pneumoconiosis Workers’ Compensation Act 1979 Lump sum compensation
Asbestosis Inhlation of asbestos Plumbers, electricians, builders Blue asbestos (crocidolite) Can’t be cleared by immune system Histology: asbestos bodies and features of pulmonary fibrosis, affecting lower lobes more
Rx No treatment Considerable time lag: 20 -40 years following exposure Compensation Risk……….
Sarcoidosis A 25 -year old afro-Caribbean woman presents with SOB and bilateral leg lesions…… Multisystem granulomatous disorder of unknown aetiology Commonly effects the lungs Non-caseating granulomas Rare (19/100000 in UK) Peak 20 -40 yrs
Sarcoid path Non-caseating granulomas (Infiltrated by Th 1 lymphocytes and macrophages) (Fuse to multinucleated epithelioid cells) Resolution of granulomas 10 -20% persistent interstitial fibrosis
Clinical features 90% have pulmonary involvement SOB Chest pain Cough Non-specific features Lymphadeopathy Weight loss Fever Fatigue
Extrapulmonary features
Inv Bedside The usual Bloods FBC (normochronic normocyctic anaemia) ESR Serum Ca 2+ Serum ACE Can be 2 x normal levels Used to monitor progression Imaging- CXR
More inv
Expensive stuff HRCT Staging Identifying pulmonary fibrosis Biopsy GOLD standard for diagnosis
Rx Hilar lymphadenopathy and no pulmonary involvement = no treatment Medical Infiltration > 6 weeks = steroids Prognosis Depends on stage Mortality < 5% UK Shadowing on CXR >2 years risk pulm fibrosis
Summary Pathogenesis Varied but endstage is fibrosis and inflammation of the alveoli and interstitium Presentation Cough, SOB, fine end inspiratory crackles Smoking, occupation, pets Investigations Bed, blood, imaging, special Lung function- restrictive CT- honeycombing, groundglass Treatment Steroids, transplant, avoid exposure
Case study A 64 year old gentleman presents to his GP with increasing SOB over the last 6 months. His exercise tolerance has reduced to the point where walking to the corner shop makes him out of breath. He also complains of a dry cough. He has a past medical history of high blood pressure which is managed with Ramipril. He has never smoked and works as an office manager. On examination he is slightly short of breath with O 2 sats 93% on air and he has clubbing. Auscultation reveals bilateral basal fine end inspiratory crepitations and no wheeze.
? ? What are your main differential diagnoses for this gentleman? (make sure these include all important differentials that must be ruled out) How would you investigate this gentleman? What is your management plan? Will anything help? Can you tell me about the pathophysiology of ILD? Can you tell me some causative organisms for EAA?
Any questions