Interpreting the cardiopulmonary exercise test CPEXCPETMetabolic testing Sathish
![Interpreting the cardiopulmonary exercise test [CPEX/CPET/Metabolic testing] Sathish Parasuraman Cardio-vascular research fellow University of](https://slidetodoc.com/presentation_image/4f4e559641a6135e72b20f912609d60c/image-1.jpg "Interpreting the cardiopulmonary exercise test [CPEX/CPET/Metabolic testing] Sathish Parasuraman Cardio-vascular research fellow University of")
Interpreting the cardiopulmonary exercise test [CPEX/CPET/Metabolic testing] Sathish Parasuraman Cardio-vascular research fellow University of East Anglia

• When to do it • How to do it? • How do you interpret it? • Some examples

When to do it? 1. When you want the whole picture of how a disease is affecting a person Eg. A young sarcoid / young congenital heart disease patient, you want to review annually 2. Patient with exercise limitation ? due to lung ? due to heart 3. Fitness for surgery November 4, 2020

Quiz! • When the presenting complaint is exercise limitation, what is the best to do? a) b) c) d) Exercise test Coronary angiogram Contrast CT scan of chest Blood tests November 4, 2020

November 4, 2020

What can CPEX tell you? • Exercise time/ECG/BP/Heart rate • Oxygen consumption at peak exercise • When does the anaerobic metabolism begin? • Oxygen saturations at rest and peak exercise November 4, 2020
 = Respiratory frequency * Tidal")
Terminologies in CPEX • VE – “minute ventilation” (Litres) = Respiratory frequency * Tidal volume • VO 2 – Oxygen uptake (ml/kg/min) Ignore V prefix • Peak VO 2 – Oxygen uptake at peak exercise (ml/kg/min) • VCO 2 – Carbon dioxide output (ml/kg/min) You know most terms • AT – Anaerobic Threshold, when anaerobic metabolism supplements exercise • R – Gas exchange ration = VCO 2/VO 2 November 4, 2020

Determinants of exercise capacity November 4, 2020

Energy supply during exercise • Hydrolysis of phosphocreatinine 1 st minute • Oxidation of glucose and fatty acids 2 nd to 10 th minute • Anaerobic metabolism 7 th to 10 th minute November 4, 2020

CO 2 Production during exercise • Glucose + 10 O 2 10 CO 2+ H 2 O + Energy • Palmitate + 10 O 2 7 CO 2 + H 2 O + Energy CO 2 • Anaerobic Glycolysis Lactate + Energy

oxygen and carbon-dioxide kinetics Peak VO 2 < 85% Heart Problem CO 2 P VO 2 Lung problem O 2, CO 2 Blood problem Muscle problem Deconditioning Time November 4, 2020

Respiratory Exchange Ratio RER or simply “R” • RER or R=VCO 2/VO 2 • Climbs steadily after AT • At peak exercise it is >1 November 4, 2020 Anaerobic Threshold or Lactate Threshold

Anaerobic threshold Heart Problem CO 2 O 2, CO 2 Anaerobic threshold Lung problem Blood problem Muscle problem Deconditioning Time November 4, 2020

VO 2 at anaerobic threshold and O 2 pulse • VO 2 at Anaerobic threshold • O 2 pulse = VO 2/heart rate • Surrogate for stroke volume • Normal VO 2 @ AT / Predicted PVO 2 >40% • If VO 2@AT/pred PVO 2 <40% suggests cardiac limitation at AT/pred PVO 2 exercise indicates • VO 2 A fall on incremental cardiac pathology =15. 69/38. 75 =40%

So far. . • Low Peak VO 2 indicates a pathology • Respiratory Exchange Ratio (CO 2/O 2) >1. 15 suggests maximal test • Anaerobic metabolism sets in early in heart failure (<40% of predicted peak VO 2) • Oxygen pulse is a surrogate for stroke volume November 4, 2020

Ventilation • Ventilation is a product of tidal volume and respiratory frequency • VE = tidal volume X resp. freq. • During progressive exercise, dead space decreases, tidal volume increases • Respiratory frequency increases, later, but rarely beyond 50 breaths/minute November 4, 2020

Maximum voluntary ventilation & Breathing reserve • Maximum Voluntary Ventilation – The upper limit of body’s ability to ventilate the lungs Heart Problem Lung problem Blood problem • Maximum Voluntary Ventilation(MVV) = FEV 1*40 Breathing reserve<11 L • Breathing reserve = MVV - VE (Ventilation) at peak exercise November 4, 2020 Muscle problem Deconditioning

Desaturation during exercise • Desaturation suggests a lung problem • Oxygen saturations do not fall markedly until the PO 2 is <8 k. Pa • If saturation falls >5%, it suggests abnormal exercise induced hypoxemia November 4, 2020

Ventilatory efficiency • Ventilatory efficiency of elimination CO 2 Slope 63 Slope 34 • Measured from the beginning of exercise Slope 23 to anaerobic threshold VE-VCO 2 slope <30 degrees November 4, 2020 • High VE/VCO 2 slope indicates ventilationperfusion mismatch Heart Problem Lung problem Blood problem Muscle problem Deconditioning

So far… • Desaturation indicates lung problem • Low breathing reserve indicates lung problem • High VE-VCO 2 slope indicates ventilation-perfusion mismatch November 4, 2020

Truly limited Not the lungs Lung limitation V/Q mismatch and early anaerobic met. High VE/VCO 2 slope November 4, 2020

General considerations • A protocol is chosen, so patient lasts no more than 8 -12 minutes • Reason for stopping could give a clue • Leg fatigue- cardiac • Leg pain-peripheral vascular disease • Chest pain-angina • Breathlessness-lung

64 m Recent diagnosis of prostrate Ca, receiving local radiation Feels tired and breathless Inconclusive treadmill ETT VO 2 at AT/Pred PVO 2 = 18. 27/24. 8 = 74%

64 m Report Recent diagnosis of prostrate Ca, receiving local radiation Normal PVO 2 Normal VO 2 at AT Normal VE/VCO 2 slope Feels tired and breathless Inconclusive treadmill ETT Borderline breathing reserve No desaturation during exercise Abrupt flattening of VO 2, VO 2 pulse towards peak exercise, with unexpected raise on recovery November 4, 2020 Imp Coronary ischemia

Coronary ischemia November 4, 2020

FH of HOCM IVS of 13 mm Fit & well man

FH of HOCM IVS of 12 mm Asymptomatic Report Normal PVO 2 Normal VO 2 at AT Normal spirometry, breathing reserve & saturations Normal VE-VCO 2 slope Imp No exercise limitation

A difficult case • 67 year old man, breathless. X 1 year • Clubbed • CT chest- ground glass opacification, normal LV systolic function • Ex- smoker X 40 PY • Abnormal spirometry with reduced DLCO November 4, 2020

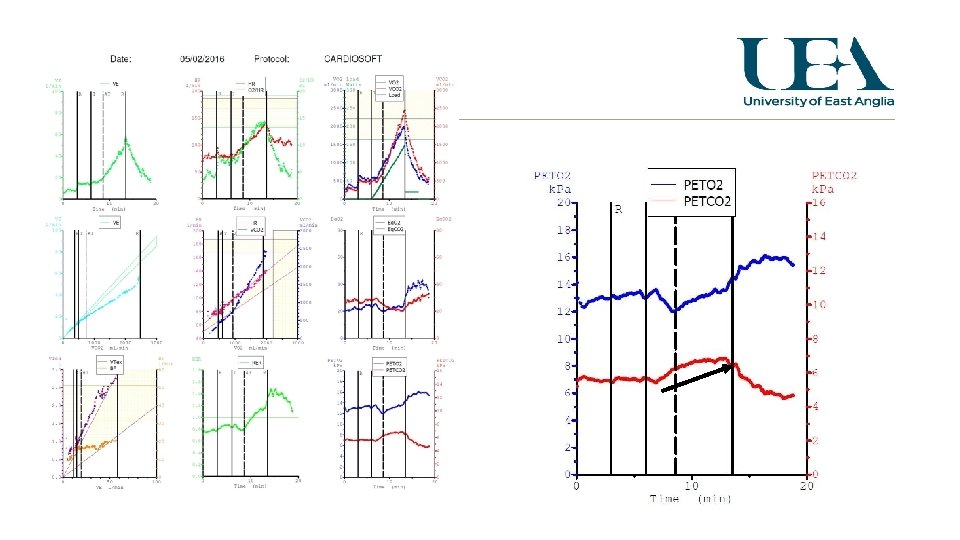
A difficult case • Treadmill CPEX for 7 minutes, stopped due to breathlessness • PVO 2 of 82% of predicted • R of 1. 29 • VO 2 at AT is 53% of predicted PVO 2 • VE/VCO 2 slope is 41 @ RCP • Breathing reserve is 6, maximal respiratory frequency was 40

Oxygen saturation Increased on exercise! suspect this is primary lung issue coexisting ischemia Why the Pa. O 2 increases on exercise? Potential right to left shunt which decreased during exercise ie-pulmonary shunt November 4, 2020

43 m, Breathless HT, DM, congenital blindness Mild LV hypertrophy, normal angiogram, Normal spirometry November 4, 2020

Report Likely mitochondrial myopathy November 4, 2020 PH 7. 19 10 mins recovery Ph 7. 21 20 mins recovery 7. 27

Another difficult case • 19 Female • Being investigated for breathlessness/tiredness • Normal haemoglobin, echocardiogram • Normal FEV 1, FVC, reduced DLCO (65%) • Normal CT (plain) chest

19 f, breathless. Slightly reduced DLCO, normal echo & plain CT Low PVO 2 Low VO 2 at AT Normal breathing reserve November 4, 2020

Report Low PVO 2 Low VO 2 at AT Normal VE-VCO 2 Saturations at peak exercise unclear Very high respiratory frequency Imp/DD Mitochondrial myopathy Left to right shunt November 4, 2020

Evidence base for CPEX • Heart failure patients with PVO 2 < 12 ml/kg/min indicate poor prognosis and are candidates for heart transplantation • In lung cancer- a PVO 2 of <15 ml/kg/min predicts high perioperative risk • In major abdominal and vascular surgeries, VO 2 at AT of <11 ml/kg/min predicts high cardiovascular risk and poor survival November 4, 2020

Thank you! November 4, 2020
- Slides: 38