INTERPRETATION of ELECTROCARDIOGRAMS BRIAN D LE MD Presbyterian

INTERPRETATION of ELECTROCARDIOGRAMS BRIAN D. LE, MD Presbyterian Hospital CIVA

Outline I. III. Approach to interpretation of ECGs Cases illustrating approach principles Unusual Cases

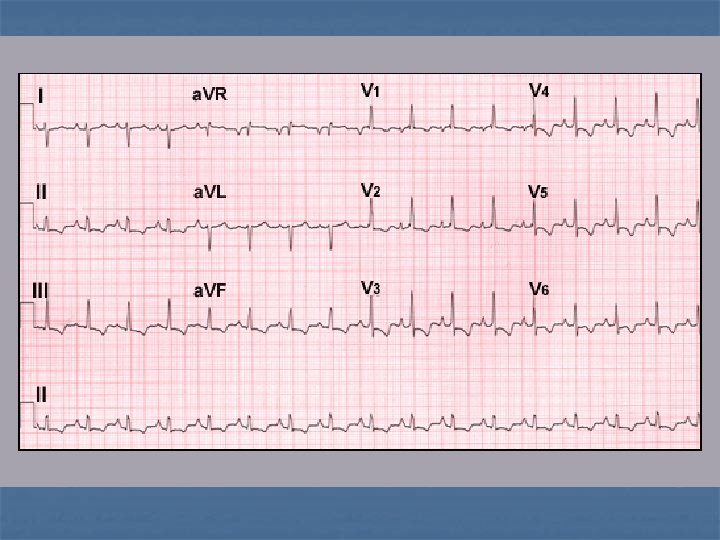
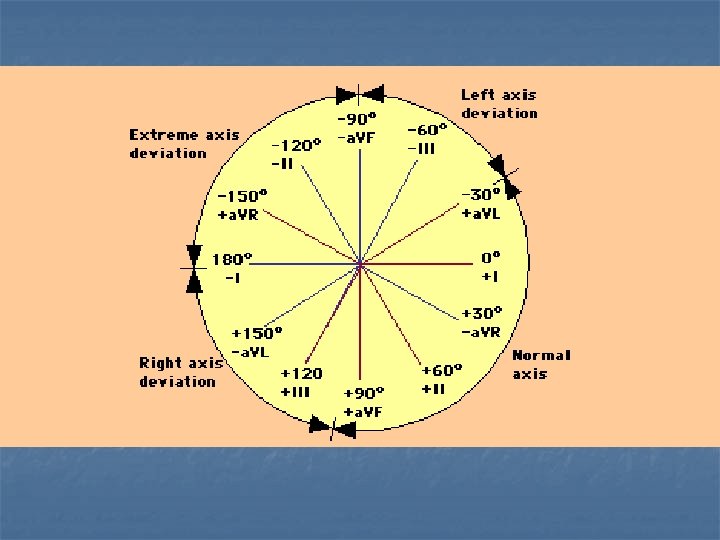
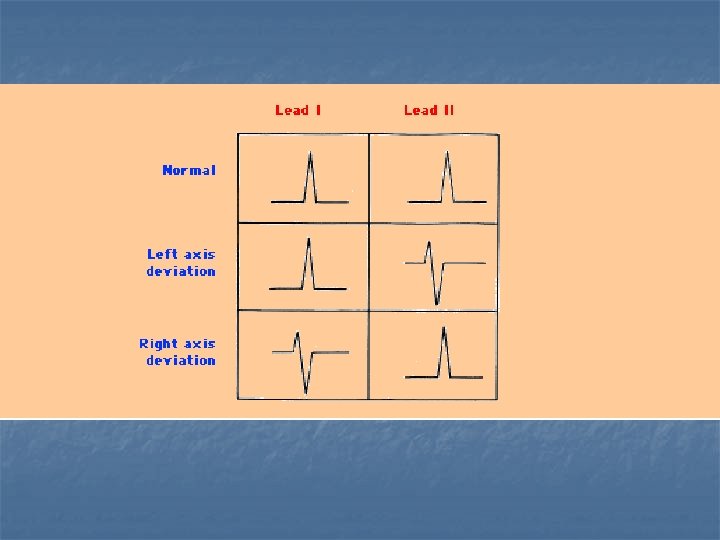
Seven Step Approach n n n n Rate Rhythm Axis Intervals Hypertrophy ST/Tw changes, Q waves Conduction system

Seven Step Approach n n n n Rate Rhythm Axis Intervals Hypertrophy ST/Tw changes, Q waves Conduction system

Seven Step Approach n n n n Rate Rhythm Axis Intervals Hypertrophy ST/Tw changes, Q waves Conduction system

Seven Step Approach n n n n Rate Rhythm Axis Intervals Hypertrophy ST/Tw changes, Q waves Conduction system

Seven Step Approach n n n n Rate Rhythm Axis Intervals Hypertrophy ST/Tw changes, Q waves Conduction system

INTERVALS PR < 200 ms QRS < 120 ms QTc: Men < 440 ms, Women < 460 ms

Seven Step Approach n n n n Rate Rhythm Axis Intervals Hypertrophy ST/Tw changes, Q waves Conduction system
+Sw(V 3)>24 mm (male) >20 mm (female)")
n Left Ventricular Hypertrophy Cornell +R (a. VL)+Sw(V 3)>24 mm (male) >20 mm (female) n Sokolow S(V 1) + R(V 5)=32 mm n Rw (a. VL)>11 mm n Rw (I)>14 mm n

n Right Ventricular Hypertrophy n n n n 1. RAD>100* 2. IRBBB 3. R>S V 1 4. R<S V 6 5. R in V 1>=7 mm 6. R V 1 + S V 5 or V 6 >=10 mm 7. RAE 8. strain pattern in rt precordial leads

Seven Step Approach n n n n Rate Rhythm Axis Intervals Hypertrophy ST/Tw changes, Q waves Conduction system

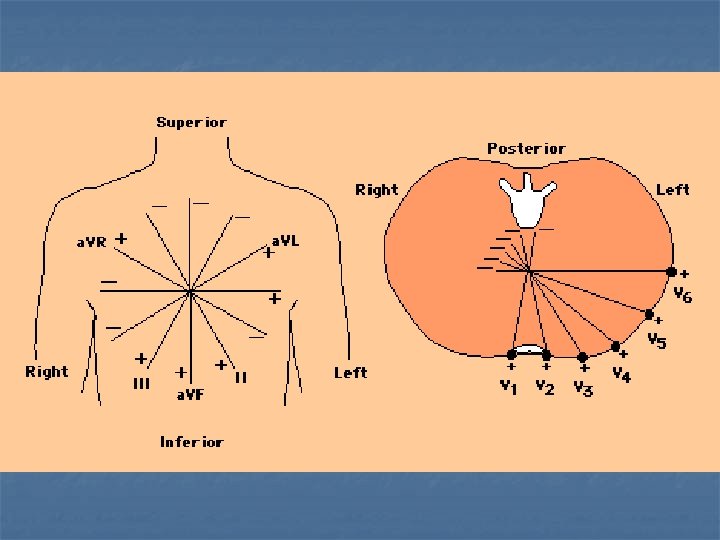
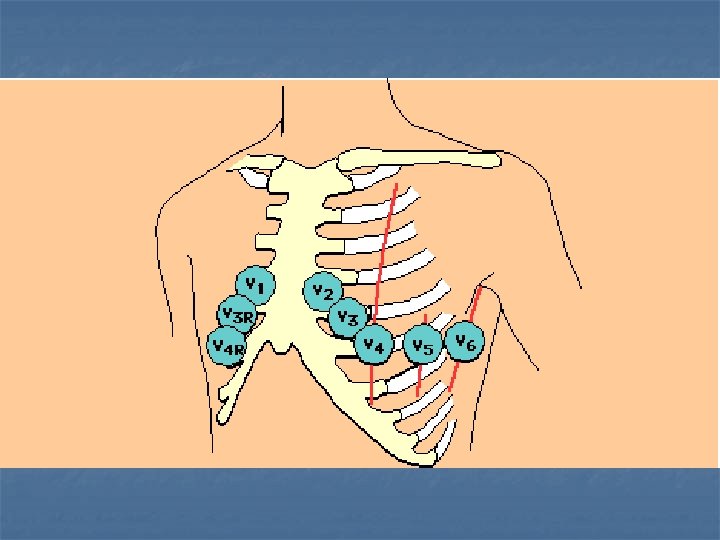
ANATOMICAL LOCALIZATION ANTERIOR: V 1 -V 4, SEPTAL V 1 -V 2 LATERAL: V 5 -V 6, I, Avl INFERIOR: II, III, a. VF

Seven Step Approach n n n n Rate Rhythm Axis Intervals Hypertrophy ST/Tw changes, Q waves Conduction system
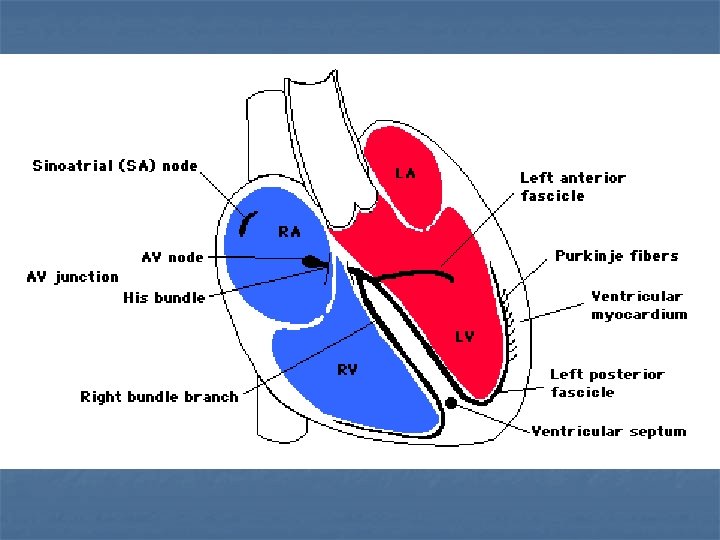
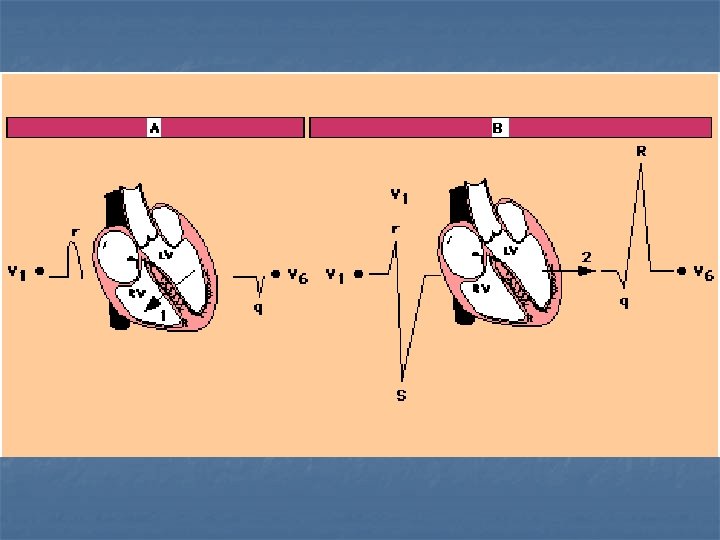

n LBBB n n n Left Anterior Fascicular Block n n LAD > -30', + I, a. VR, -II/III/a. VF q. R in I and L r. S in II, III and a. VF Left Posterior Fascicular Block n n QRS > 0. 12 sec wide monophasic R in I, V 5 and V 6 (usually notched or slurred) no Q in I, V 5 and V 6 RAD > 100' small R in I and a. VL, Q in II, III, a. VF S 1 Q 3 pattern RBBB n n n QRS>0. 12 sec R' > r in right precordium wide S in I, V 5 and V 6

Normal Variants- Juvenile Tw inversions

Nuts and Bolts

Electrode Misplacement

Amplitude Artifact

Parkinson’s Tremor

CASES

Case 1: 21 yo presents for routine physical exam

DEXTROCARDIA

Case 2: 38 yo with one week of URI presents with chest pain

Acute Pericarditis n n n Stage I--ST elevation, Tw upright, PR depression Stage II--ST baseline, flattened Tw Stage III--inv Tw Stage IV--Tw baseline, days to wks

Case 3: 48 yo homeless man found unresponsive

Hypothermia

Case 4: 34 yo ESRD missed three days of dialysis

Hyperkalemia

Case 5: 28 yo woman s/p neck surgery

Hypocalcemia

Case 6: 32 yo female on antidepressants had syncope

Acquired Long QT Syndrome

Case 7: 60 yo man with chest pain

Inferior MI with RV infarction and 2: 1 and complete heart block

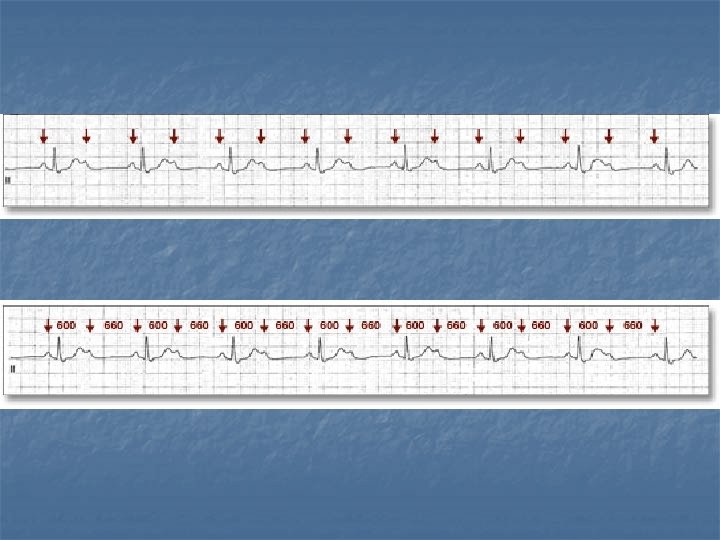
2: 1 Heart block with ventriculophasic effect

Case 8: 80 yo man with syncope

Aflutter with complete heart block Aflutter with normal conduction

Aflutter with 1: 1 conduction

Aflutter with carotid sinus massage

Counter-clockwise Aflutter

Clockwise Aflutter

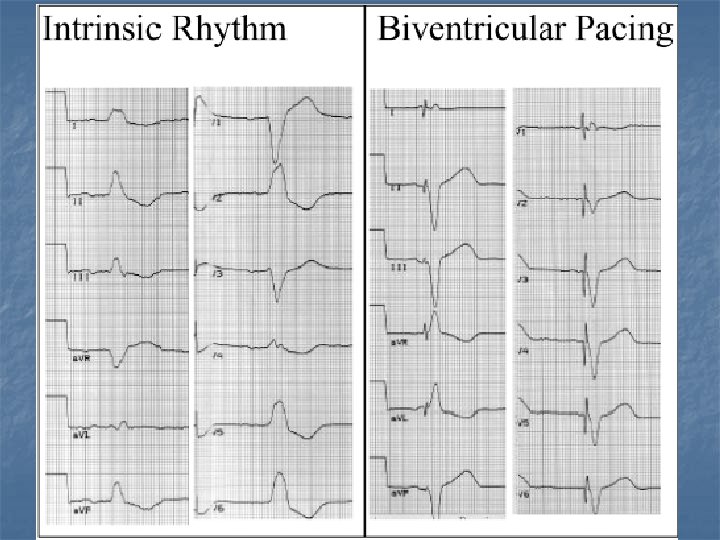
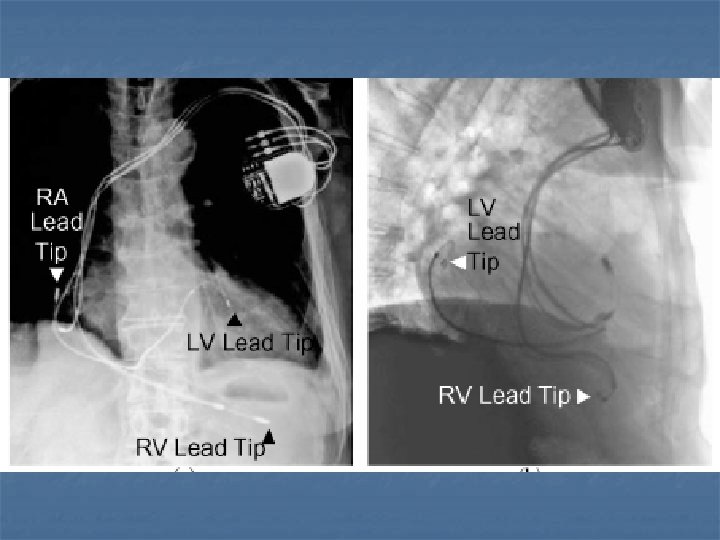
Case 9: 50 yo man with DCM

Biventricular pacing

Case 10: 25 yo man with palpitations

Pre-excited Atrial Fibrillation- right sided postero-septal pathway

Wolf-Parkinson-White: Left anterolateral pathway

Postero-septal pathway pre-ablation

Post-ablation with repolarization abn due to memory effect

Case 11: 25 yo female with lightheadedness
")
AV Node Re-entrant Tachycardia (AVNRT)

Case 12: 75 yo man with ischemic DCM and syncope

Ventricular Tachycardia n n n BRUGADA'S CRITERIA- Circulation '91 1. Absence of all RS complex in all precordial leads S 21%, SP 100% 2. R to S interval > 100 ms in one precordial lead S 65%, SP 98% 3 A-V Dissociation, fusion, capture beats S 82%, SP 98% 4. Morphologic criteria in V 1+2, 6

Ventricular Tachycardia

Ventricular Tachycardia: AV dissociation, RS >100 ms

Case 13: 18 yo Asian man with family history of SCD presents with syncope

Brugada Syndrome n n Genetic mutation in SCNA 5 Predominantly in Asian males Syncope and sudden cardiac death Three types

Brugada’s Type II- Saddle back

Case 14: 28 yo man with syncope
")
Arrythmogenic Right Ventricular Dysplasia (ARVD)

Case 15: 28 yo man with syncope

Short-coupled Torsades

Case 16: 34 yo woman with fatigue, weight gain, and abn menstrual period

Myxedema

Case 17: 84 yo man with skipped beats

Sino-atrial exit block Type I

Case 18: 64 yo woman presents for routine exam

Retrograde concealed conduction into the AV node
- Slides: 80