Interpretation and utility of ammonia level in Hepatic

 and its pathophysiology •")


 Minimal to Grade I (covert HE) • Grade 1:")
 • • Fluid and electrolyte")


 Labs • LFT’s • BUN/creatinine •")





 • -T/F:")




: 643")




- Slides: 29
Interpretation and utility of ammonia level in Hepatic Encephalopathy Patrick Fleming, MD Henry Ford EM; PGY-3
Goals and Objectives • Review definition/classification of hepatic encephalopathy (HE) and its pathophysiology • Review differential diagnosis, clinical/laboratory findings, and management of HE • Review of literature to make an evidence based assessment of utility testing for ammonia level in diagnosis and management of HE
Hepatic Encephalopathy • “HE is a brain dysfunction caused by liver insufficiency and/or PSS; manifests as a wide spectrum of neuropsychiatric abnormalities ranging from subclinical alteration to coma”
Classification of HE • Type A - due to acute liver failure • Type B - predominantly from portosystemic bypass or shunting • Type C - due to cirrhosis
Severity Classification (West Haven Criteria) Minimal to Grade I (covert HE) • Grade 1: some cognitive changes, euphora/anxiety, shortened attention span, impairment in calculations, or altered sleep—clinical findings usually not reproducible Grade II-IV (overt HE) • Grade II: lethargy/apathy, disoriented to time, personality change/inappropriate behavior, asterixis • Grade III: somnolent but responsive to stimuli; confused, disoriented (to time and space), bizarre behavior • Grade IV: coma, unresponsive to painful stimuli
Precipitating Factors (factor unknown in 20 -30% of cases) • • Fluid and electrolyte disturbances Renal failure Infection GI bleed Sedatives High protein diet Constipation
History and Physical Presenting complaint • AMS, flapping tremor, mood and behavior changes Physical Exam • Look for stigmata of cirrhosis: • Neurologic findings: see HE severity scale • Asterixis: elicited bilateral flapping tremor
Differential Diagnosis • Metabolic encephalopathies: CO 2 narcosis, DKA, hypoglycemia, hypoxia • Toxic encephalopathies: alcohols, narcotics, benzodiazepine • Intracranial event: infection, head injury, tumor, ICH, stroke • Pyschiatric
Testing (for rule-out of other conditions in differential) Labs • LFT’s • BUN/creatinine • Electrolytes • Glucose • ETOH level • Urine toxicology • ABG • Pt/ptt/inr • Ammonia? Imaging • CT or MRI head
Ammonia and HE Friedrich von Frerichs Time line of theory: 1879: Friedrich von Frerichs amongst the earliest commentators on Hepatic Encephalopathy 1893: Hahn et al working in Pavlov’s lab report findings of intoxication following meat feeding in dogs that had undergone Eck fistula 1932: Van Caulaert and Deviller show high ammonia levels in patients with liver disease, increase in levels after given ammonia salts, and induction of neuropsychiatric symptoms in many of their patients 1936: Kirk’s experimentation of administration of ammonia to cirrhotic patients 1958, 1963: studies by Sherlock and Stahl show in general as ammonia level increase severity of HE increase
Pathogenesis Common theory • Nitrogenous compounds from GI tract adversely affect brain function Build up of nitrogenous compounds from: • Decreased hepatic function • Porto-systemic shunts Elgouhari HM, O’Shea R. What is the utility of measuring the serum ammonia level in patients with altered mental status? Cleve Clin J Med. 2009; 76(4): 252 -254
Ammonia and HE
• A 57 yo patient presents to ED with known alcoholic cirrhosis with altered mental status. Family states for last day he has been less active, is sleeping much of day, and seems confused. On exam patient is disoriented and drowsy. You note stigmata of cirrhosis and are able to elicit asterixis.
• Q: How many in the audience would obtain an ammonia level in the work-up of this patient?
• -T/F: a normal ammonia level can rule out HE (sensitivity) • -T/F: an elevated ammonia level can establish the diagnosis of HE (specificity) • -T/F: serial ammonia levels are useful in assessing response to therapy for HE
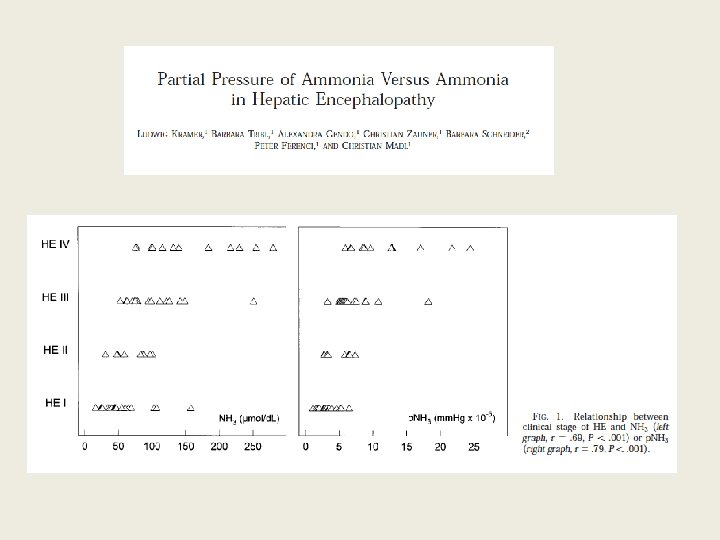
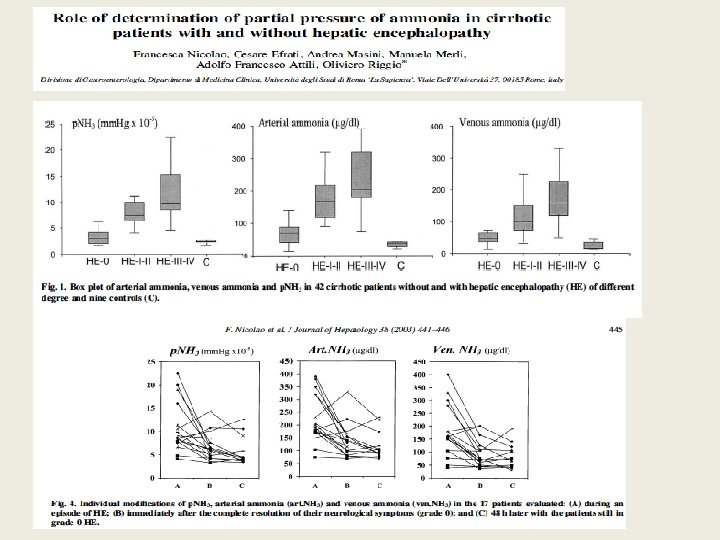
• Value of ammonia level still debated • No clear advantage to source of sample (venous vs. arterial vs. partial pressure) • Would ultimately like to know rate of diffusion of ammonia across blood brain barrier (and the variables that alter this)
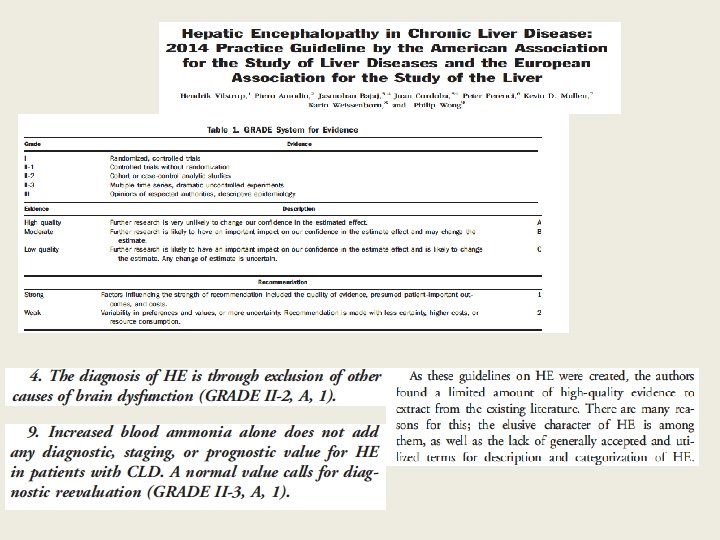
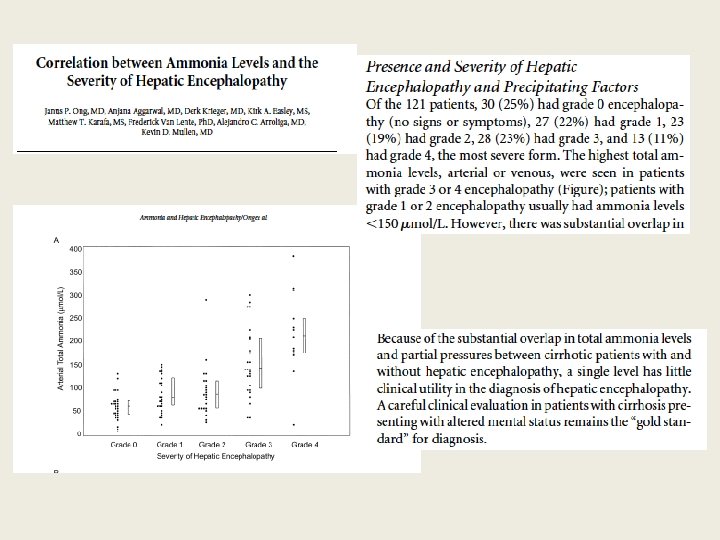
Ammonia levels in HE • Normal levels do not rule out HE • In one study more than 69% without evidence of HE had elevated levels • Neither sensitive or specific for presence or degree of HE • Evidence for having special prognostic value in patient with acute liver failure
Technical aspects of ammonia level testing • Venous blood level as reliable as arterial if obtained and handled properly • Prolong use of tourniquet or fist-clenching false elevation • Venous blood should be transported on ice and handled quickly for analysis • A serum ammonia assay is $27. 07 (2013 Medicare reimbursement)
Dangers of ammonia interpretation • Improper technique can lead to falsely elevated levels • Measurement in patient without signs of HE can lead to improper treatment • Over-reliance on elevated level can lead to anchoring on diagnosis
From: Serum Ammonia Level for the Evaluation of Hepatic Encephalopathy JAMA. 2014; 312(6): 643 -644. doi: 10. 1001/jama. 2014. 2398 Table Title: Laboratory Test Results in a Patient With Hepatitis C Cirrhosis Date of download: 12/1/2015 Copyright © 2015 American Medical Association. All rights reserved.
Treatment • • Identify and correct precipitating factor Maintain nutrition: protein intake 1. 2 -1. 5 g/kg/day Lactulose: 25 m. L q 1 hour until defecation, then 15 -45 m. L q 8 -12 for 2 -3 soft stools daily Rifaximin: 500 mg PO BID
Disposition • Disposition: Consider underlying cause, response to therapy. Grade 1 without complicating factors may possible be discharged. Grade III-IV likely need ICU.
Summary • A normal ammonia level cannot rule out HE • An elevated ammonia level cannot establish the diagnosis of HE • Serial ammonia levels does not currently have role in assessing response to therapy for HE • HE is a clinical diagnosis; focus on excluding other causes of AMS
References • • • Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014 Aug; 60(2): 715 -35 Elgouhari HM, O’Shea R. What is the utility of measuring the serum ammonia level in patients with altered mental status? Cleve Clin J Med. 2009; 76(4): 252 -254 Kramer, L. , Tribl, B. , Gendo, A. , Zauner, C. , Schneider, B. , Ferenci, P. , and Madl, C. (2000). Partial pressure of ammonia versus ammonia in hepatic encephalopathy. Hepatology 31 (1): 30 -34. Ong, J. P. , Aggarwal, A. , Krieger, D. , Easley, K. A. , Karafa, M. T. , Van Lente, F. , Arroliga, A. C. , and Mullen, K. D. (2003). Correlation between ammonia levels and the severity of hepatic encephalopathy. Am. J. Med. 114 (3): 188 -193. Stahl, J. (1963). Studies of the blood ammonia in liver disease: Its diagnostic, prognostic, and therapeutic significance. Ann. Int. Med. 58: 1 -24. Lockwood AH. Blood ammonia levels and hepatic encephalopathy. Metab Brain Dis 2004; 19: 345349. Nicolao F, Efrati C, Masini A, et al. Role of determination of partial pressure of ammonia in cirrhotic patients with and without hepatic encephalopathy. J Hepatol. 2003, 38 (4): 441 -446 Wang V, Saab S. Ammonia levels and the severity of hepatic encephalopathy. Am J Med 2003; 114: 237 -8. Bhatia V, Singh R, Acharya SK. Predictive value of arterial ammonia for complications and outcome in acute liver failure. Gut. 2006; 55(1): 98 -104. Lockwood AH, Yap EWH, Wong W-H. Cerebral ammonia metabolism in patients with severe liver disease and minimal hepatic encephalopathy. J Cereb Blood Flow Metab 1991; 11: 337 -341.