INTERNS GUIDE TO SEPSIS SPECTRUM Adam Hayek PGY


 SEVERE SEPSIS (SEPSIS +")

 <36°C(96. 8°F)")

 (>100. 9°F) Hypothermia (core temperature")
 Leukopenia")

 Acute oliguria")
 Decreased capillary refill or mottling")

 Draw appropriate")


 for : � Neutropenic patients")





 Do not use")


 Norepinephrine is first choice")
 Vasopressin dose more")




 if Scv.")
: � Plt count <10, 000")
")
")

: � Arousable �")

: � When 2 consecutive BS >180 �")


 � Daily sc low")

 feeding within 48 hours")

- Slides: 46
INTERN’S GUIDE TO: SEPSIS SPECTRUM Adam Hayek PGY 3
Objective Identification � Classification � Management � �Importance of timely delivery of care Escalation of care � Importance of early goal directed therapy (EGDT) �
Sepsis Spectrum � � � SIRS SEPSIS (SIRS+ proven/probable infection) SEVERE SEPSIS (SEPSIS + acute organ dysfunction) SEPTIC SHOCK (SEPSIS + hypotension not reversed with fluid resuscitation) DEATH (25%)
WHAT IS SIRS?
1992 Identify: SIRS � Systemic Inflammatory Response System � Fever >38°C(100. 4°F) <36°C(96. 8°F) � Heart Rate >90 BPM � Tachycardia RR >20 p. CO 2 <32 mm. Hg � WBC >12, 000 cells/mm³ <4000 cells/mm³ > 10% bands � 2 or More SIRS Criteria= Go hunting for infection � � BCx 2, CXR, UA/UC If infection found or suspected= SEPSIS
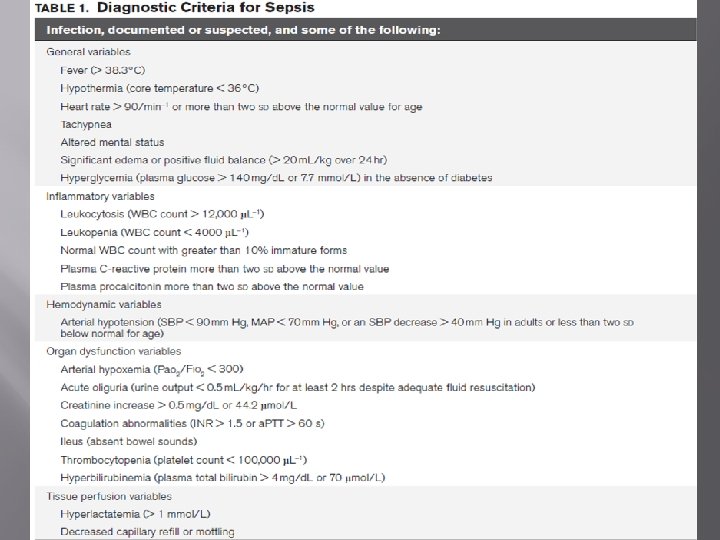
Who Are We Missing? � � � � � 2012 Surviving Sepsis Campaign Updates 1992 criteria was not sensitive enough Allows physician to account for more variables Patients don’t always decompensate in linear fashion Importance of early detection Early goal directed therapy Allowed more variables to consider when deciding SEPSIS Patient “Toxic Appearing” Definitions “Sepsis is the clinical syndrome that results from a dysregulated inflammatory response to an infection” � Probable or documented infection with SOME of the following: �
General variables � � � Fever (> 38. 3°C) (>100. 9°F) Hypothermia (core temperature < 36°C) Heart rate > 90/min OR 2 SD above age normal Tachypnea Altered mental status Significant edema or positive fluid balance �> � 20 m. L/kg over 24 hr Hyperglycemia > 140 mg/d. L without diabetes
Inflammatory variables � � � Leukocytosis (WBC count > 12, 000 µL– 1) Leukopenia (WBC count < 4000 µL– 1) Normal WBC count with greater than 10% immature forms CRP > 2 SD above normal PCT > 2 SD above normal
Hemodynamic variables � Arterial hypotension � SBP < 90 mm Hg, MAP < 70 mm Hg Or � SBP decrease > 40 mm Hg in adults Or �< 2 SD below normal
Organ dysfunction variables � � Arterial hypoxemia (Pao 2/Fio 2 < 300) Acute oliguria � UO < 0. 5 m. L/kg/hr for at least 2 hrs � Despite adequate fluid resuscitation � � � Creatinine increase > 0. 5 mg/d. L Coagulation abnormalities INR > 1. 5, a. PTT > 60 s Ileus (absent bowel sounds) Thrombocytopenia (platelet count < 100, 000 µL– 1) Hyperbilirubinemia (Total bilirubin > 4 mg/d. L
Tissue perfusion variables � � Hyperlactatemia (> 1 mmol/L) Decreased capillary refill or mottling
YOU’VE DETERMINED PROBABLE SEPSIS Now What?
Initial Screening � � � Routine screening for potential infection (1 C) Draw appropriate cultures (antibiotics can be delayed only up to 45 min for this) (1 C) Draw 2 sets of BC ( at least one peripheral and one central if line placed >48 hrs ago) If invasive candidiasis suspected: 1, 3 B glucan (2 B) and galactomannan antibodies (2 C) Prompt imaging studies to confirm source of infection (UG)
Time-bound delivery care Get good PIV access 2 < 18 gauge
Which Antibiotic? � � Administration of antibiotics within 1 hour of onset of severe sepsis (1 C) and septic shock (1 B) One or more antibiotics that will have activity and penetration against likely pathogens (1 B) Reassess antibiotic regimen for de-escalation (1 B) Use Procalcitonin to guide de-escalation (2 C)
Special Antibiotics Consideration � Combination antibiotics therapy (2 B) for : � Neutropenic patients � Multidrug resistant bacteria High risk of resistant �gram negatives, acinetobacter, pseudomonas � Pseudomonas bacteremia �B � lactam + Aminoglycoside or fluoroquinolone ( 2 B) Strep pneumonia bacteremia �B lactam + macrolide (2 B)
Duration of antibiotics � � Continue combination for 3 -5 days then deescalate to appropriate (2 B) Total antibiotics 7 -10 days, except: (2 C) � Unresolved clinically � S. aureus bacteremia � undrainable focus of infection � viral/fungal sepsis � immunocompromised or neutropenic � Initiate antivirals as early as possible when indicated (2 C)
Source control � � � Establish anatomic diagnosis of infection source and intervene <12 hours (1 C) Infected peripancreatic necrosis- delay intervention till demarcation develops (2 B) Intervention should be percutaneous when possible ( IR instead of surg) (UG)
WHERE DOES THE PATIENT BELONG General Medical Floor vs Medical Intensive Care Unit
Severe Sepsis
Initial Resuscitation � � � Central venous pressure 8 -12 cm Mean arterial pressure ≥ 65 mm Urine output > 0. 5 ml/kg/hr Central venous saturation > 70% or mixed venous saturation > 65% (1 C) If lactate elevated: normalize lactate
Fluid therapy � � � Crystalloids are initial therapy (1 B) Do not use Hydroxyethyl starches (1 B) Use albumin only when substantial amounts of crystalloids are needed (1 C) Minimum of 30 ml/kg bolus of crystalloids initially Continue fluid administration until hemodynamic improvement occurs (UG)
INITIAL RESUSCITATION: EGDT Rivers, E, et al. NEJM 2001
EGDT
Vasopressors � � Target mean arterial pressure of 65(1 C) Norepinephrine is first choice of vasopressors(1 B) Add epinephrine when additional agent required (2 B) Vasopressin can be added at 0. 03 units/min for raising MAP or reducing dose of NE (UG)
Vasopressors � � Do not use vasopressin as single agent (UG) Vasopressin dose more than 0. 04 units/min not recommended (UG) Dopamine used only in selected patientsbradycardia and low risk for tachyarrhythmias (2 C) Phenylephrine to be used as salvage therapy, serious tachyarrhythmias, good cardiac output (1 C)
Vasopressors � � � Low dose dopamine should not be used for “renal protection” (1 A) Place an arterial catheter as soon as practical in patients requiring vasopressors (UG) Trial of dobutamine up to 20 mcg/kg/min in patients with documented low cardiac output/high filling pressures � First 6 hours with hypoperfusion despite adequate fluids and MAP (1 C)
Steroids in shock � � Use hydrocortisone if persistent hemodynamic instability despite fluids and vasopressors (2 C) Do not use the ACTH stimulation test (2 B) Taper steroids when off the vasopressors (2 D) Steroids should not be used in the absence of shock (2 D)
So much more to know… � � � � Transfusion in Sepsis Mechanical Ventilation Management Sedation and NM blockade Glucose Control Renal Replacement therapy Nutrition Stress ulcer prophylaxis Discuss goals of care
Questions? � � Have fun Ask questions Keep reading Don’t accept anecdotes at face value � Look up � Find supporting literature
Transfusion in severe sepsis � � In first 6 hours ( EGDT) if Scv. O 2 <70 despite adequate MAP and CVP, and HCT <30 In absence of active bleeding, active myocardial ischemia, transfuse only if Hb <7 gm/dl to target of 7 -9 gm /dl (1 B) Do not use erythropoietin (1 B) in severe sepsis to treat anemia Do not use blood products ( FFP) to treat lab abnormalities ( prolonged INR) in absence of bleeding or planned procedures (2 D)
Transfusion in severe sepsis � Platelet transfusion (2 D): � Plt count <10, 000 /mm 3 � Plt count <20, 000 /mm 3 and risk for bleeding is high � Plt count <50, 000 and bleeding or needs procedures Do not use: antithrombin (1 B), activated protein C, iv immunoglobulins (2 b)
Mechanical Ventilation � � � 6 ml/kg predicted body weight tidal volume (1 A) Maintain plateau pressures ≤ 30 cm in ARDS(1 B) Apply PEEP to avoid alveolar collapse (1 B) Head of bed elevation 30 -45 degrees (1 B) Appropiate use of NIPPV in acute hypoxic respiratory failure (2 B)
Mechanical Ventilation � Severe ARDS ( Pa. O 2/Fi. O 2 <100 mm Hg) � Recruitment manouver (2 C) � Prone positioning (2 B) in experienced facilities � Avoid � Pulmonary artery catheters (1 A) � Liberal fluid strategy(1 C) in absence of hypoperfusion � B 2 agonists in absence of bronchospasm (1 B)
ARDS-NET protocol
Mechanical Ventilation � Weaning protocols in place for SBT (1 A): � Arousable � Hemodynamically stable � No new potentially serious condition � Low ventilatory and Fi. O 2 requirements � Consider extubation if above conditions are met
Sedation and NM blockade � � � Minimize sedation targeting specific titration endpoints (1 B) Avoid neuromuscular blocking agents in absence of ARDS (1 C) For severe ARDS short course of NMB agents may be used for upto 48 hours for hypoxia (2 C)
Glucose control � Protocolized approach (1 A): � When 2 consecutive BS >180 � Target upper BS level ≤ 180 � Check BS 1 -2 hrs till BS and insulin infusions are stable , then q 4 hours (1 C) � Point of care BS may not be as accurate as plasma glucose (UG)
Renal replacement therapy � � Continuous renal replacement therapy and intermittent hemodialysis are equivalent (2 B) Use continuous renal replacement therapy for better fluid management in hemodynam ically unstable patients (2 D)
Stress Ulcer Prophylaxis � � � H 2 blockers or proton pump inhibitors should be used in patients at risk for Upper GI bleeding (1 B) Proton pump inhibitors used rather than H 2 blockers (2 D) In absence of risk factors, do not use prophylaxis (2 B)
Prophylaxis � Daily pharmacoprophylaxis in sepsis against VTE (1 B) � Daily sc low molecular weight heparin (1 B) � Unfractionated heparin sc bid (1 C) or tid � If creatinine clearance <30 ml/min, use deltaparin (1 A) or Unfractionated heparin (1 C) � Severe sepsis: combination of pharmacological therapy and intermittent pneumatic compression devices (2 C)
Prophylaxis � Contraindications to use of pharmacological prophylaxis: � Intracerebral hemorrhage � Active bleeding � Severe coagulopathy � Thrombocytopenia � Use intermittent pneumatic compression devices (2 C)
Nutrition � � Start oral or enteral ( if necessary) feeding within 48 hours for patients admitted with severe sepsis (2 C) Avoid full dose feeding in first week, use low dose (500 cal/day advancing only as tolerated) (2 B) Use iv glucose or enteral feeding instead of total parental nutrition in first week (2 B) Do not use specific immunomodulating supplementation (2 C)
Goal clarification � � Discuss goals of care and prognosis with patients and families (1 B) Incorporate goals of care and end of life care planning into treatment Use palliative care when appropriate (1 B) Address goals of care within 72 hours of ICU admission (2 C)