INTERN SEMINAR Severe Bradycardia During Cesarean Section Ri

INTERN SEMINAR: Severe Bradycardia During Cesarean Section Ri 黃哲南 & Ri 陳雅茹

Brief History 36 -year-old Korean woman n Height: 165 cm Weight: 83. 6 kg n GA 37 weeks, admitted for scheduled C/S n Regular examination revealed a healthy pregnancy n ¨ no hypertension ¨ no gestational diabetes mellitus (GDM)

Obs / Gyn History n G 5 P 3 SA 1 ¨ P 1: NSD ¨ P 2: C/S due to placenta previa ¨ P 3: C/S due to prior C/S Menarche: 13 y/o n Interval / Duration: 28 days / 4 days n LMP: 93/8/24 n EDC: 94/5/25 n

Past History Deny any systemic disease n Previous OP history: C/S X 2, both were uneventful n Smoking: nil n Alcohol consumption: nil n Drug or food allergy: denied n

Physical Examination Consciousness: clear and alert n T/P/R: 36. 4℃ / 100 / 20 n HEENT: grossly normal n ¨ Conjunctiva: not pale Sclera: anicteric Neck: supple, no LAP, JVE or goiter n Chest: symmetrical expansion, clear BS n Heart: RHB, no audible murmur n Abdomen: ovoid, normoactive Bo. S n Extremities: freely movable, no cyanosis n

Laboratory Examination Date RBC Hb PLT WBC Band Seg Eos 5/3 4. 38 11. 1 274 7. 57 0 71. 7 3. 3 Date BUN Cre Alb AST ALT 3/16 10. 1 0. 7 3. 93 23 6 Date Na K Cl Ca 3/16 136 4. 1 105 1. 95 Date PT INR PTT 3/16 11. 6 0. 98 29. 2

Clinical Course Pre-anesthetic evaluation was unremarkable n Classified as ASA class 1 n

Clinical Course C/S was performed on May 4 under spinal anesthesia n A male baby, weighed 3114 gm, was delivered smoothly n Uterus was pulled out, and a huge myoma was noted at the fundus of uterus n
")
Clinical Course Progressive bradycardia and loss of consciousness were noted (slowest HR was 20/min) n NIBP was un-measurable n CPR was started n Near-asystole had been shown by ECG during resuscitation n
 and epinephrine (0. 05 mg) were given intravenously n")
Clinical Course Atropine (1 mg) and epinephrine (0. 05 mg) were given intravenously n Vital signs became stable within minutes, and consciousness was regained gradually n No more hemodynamic unstability developed during the remained operation n ABG n p. H=7. 461 HCO 3=16. 0 n Pa. CO 2=22. 4 BE=5. 6 Pa. O 2=284. 2 Estimated blood loss was 400 m. L

Clinical Course Sent to 4 FI for further close observation n Cardiologist was consulted n

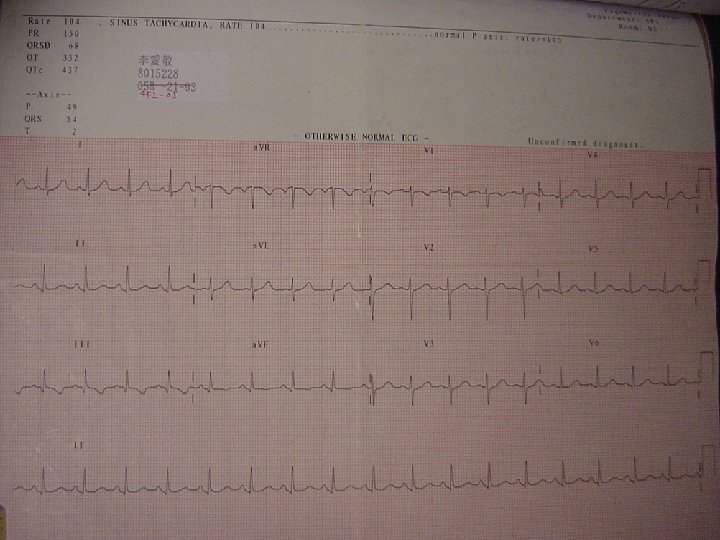
Clinical Course n Cardiologist consultation ¨ PE: same as admission evaluation ¨ EKG: Sinus tachycardia (HR=104/min) n Non-specific ST-T change at lead III and a. VF n ¨ Echocardiography: n Good LV contractility (LVEF=72%) n Mild TR (PG=28 mm. Hg) n Mild MR n No chamber dilatation ¨ Impression: Vasovagal reflex

Clinical Course No cardiac event occurred in 4 FI, so she was transferred to 5 B on May 5 n The following admission course was uneventful, and she discharged on May 9 (Post OP Day 5) n

Discussion

Differential Diagnosis

High spinal block and spinal induced sympathectomy n Massive hemorrhage n Amniotic fluid embolism n Pulmonary embolism n Myocardial infarction n Bezold-Jarisch reflex & Vasovagal reflex n

Bezold-Jarisch Reflex

Clinical Relevance of the Bezold–Jarisch Reflex Anesthesiology 2003; 98: 1250– 60

n 1867: Bezold and Hirt ¨ Veratrum alkaloid ¨ Hypotension, bradycardia, apnea n Definition of Bezold-Jarisch reflex: ¨ By Dawes in 1947 ¨ Hypotension, bradycardia, peripheral vasodilation Clinical Relevance of the Bezold–Jarisch Reflex Anesthesiology 2003; 98: 1250– 60

Anesthesiology 2003; 98: 1250– 60

Anesthesiology 2003; 98: 1250– 60

Anesthesiology 2003; 98: 1250– 60

Anesthesiology 2003; 98: 1250– 60

Vasovagal Reflex

Stimulus Afferent pathway Efferent response Higher centers Pain, Emotion Pancreatic polypeptide Carotid sinus IX Medullary vasomotor center Carotid sinus sensitivity Vagus nerve + + Bradycardia Aortic baroreceptors Ventricular afferents Decreased Venous return Unmyelinated ‘c’ fibers. Respond to chemical and mechanical stimuli. Enhanced activation by β 2 receptor stimulation. Other viscera e. g. bladder Sympathetic NE Vasodilation in resistance vessels Epinephrinevasodilation + Adrenal in skeletal gland muscles British Journal of Anaesthesia 86(6): 859 -68 (2001)

n Causes ¨ Hemorrhage ¨ Orthostasis ¨ Compression of inferior vena cava during pregnancy ¨ Regional anesthesia British Journal of Anaesthesia 86(6): 859 -68 (2001)

n The current pathophysiological hypothesis for such vasovagal episodes holds that a rapid preload reduction causes an abnormally elevated inotropic response, due to an exaggerated catecholamine release. Chest Volume 117(6) June 2000; pp 1801 -1803 Stroke Volume 29(11) November 1998 ; pp 2347 -2351

n The increase in myocardial contractility in the setting of a preload reduction activates cardiac mechanoceptors, mediating via the brain stem an abnormal enhancement of parasympathetic activity, together with a sympathetic withdrawal. Chest Volume 117(6) June 2000; pp 1801 -1803 Stroke Volume 29(11) November 1998 ; pp 2347 -2351

Management

Restoration of venous return Head-down tilt or leg elevation n Compression of the vena cava should be relieved in obstetric cases n If hypovolemia was considered, IVF should be given n British Journal of Anaesthesia 86(6): 859 -68 (2001)

Medication: n Anticholinergic drugs: ¨ Atropine n Not be the best single agent if bradycardia is suspected to be accompanied by vasodilation n Sympathomimetic drugs: ¨ Ephedrine n Direct sympathetic effects on the heart rate ¨ Epinephrine British Journal of Anaesthesia 86(6): 859 -68 (2001)

n Thump pacing for asystole ¨ Prompt treatment with epinephrine has been emphasized as crucial for successful recovery ¨ Epinephrine may be necessary during cardiac arrest in association with high spinal anesthesia ¨ For asystole or persistent severe bradycardia, epinephrine should be used early British Journal of Anaesthesia 86(6): 859 -68 (2001)

Thank you for your attention!
- Slides: 36