INTERHOSPITAL CONFERENCE 21 DEC 2007 Physical examination Thai






































- Slides: 44
INTER-HOSPITAL CONFERENCE 21 DEC. 2007
Physical examination • Thai male, not pale, no jaundice • v/s T 37˚C PR 80/min BP 120/80 mm. Hg • Heart : normal • Lung : clear • Abdomen : soft, not tender, no hepatomegaly • Neuro sing : WNL
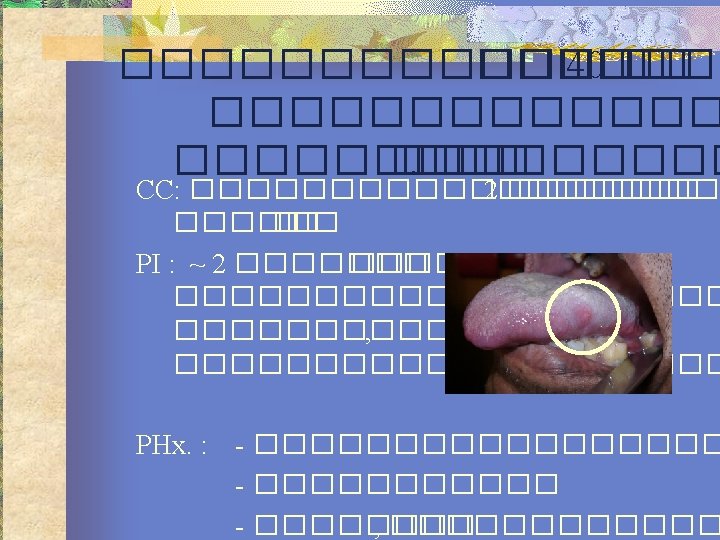
ENT Examination • AR : normal mucosa, no discharge • PR : no mass, no discharge • OC : ulcerative lesion at Lt. lateral tongue size 0. 5 x 0. 5 cm. • IDL : no mass, TVC move bilateral • Neck : no palpable lymph node
Management?
BIOPSY : Negative for malignancy
DIFFERENTIAL DIAGNOSIS
ENT Examination • OC : ulcerative lesion at Lt. lateral tongue size 0. 5*0. 5 cm. , submucosal lesion 2*3 cm. , no limited tongue movement
INVESTIGATION
INVESTIGATION • A. • B. • C. • D. • E.
DIAGNOSIS AND MANAGEMENT
DIAGNOSIS
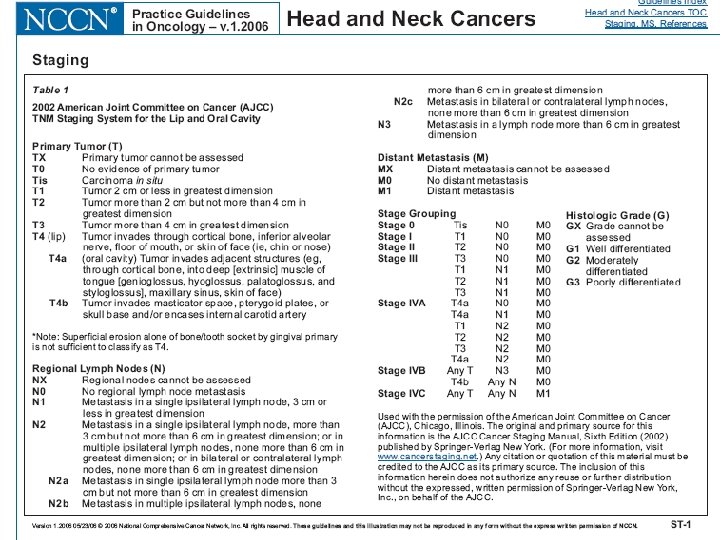
DIAGNOSIS • CA Tongue T 2 N 0 M 0
MANAGEMENT • Surgery? • RT?
MANAGEMENT • Surgery? • RT? Wide excision?
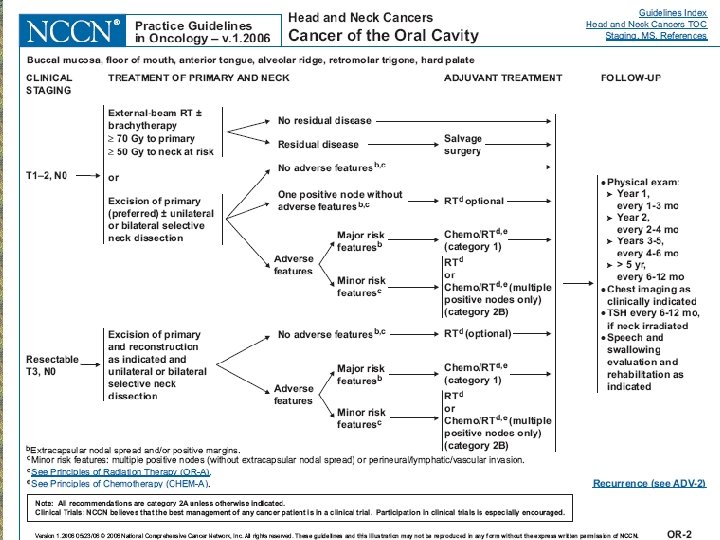
DIAGNOSIS AND MANAGEMENT • Dx. CA Tongue T 2 N 0 M 0 • Rx. Lt. Hemiglossectomy with primary closure with Lt. SND I-IV
Surgical Pathology Report • Tongue : consists of Lt. half portion of tongue, measuring 5*3*2. 5 cm. The outer surface reveals an ulcerated light tan firm mass, measuring 2. 7*1. 8*0. 8 cm. , occupying the Lt. half of tongue, 0. 5 cm. from medial resected margin and 0. 5 cm. from deep resected margin • Lymph node group I-IV : No evidence of malignancy
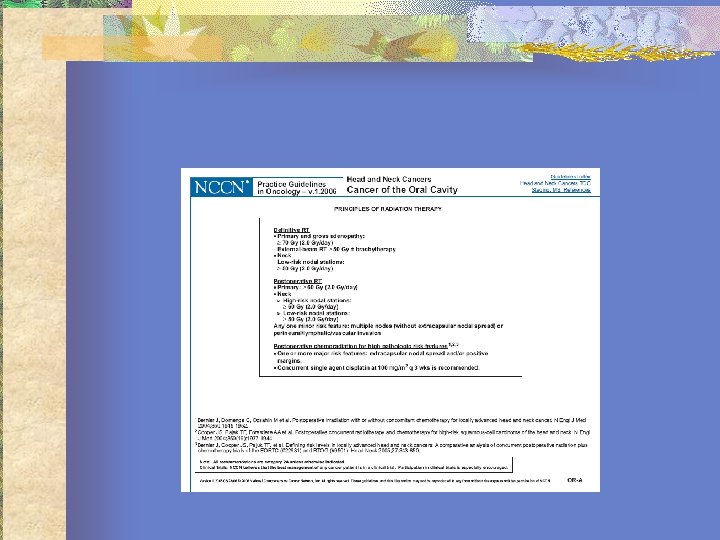
Management • Combine Post-Op. RT? • Combine Chemotherapy?
Management of the N 0 Neck in CA Oral cavity
Evaluation of the N 0 Neck • The reported false negative rate in assessing of cervical LN metastasis by palpation is 20%-50% • Factor affecting : • • • The experience of the examiner The patient’s body The previous treatment – Sx / RT
Evaluation of the N 0 Neck • Structure in neck mistake • Transverse process of atlas • Carotid bifurcation • Submandibular gland
Evaluation of the N 0 Neck • Digital palpation • CT / MRI • Ultrasound guided FNAB
Evaluation of the N 0 Neck • Malignancy criteria for CT/MRI • LN > 15 mm. in level II • LN > 10 mm. in other levels • Group of ≥ 3 nodes ( 1 -2 mm. ) • Central necrosis • Loss of tissue planes ( fat plane)
N 0 Neck affecting the recurrent/survival rate Oral cavity CA Type N 0 1 node 2 nodes ≥ 3 nodes 5 years survival 75% 49% 30% 15%
Therapeutic modalities for the N 0 neck • Prophylactic Neck dissection • Prophylactic Neck irradiation • Observation with therapeutic ND once regional metastasis become appearance
The N 0 neck in oral cavity CA • Byers et al : the prediction of nodal metas. In primary oral tongue SCCA • • • The depth of muscle invasion N stage The degree of differentiation of the 1˚ tumor • T 1 N 0 with muscle invasion < 4 mm. , WD 14% chance of nodal involvement
The N 0 neck in oral cavity CA • SCCA of oral cavity the sites with < 20% occult metastasis : • • • T 1/T 2 lip T 1/T 2 oral tongue < 4 mm in thickness T 1/T 2 FOM < 1. 5 mm in thickness
Surgical therapy in the N 0 neck with oral cavity CA • SOHND • Minimal morbidity • Reduces the risk of occult disease • Avoid the undesirable side effect of RT ( RT is reserved for possible future tx. of second primary tumor(
RT in the N 0 neck with oral cavity CA • An alternative treatment to SOHND • PORT of the surgically treated primary tumor site, the neck has not been dissected, and the risk of occult regional dz. is substantial • Primary tumor is treated with RT and the risk of occult node > 20%
Elective neck dissection VS Elective neck irradiation ENI reduced neck failure rate in pt with control primary tumor and N 0 neck from 18% to 1. 9% • In T 1 N 0 SCCA oral tongue, ENI provided 95% control rate for neck recurrences compare with 38% without ENI • Modality is chosen to Tx primary cancer may also help in formulating a decision as to how to tx the neck •
Elective neck dissection VS Elective neck irradiation • Prophylactic neck RT provides equal control rate for neck metastasis to prophylactic ND
THANK YOU FOR YOUR ATTENTION
Combined modality of treatment • perineural spread • intravascular spread • intralymphatic spread +ve margin • 2 histo. Positive LN • multiple +ve LN • extracapsular spread •
Management of contralateral N 0 • 14% incidence of involvement of contralateral neck node regardless of tumor stage • If primary oral cavity cancer is midline location, bilaterally, along the tip of tongue or approaches or cross the midline
BASIC LAB. • • CBC : Hct. 36% WBC 11, 200 ( N 72. 2% L 21% E 2. 1% M 3. 9%) BUN 5 Cr 0. 5 Na 137 K 4. 3 Cl 106 CO 2 25 FBS : 107 LFT : Alk. 59 SGPT 12 SGOT 17 TB 0. 63 TP 7. 8 Alb 4. 6 EKG : Normal CXR : No active pulmonaly lesion
BIOPSY. • Lt. Lateral tongue : Squamous cell carcinoma, moderate differentiated
N 0 in early SCCA oral cavity Most important prognostic factor in Mx of oral SCCA is status of cervical LN. • Present of metastasis to cervical LN can reduce curative rate by 50% • 3 Tx options are available. • • Observation with therapeutic ND once regional metastasis become appearance Elective neck RT Elective neck dissection
Morbidities of associated ENI • Xerostomia • Dsyphagia • Increased oral passage time • Mucositis • Pain • Increased complication if salvage sx. • Long duration of tx.