Interesting Case Submission BSGAR 2016 Sheep in Wolves

Interesting Case Submission BSGAR 2016 Sheep in Wolves’ Clothing
 james. burn 2@imperial. nhs. uk • Dr")
Authors • Dr James Burn (Sp. R) james. burn 2@imperial. nhs. uk • Dr Mary Roddie (Consultant) mary. roddie@imperial. nhs. uk

History #1 • Sudden onset breathlessness. • Chest pain • Referred for CTPA

CTPA • PE’s

CTPA • CT Abdomen and Pelvis recommended for further assessment of incidental parasplenic soft tissue mass.

CT AP + IV
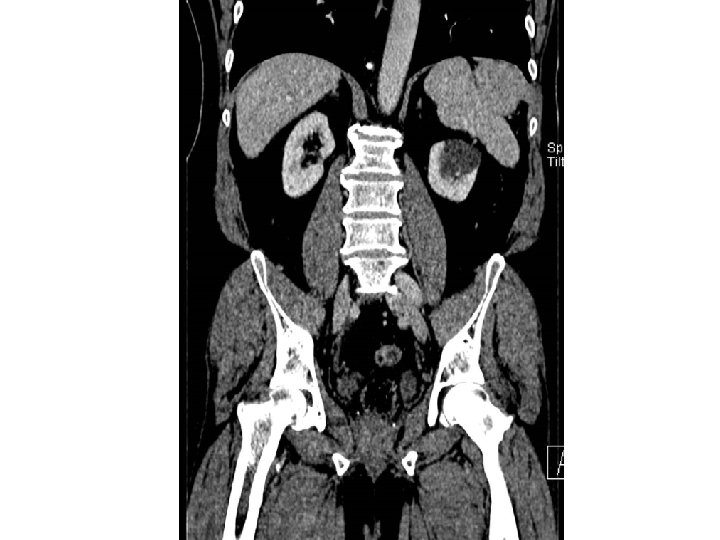

CT AP • Heterogenously enhancing, irregular soft tissue parasplenic mass. • Broad peritoneal contact. Separate from spleen. • Small volume of adjacent free fluid • ? peritoneal tumour deposit (solitary) • No primary demonstrated • US recommended for further assessment + biopsy. • PET for ? primary / other sites of peritoneal disease

US • Homogenous echotexture – similar to spleen. Smooth contour. Core Biopsy taken

Histology • Initial report inconclusive - ? abnormal liver tissue. ? Sarcomatous lesion. ? lung / liver origin. • Re-discussed at MDT – Awaiting PET for primary localisation / other sites of peritoneal disease.

PET Homogenous low-grade activity of parasplenic mass – otherwise unremarkable study.

Final Diagnosis # 1 • Accessory Liver Lobe // “Ectopic Liver“ • Confirmed on further re-analysis of Histology • Accessory lobe of the liver (ALL) is congenital ectopic hepatic tissue mostly due to embryonic heteoplasia (Aut. Recessive) • In rare instances an ALL may occur after trauma or surgery. • Classified by those connected to liver and a completely separate lobe • If connected may be pedunculated or sessile. If remote can even lie within thorax or pelvis

Final Diagnosis # 1 • Torsion, traumatic rupture or infarction the principle presenting complications. • Surgical resection may be considered in these contexts – or if other congenital anomalies in children. • Diagnosis confirmed histologically – usually post-operatively. In this case on re-review.

Case #1 - Retrospect Subdiaphragmatic stalk of enhancing tissue extending from the left lobe of the liver into the left upper quadrant – peduncle of ALL

History #2 • RIF Pain and tenderness and fever 10 days post C-Section. • ? Appendicitis ? Collection • CT AP + IV
 • Ill-defined appendix – appendicitis")
CT AP + IV • RIF/lower abdominal inflammation (post-op) • Ill-defined appendix – appendicitis not excluded

Case #2 • Laparoscopic appendicectomy • Incidental note made of small nodule related to distal small bowel • MRI Small Bowel requested to assess.

MRI Small Bowel Solitary distal small bowel enhancing polyp – appears more intraluminal. ? Carcinoid ? GIST

Bloods • • • Chromogranins VIP Gastrin Glucagon Somatostatin All Normal • Pancreatic Polypeptide Insufficient sample for analysis

CTE for further assessment Solitary distal Ileal enhancing intraluminal nodule. Otherwise unremarkable

Re-discussed at MDT • Planned for small bowel resection ? NET ? GIST • Smal bowel resection - Histology?

Final Diagnosis • Ectopic Pancreatic tissue.

Ectopic Pancreas • More common within proximal GI tract – Stomach, duodenum and jejunum (70%) • But can occur anywhere • Often incidental finding at laparoscopy for other reasons. • Resection recommended: – Can result in pain or bleeding related to pancreatitis. – Neoplastic transformation – Lead point for intussusception

Ectopic Pancreas • Diagnosis confirmed histologically – usually post-resection as submucosal location can limit yield from enteroscopic biopsy

Learning Point • Keep an open mind for atypical benign pathology – particularly in the incidental finding. • Wide variety of locations of ectopic parenchyma.

References • Accessory lobes of the liver: A report of 3 cases and review of the literature. Intractable & Rare Diseases Research. 2012; 1(2): 86 -91. Chenglin Wang et al • Ectopic liver: Different manifestations, one solution. World J Gastroenterol 2013 October 14; 19(38): 6485 -6489. Pavel Zonca, Lubomir Martinek, Peter Ihnat, Jan Fleege • Heterotopic pancreas in the gastrointestinal tract. World J Gastroenterol. 2009 Aug 7; 15(29): 3701– 3703. Zhou Yuan et al
- Slides: 26