Interesting case Diagnosis rupture globe Operation repair globe

Interesting case Diagnosis : rupture globe Operation : repair globe left eye R 2 Jutamas Srisung Advisor : Lt. Col. Natthaphong

History taking ? ? R 1

Past history • Underlying disease : DM, HT, DLP, ESRD • ESRD on HD 3ครง /week (จนทร , พธ , ศกร ) via Lt. forearm AVBG, last HD on Friday (on complication during HD, clinical euvolumia) • No drug allergy • No history of surgery • No history of smoking or drinking alcohol

Past history • No history of snoring • Time of injury : 6. 00 am, NPO time : 7. 00 am • Functional class II
 1 x 1 po pc")
Past history • ‐ ‐ ‐ Current medication ASA(81) 1 x 1 po pc Simvastation (40) 1 x 1 po hs Mixtard (70/30) 40‐ 0‐ 26 u sc ac Pioglitazone(15) 1 x 1 po pc Furosemide (40) 2 x 1 po pc Lercardipine (20) ½ x 1 po pc

Physical examination • A thai woman , good concoiusness • BW : 75 kg , Height 153 cm, BMI : 32. 04 kg/m 2 • HEENT : not pale, no jaundice • Left eye : conjunctival larceration , subconjunctival hemorrhage c hyphema, not seen pupil • Right eye : normal contour, pupil 2 mm. RTL • VA : Lt eye : HM , Rt eye : 20/80

Physical examination • Airway examination : Limit neck of motion : No Thyromental distance > 6 cm Mouth opening > 3 cm Upper lip bite test : grade 1 Prominent incisor : No Mallampati grade : grade 2

Physical examination • Pulmonary : no dyspnea , no tachypnea , equal breath sound both lungs • CVS : Pulse full & regular , no heaving, no thrill, normal S 1&S 2, no murmurs • Abdomen : soft, not tender, liver & spleen can not palpable • Extremities : no deformity, no pitting edema • Neuro : E 4 M 6 V 5, no facial palsy, Rt Pupil 2 mm RTL Lt cant evaluation, motor grade V/V all, no weakness

Investigation R 1

Investigation • CBC: Hb 10. 0 gm/dl, Hct 32 %, Platelet 258, 000/mm 3 • Electrolytes: Na 139, K 5. 0, Cl 106, CO 2 23 • BUN: 72. 1 mg/d. L Cr: 6. 01 mg/d. L • Calcaim 8. 9 , Phosphate 3. 3, Magnesium 1. 9 • Anti HIV : negative • DTX 172 mg%

Ekg • NSR, regular rate, HR 75 bpm , no chamber hypertrophy , no LVH , no ischemic pattern

Chest x-ray • Normal , no infiltration, mild cardiomegaly No fracture rib
 • Normal structural brain , no ICH , no skull fracture")
CT-Brain (non contrast) • Normal structural brain , no ICH , no skull fracture

Problem list R 1

Problem list • Rupture globe at Left eye • Obesity • Underlying disease : hypertension , DLP, DM type II, ESRD

Preoperative evaluation • Rupture globe lt eye • obesity • U/D : HT, DM type II, ESRD

Preoperative evaluation R 2

Preoperative evaluation • ‐ ‐ ‐ Rupture globe injury : No asscociated trauma VA at lt eye : HM Prevent increase intra ocular pressure

Morgan&Milhail’s Clinical anesthesiology 5 Th

Rupture globe injury • Open globe injury is not require immediately and some time can spent to adequate preparing patient. • The surgery should not be performed within 12 hr to minimize infection and other complication

Rupture globe injury • In case unreliable GI absorbtion aspiration prophylaxis • Metoclopramide 0. 15 mg iv facilitate gastric emptying and increase tone of LES reduce gastric • Ranitidine 50 mg iv acidity • Nonparticulate antacid

Obesity

Low risk of OSA

Obesity Airway ‐ Potentially difficult airway ‐ Excessive tissue: mouth & pharynx ‐ Short & thick neck ‐ Limited movement of atlantoaxial joint& C‐ spine: lower‐C and upper‐ T fat pads ‐ Large breast ‐ Thick submental fat pad

Obesity • • • Airway Cardiovascular Respiratory Metabolic Hematologic

Hypertension • End organ damage caused by long standing hypertension : ‐ CVS : LVH, MI, CHF ‐ Renal involvement : nephropathy ‐ Cerebral involvement : TIA, stroke

Hypertension ‐ Identified current therapy ‐ Evaluated EKG, CXR, serum creatinine ‐ Identified normal baseline BP

DM type II ‐ Blood glucose preoperative ‐ Targets range of glycemic control : 100‐ 180 mg/dl ‐ End organ damage : Macrovascular : stroke , MI Microvascular : nephropathy , neuropathy , cardiomegaly

DM type II ‐ Aware “stiff joint syndrome” ‐ Pre operative hyperglycemia is associated with worsened neurologic and cardiac ischemia and poor wound healing ‐ Hypoglycemia serious risk

ESRD ‐ Clinical euvolumia , regular HD ‐ Lab : Hct , electrolyte normal ‐ Aware platelet dysfunction

ASA classification • ASA class III E

Preoperative preparation R 2

Preparation NPO Inform Consent Warm IV fluid Force air warmer No G/M blood component Prepare drug for blunt airway reflex (such as lidocaine , esmolol, labetalol • Difficult airway management • • •

Preoperative preparation • Ramp position • Proper size NIBP cuff • Dextro‐strip to monitor intraoperative blood glucose • Prepare insulin , glucose for collect blood glucose intraoperative

Choice of anesthesia RA VS GA

Regional anesthesia Advantage ‐ Decrease risk of aspiration ‐ Postoperative analgesia ‐ Nausea and vomiting are infrequent ‐ Return ambulation faster Disadvantage ‐ Increase IOP (volume of local anesthesia) ‐ Extrude intraocular contents ‐ Time limit operation ‐ Can mobile

General anesthesia • Preferred technique for open‐globe injury ‐ Immobile patient ‐ No time limitation
 avoid")
Choice of anesthesia • GA with oral RAE with controlled ventilation Oral RAE(Ring-Adair-Elwyn) avoid kinking and obstruction Morgan&Milhail’s Clinical anesthesiology 5 Th

Intra operative management

Anesthetic consideration R 3

Anesthetic consideration Smooth induction and intubation Control intraocular pressure Concern severe oculocardiac reflex Smooth emergence and extubation

Intraoperative • Monitoring : standard monitoring : EKG , NIBP , O 2 sat , Et. CO 2 • Position : supine • intraoperative lab monitoring : blood glucose

time in OR 23. 00 Monitor • NIBP, EKG, O 2 sat • BP at OR 180/70 mm. Hg • PR 70 / min

At 23. 05 • Ramped position • Preoxygenation • Esmolol 30 mg iv x 2 dose Induction & intubation: • Fentanyl 50 mcg IV • Propofol 100 mg IV • Cisatracurium 10 mg iv • ETT oral RAE no 7. 5 depth 19 cm by video laryngoscope (C‐ mac)

Smooth induction and intubation To prevent BP and heart rate rise at the time of intubation • Fentanyl 7‐ 8 mcg/kg IV with induction • Lidocaine 1. 5 mg/kg IV : 2 minutes before intubation • Nicardipine 0. 015‐ 0. 03 mg/kg IV : 2 minutes before intubation
, Short")
Smooth induction and intubation • Esmolol 2 mg/kg IV (Selective Beta 1 blocker), Short duration of action , half life 9 min • Labetalol 0. 15‐ 0. 45 mg/kg IV (Non‐selective Beta blocker), also action in alpha rp , long acting , half life 5 hr
 • Total body weight")
Intraoperative • Most of the drugs: – Lean body weight(LBW) • Total body weight (TBW) in: – Propofol (maintenance infusion) – Succinylcholine – Dexmedetomidine – Neostigmine

Intraoperative Ramped position : for intubation

Anesthetic consideration Smooth induction and intubation Control intraocular pressure Concern severe oculocardiac reflex Smooth emergence and extubation
 • Normal pressure is 10‐ 20 mm. Hg • Cough, strain")
Intraocular pressure (IOP) • Normal pressure is 10‐ 20 mm. Hg • Cough, strain or vomiting increase IOP 30‐ 40 mm. Hg • Forceful eyelid squeeze increase IOP more than 50 mm. Hg
 Morgan&Milhail’s Clinical anesthesiology 5 Th")
Effect of cardiac and respiratory variables on intraocular pressure(IOP) Morgan&Milhail’s Clinical anesthesiology 5 Th
 Morgan&Milhail’s Clinical anesthesiology 5 Th")
Effect of anesthetic drug on intraocular pressure(IOP) Morgan&Milhail’s Clinical anesthesiology 5 Th
 • The degree of IOP reduction is")
Effect of anesthetic drug on intraocular pressure(IOP) • The degree of IOP reduction is proportional of depth of anesthesia

Succinylcholine • • • Transient increase IOP Increase IOP 6 ‐ 12 mm. Hg Duration 5 ‐ 10 minutes Extraocular muscle spasm Increase serum potassium by 0. 5 m. Eq/L

Effect of Hypothermia on IOP • Increase viscosity of aqueous humor elevate IOP • Decrease formation of aqueous humor reduce IOP • Vasoconstriction : reduce IOP Conclusion : reduce IOP

Intraoperative : maintainance

• Maintainance: air: O 2: 1: 1 desfurane 6 % • Muscle relaxant: cisatracurium 10 mg • Analgesia : Fentanyl 100 mcg with titration doses • Antiemitic : ‐ ondrasetron 8 mg IV ‐ Dimen 50 mg iv ‐ Metoclopramide 10 mg iv • DTX : 98‐ 118 mg% • Operation time : 3 hr 10 min

Intra operative management • Control BP : Useful guideline is decrease 25% of MAP to lower limit of autoregulation • Intra‐operative blood glucose monitoring :

Anesthetic consideration Smooth induction and intubation Control intraocular pressure Concern severe oculocardiac reflex Smooth emergence and extubation

Oculocardiac reflex • Manifested by bradycardia, bigeminy, ectopy, nodal rhythms, A‐V block and cardiac arrest • Caused by traction on the extraocular muscle (espacially medial rectus)
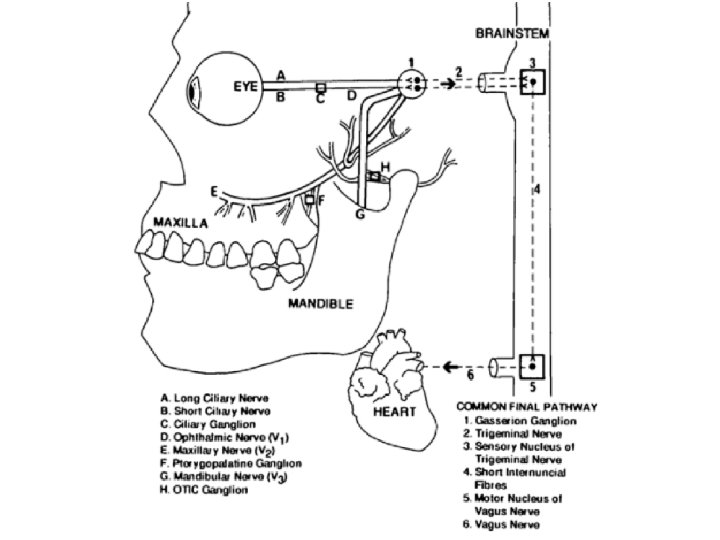

Oculocardiac reflex • Afferent pathway : Orbital content ‐> Ciliary ganglion ‐> Ophthalmic division of Trigeminal nerve(CN V 1) ‐> Gasserion ganglion ‐> Sensory nucleus of trigeminal nerve • Efferent pathway : Motor nucleus of vagus nerve(CN X) ‐> Heart(sinoatrial node)

Management of oculocardiac reflex • Notify surgeon and cessation surgical stimuli (heart rate and rhythm return in 20 seconds) • Confirm of adequate ventilation, oxygenation and depth of anesthesia • If the initial cardiac dysrhythmia is especially serious or if the reflex tenaciously recurs – Atropine 0. 02 mg/kg IV – Glycopyrrolate 0. 01 mg/kg IV

Management of oculocardiac reflex • infiltration of rectus muscle with local anesthesia decrease incidence of OCR • No role of premedication prophylaxis • Reflex fatigue with repeated traction on the extraocular muscle

Intraoperative : emergence

Anesthetic consideration Smooth induction and intubation Control intraocular pressure Concern severe oculocardiac reflex Smooth emergence and extubation

• Emergence : awake extubation • Reverse : Prostigmine 2. 5 mg , Atropine 1. 2 mg IV • Blunt airway reflex : esmolol 40 mg iv • IV fluid : 5% DN/2 700 ml • EBL : minimal

Emergence and extubation • Smooth emergence and extubation • Deep extubation if indication and no contraindication • Blunt cardiovascular response if indication

Deep extubation With 'deep' extubation, the ET tube is removed before wake-up and before the return of upper airway reflexes • Finish operation • reverse muscle relaxant but continue volatile • Spontaneous ventilation : Tidal volume and respiratory rate • Suction secretion

Deep extubation • Off endotracheal tube • Maintain airway under mask may use oral or nasal airway • Discontinue volatile and 100 % oxygen

Contraindication of deep extubation • • • Difficult ventilation or intubation Obesity Obstructive sleep apnea Risk of aspiration pneumonitis Risk of airway swelling

Post operative

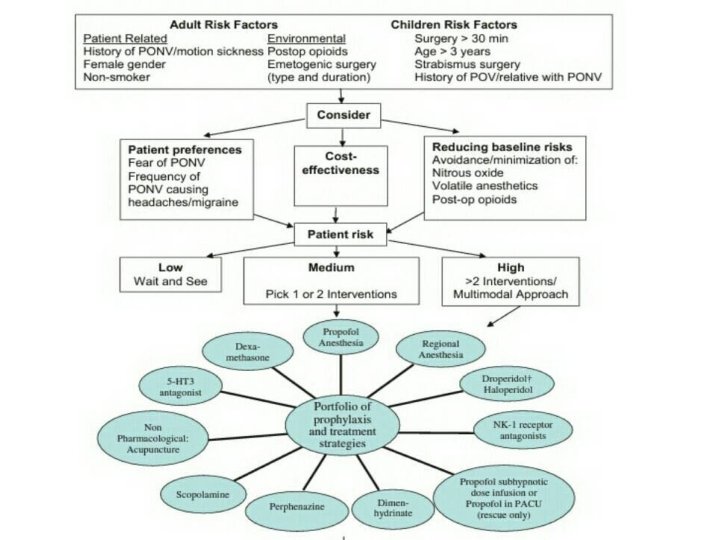
Post operative • Post operative nausea vomiting 0‐ 1 = low risk 2 = medium risk 3 and more = high risk Consensus guideline for management post operative nausea vomiting ; anesthesia&analthesia 2014

Post operative • S: ตนรตวปกต ไมมคลนไสอาเจยน ไมมไข ปวดแผลเลกนอย หายใจไดดไมเหนอย • O: V/S : BP 150/90 , PR 60/min RR 18/min BT 36. 6 C HEENT : no lids swelling , no stitch off wound no signs of endophthalmitis, VA lt eye: HM Cardiovascular : normal s 1 s 2, no murmur, regular rate Respiratory : room air o 2 sat 100 %, lungs clear both ext : no pitting edema urine output : none HD : regular ( จนทร , พธ , ศกร )

Post operative • A&P : clinical stable ‐ Volume status : Euvolumia ‐ Adequate pain control : paracetamol (500) 1 tab oral prm q 4 hr ‐ Blood glucose 100‐ 180 mg% ‐ post operative nausea vomiting : odensetron 8 mg iv , Metoclopramine 10 mg iv , dimen 50 mg iv

Reference • Clinical anesthesia 7 Th edition ; anesthesia for ophthalmologic surgery • Morgan&Milhail’s Clinical anesthesiology 5 Th edition • Yao&Artusio’s Anesthesiology 7 th edition • Consensus guideline for management post operative nausea vomiting ; anesthesia&analthesia 2014 • Perioperative management of diabetic patient ; Medscape

Thank you for your attention**
- Slides: 79