Intellectual Disabilities Developmental Disorders ASSESSMENT DIAGNOSIS DSM5 definitions

Intellectual Disabilities & Developmental Disorders
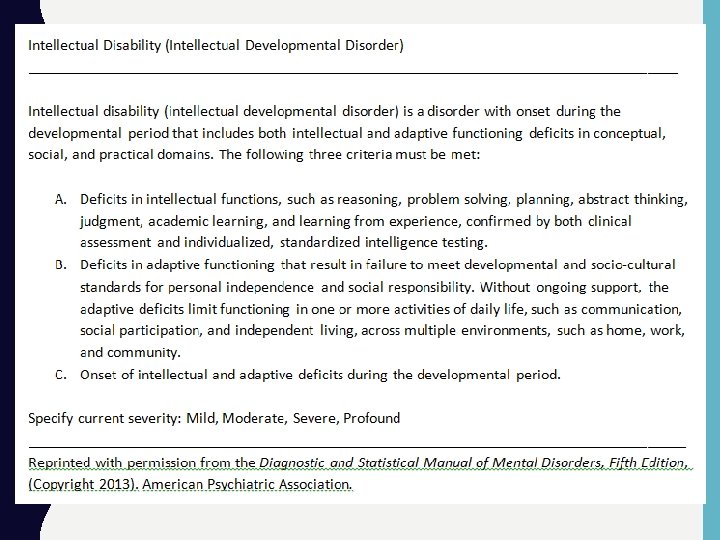

ASSESSMENT & DIAGNOSIS • DSM-5 definitions of ID includes the assessment of 2 constructs: – Intelligence scores • 2 standard deviations below the mean – Adaptive functioning: • 2 standard deviations below the mean
 • Wechsler")
INTELLIGENCE TESTS • Wechsler Tests: • Preschool & Primary Intelligence Test (WPPSI) • Wechsler Intelligence Scale for Children (WISC) (see next slide) • Wechsler Adult Intelligence Test (WAIT) • Stanford-Binet • A well-established, but less commonly used alterative. • Only 1 version, starting points and administration of specific subtest varies by age.

WISC-V: COMPOSITE SCORES • The following composite scores are calculated, each is based on 2 specific subtests: – Verbal comprehension – Visual spatial – Fluid reasoning – Working memory – Processing speed – Full scale (7 subtests: 1 -2 from each of the categories above) – See link for more a more detailed example http: //images. pearsonclinical. com/images/assets/wisc-v/WISC-V-Score. Report. pdf

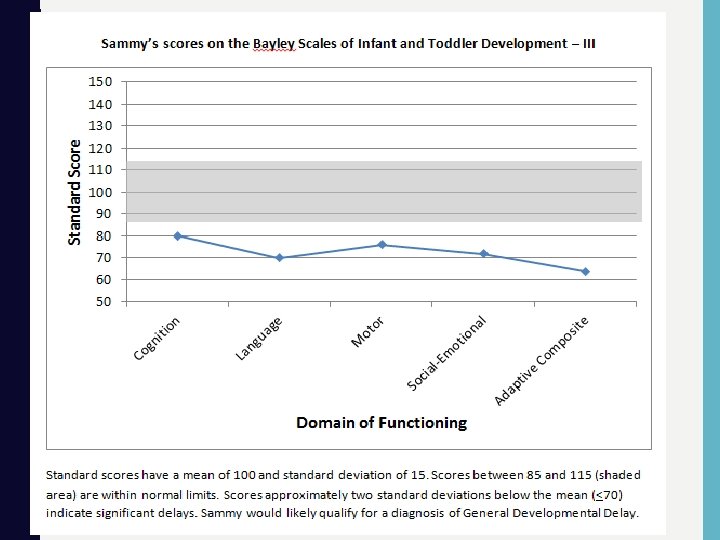
ASSESSMENT OF INFANT DEVELOPMENT • Bayley Scale for Infant Development – Motor (gross & fine) – Cognitive – Language (expressive & receptive) http: //www. pearsonclinical. com/childhood/products/100000123/bayleyscales-of-infant-and-toddler-development-third-edition-bayley-iii. html

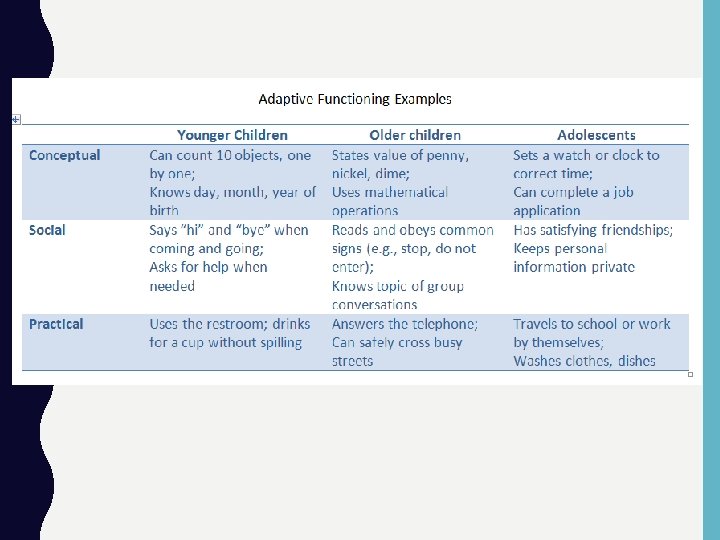
ADAPTIVE FUNCTIONING • There a number of standardized measures designed to adaptive functioning. Examples including the following: – Vineland Adaptive Behavior Scales (see link) • Domains include communication, daily living skills, socialization, motor skills, & maladaptive behaviors. http: //www. pearsonclinical. com/psychology/products/100001622/vine land-adaptive-behavior-scales-third-edition--vineland 3. html? cmpid=300224 -PPCVineland 3&gclid=CNGri. L 3 Vk 80 CFdg. Ug. Qod. Qj 8 Kww – Adaptive Behavior Assessment System (ABAS) (see link) http: //www. pearsonclinical. com/psychology/products/100000449/ada ptive-behavior-assessment-system-second-edition-abas-secondedition. html#tab-details

PREVALENCE • Total: 2% (this is based on ability relative to others– 2 standard deviation units below the average) • Percent by category (see next – Mild- 85% – Moderate- 10% – Severe & Profound (5%) • Severe- 3 -5% • Profound- 1 -2%

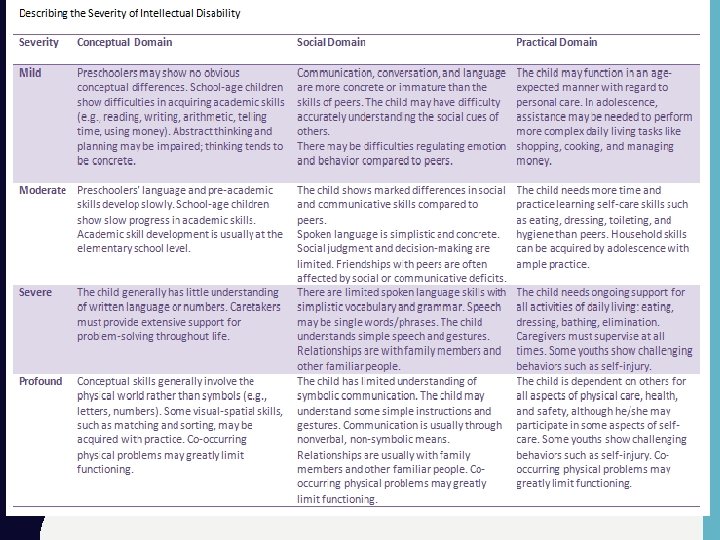
CHARACTERISTICS AND EXPERIENCES OF CHILDREN WITH INTELLECTUAL DISABILITY • Cognitive abilities of children with mild ID may be similar to other children during preschool years, but they grow at a slower rate and peak at approximately the abilities of an average 6 th grade child • Children with moderate ID have significant delays in language development (2 nd academic level) • Children with severe ID don’t develop language until schoolage years • Those with profound ID do not develop language, but may recognize and respond to a few words

FORMALLY USED TERMS • DSM-IV – Mental retardation • Until the 1970 s: – Moron (51 -70 IQ) – Imbecile (50 -26 IQ) – Idiot (25 and below IQ)

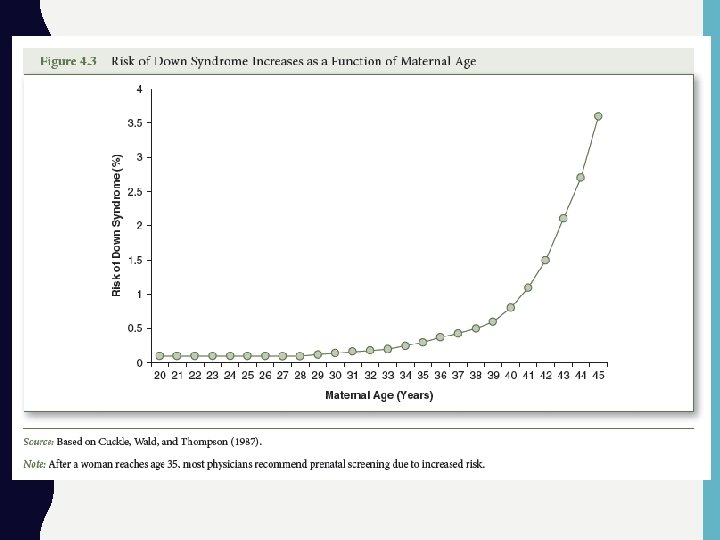
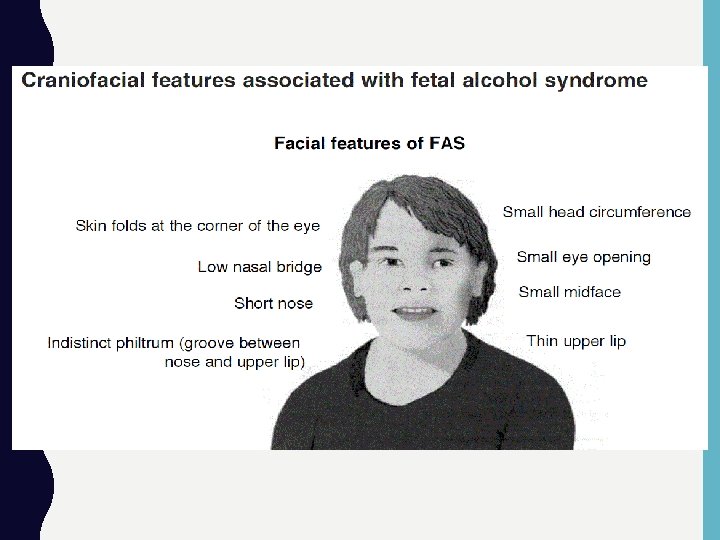
ETIOLOGY • Etiology can be classified as coming from one of two sources: – Organic- the ID is due to a biological problem or deficit, can be genetic disorders (e. g. , Down Syndrome/Trisomy 21) or environmental (fetal alcohol syndrome). In these cases there seems to be a clear etiology (“cause”). – Cultural-Familial- some cases do not seem to be a function of an organic problem or deficit. Rather, based on natural variation in ability-- some individuals are naturally going to fall in the lower end of the distribution. – See page 102 of text.
 • Among the most commonly")
ORGANIC: GENETIC/CHROMOSOMAL • Examples: – Down syndrome (trisomy 21) • Among the most commonly known & genetic disorders. In most cases, the individual has 3 rather than 2 copies of the 21 st chromosome. • Distinct phenotype, 1 per 1000 births. • Impairment usually mild (ID in mild range) • Usually described as friendly and socialable. – Fragile X syndrome • Mutation on the X chromosome (female sex chromosome) • Moderate to severe impairment. • Autistic-like behavior common, distinct phenotype. • 1 per 1500 live births. • Gender differences: more common in females, symptom presentation more severe in males.
: – Prader-Willi Syndrome • Loss of function of part")
ORGANIC: GENETIC/CHROMOSOMAL • Examples (continued): – Prader-Willi Syndrome • Loss of function of part of chromosome 15. • Distinct phenotype including narrow forehead & almond shaped eyes • Distinct behaviors including overeating & inability to regulate appetite to the point of self-harm. • Mild intellectual impairment – Phenylketonuria (PKU) • Body does not break down phenylalanine (an amino acid). It builds up on the body & the protein builds up in the body. • Screening at birth (which is standard practice now) can prevent serious problems.

ORGANIC: PREDOMINANTLY ENVIRONMENTAL • This category can include a number of issues including: – Teratogen exposure en utero, including… • Maternal substance abuse (e. g. , fetal alcohol syndrome) • Medications • Viruses (e. g. , microencephalopathy from zika virus) – Illnesses & injuries in childhood, including… • Falls resulting in head injuries • Encephalitis & meningitis • Lead exposure – Complications during birth, including… • Oxygen depravation during the birth process (e. g. , umbilical cord around the neck).

INTERVENTION: EDUCATIONAL • Early intervention: mandated by federal law for disabled children ages 3 -5 • School: All children with disabilities must receive an individualized education plan (IEP) • Transition to after-school life for children over 14 years of age is an important IEP component

OTHERAPEUTIC INTERVENTIONS • Behavioral interventions – Both in the school and at home. • Parent education – Working with parents to help them understand be able to manage certain behaviors.
- Slides: 21