Integration of the Controlled Substances Monitoring Database CSMD
 into CRNA Practice Brent Earwood, CRNA,")
Integration of the Controlled Substances Monitoring Database (CSMD) into CRNA Practice Brent Earwood, CRNA, DNP(s) Union University College of Nursing Chairman CSMD Committee TN Dept. of Health

The Problem Prescription drug abuse has reached epidemic proportions in the U. S.

In 2016, Tennessee had the 4 th highest per capita prescription rate for opioids in the U. S.

Tennessee currently ranks 3 rd nationwide in RX drug abuse

The dramatic increase in opioid abuse and overdose deaths has a direct correlation with the number of opioid prescriptions written.

Unintentional overdose deaths increased more than 250% from 2001 to 2015, exceeding deaths due to falls, guns, or MVAs in 2015

The number of babies born dependent to drugs who suffered from Neonatal Abstinence Syndrome (NAS) grew tenfold from 2001 -2011.

Americans make up 5% of the world’s population, but consume 75% of the world’s prescription drugs

In many cases, prescription drug abuse leads to the abuse of heroin due to its easy availability and low cost. Heroin use rose 75% between 2007 & 2011

But even with heroin use increasing, in 2013 seven out of ten opioid overdoses seen in emergency rooms across the country involved prescribed opioids, not illegal opioids like heroin

Over half of the Americans who died from an opioid overdose in 2015 died from prescription meds

“Ok…that’s really sad, but how does that affect me as a CRNA? ”

Because…you’re putting these people under every day and may be unaware of their prescription drug abuse

What is the Controlled Substance Monitoring Database? CSMD is Tennessee’s prescription drug monitoring program (PDMP)

A PDMP is a searchable database of controlled substance prescriptions

Purpose of CSMD • The purpose of the CSMD is to collect data on controlled substance prescribing, and by use of algorithms, identify patterns of drug abuse, diversion, misuse, morbidity, & mortality

• By flagging suspect behavior patterns, prescribers and pharmacists can be alerted to potential doctor shoppers and patterns of misuse

• Prescribers in Tennessee are required by law to access the CSMD prior to writing for a controlled substance • Pharmacists are required to check the CSMD prior to filling opioid or benzodiazepine scripts on new patients and then again annually if treatment continues

• PDMPs exist in every state but Missouri

Use of CSMD allows timely review of patient specific controlled drug records

TN Prescription Safety Act of 2016 • A major step forward in addressing prescription drug abuse in Tennessee, signed into law by Governor Bill Haslam on April 27, 2016

Specifically amended TCA 53 -10 -302 to include CRNAs as Healthcare Practitioners authorized to access the CSMD database

New Student Attention Monitor

JCAHO published a sentinel event alert in 2012 reminding hospital personnel to specifically address a patient’s previous analgesic use and abuse, duration of use, and any side effects that may indicate opioid tolerance or intolerance

Why do CRNAs Need the CSMD? • Allows accurate review of controlled substance RX history during preanesthetic review. • Can provide a starting point for honest conversation between patient and CRNA regarding actual drug use.

After discussing the CSMD report with your patient, this information can be used to tailor your anesthetic to the patient’s anticipated narcotic needs.

Why Should We Use CSMD? Because patients don’t always tell the truth

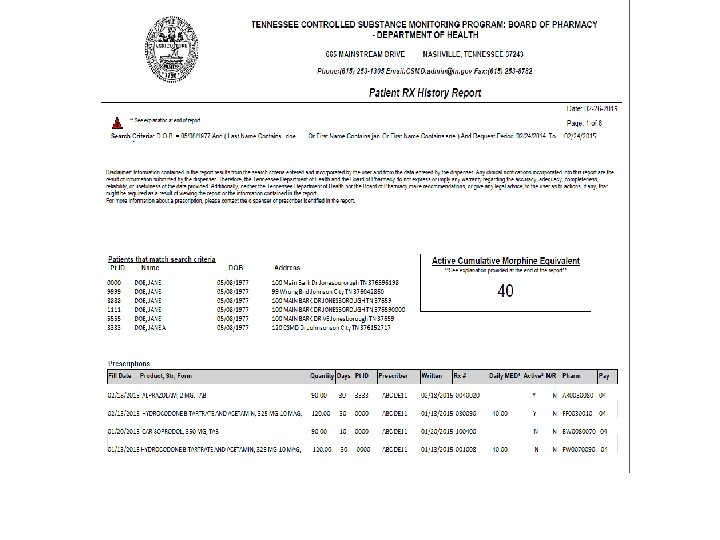
Actual Patient Scenario • Here’s an example of the CSMD in anesthesia practice. • Patient presented for a Baclofen pain pump exchange • He was being treated by a chronic pain practitioner and was under a pain contract. • Being unsure of the accuracy of his drug history, the CSMD was accessed to gain insight into the actual drug usage of the patient.

Drug List on Interview • • MS Contin Soma Xanax Valium Morphine Actiq Baclofen Pump

Drug List on CSMD with Sig from Pharmacy • • MS Contin 400 mg q 8 hrs Soma 350 mg qid for muscle spasms MS Contin 200 mg q 8 hrs Xanax 2 mg bid Morphine IR 30 -60 mg q 4 -6 hrs prn Actiq 800 ugs q 3 -6 hrs prn Valium 10 mg q 8 hrs for muscle spasms

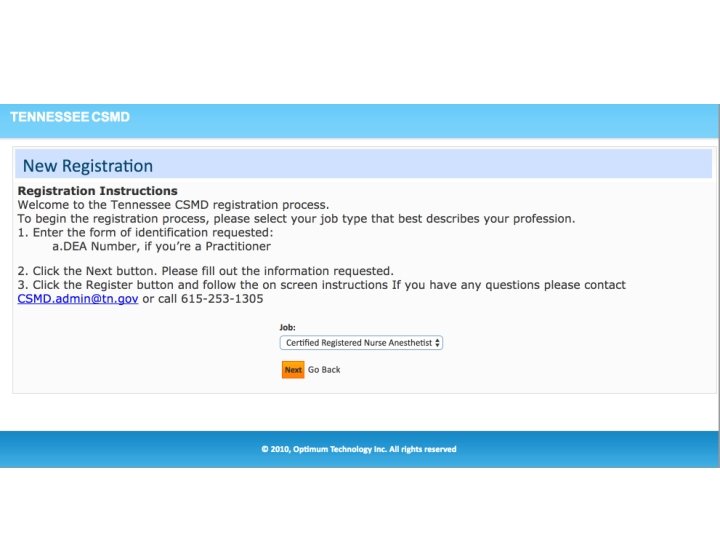
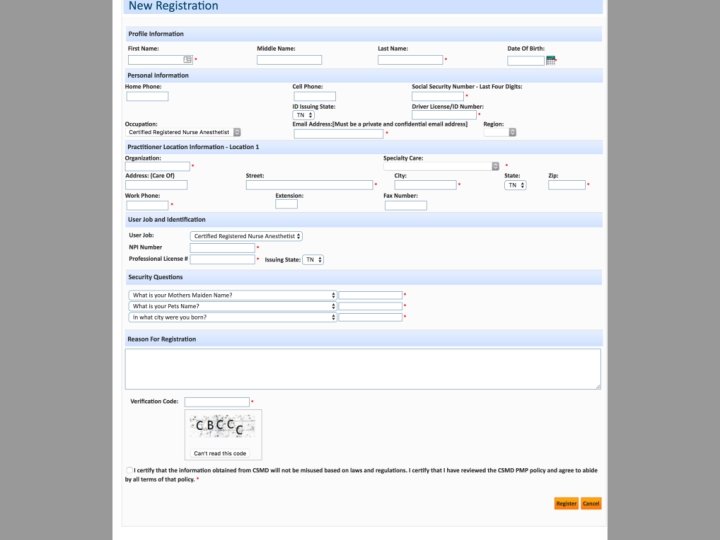
Getting Started • Go to www. tncsmd. com and register

What You Will Need • Have these numbers available when you prepare to register – National Provider Identifier number (NPI) – APRN certificate number – TN driver’s license number – Last 4 digits of your SSN – Practice location information

Using the Database • Logins are dated and stored • TN state laws, rules, & regs. govern access • You may allow other licensed individuals to login under your supervision as your delegate using their unique login credentials • May print out CSMD reports • No requirement for CRNA to use CSMD. Use is totally voluntary
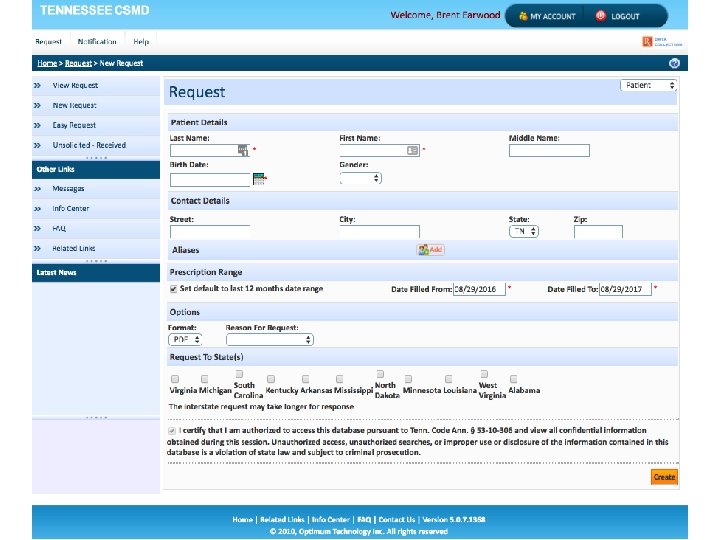

Training User
 of hydrocodone, oxycodone and codeine? Formula for")
What is the morphine milligram equivalents (MME) of hydrocodone, oxycodone and codeine? Formula for MME per day: Strength(in mg) X Morphine Equivalent X Quantity Number of days Conversions to MME Opioid name Oxycodone Hydrocodone Codeine Equivalent Milligrams milligrams (mg) of opioid morphine 1 1. 5 1 1 1 0. 15
 on CSMD Reports Y = 4 Practitioners in")
Clinical Risk Indicators (high risk patients) on CSMD Reports Y = 4 Practitioners in last 90 days Y = 4 Pharmacies in last 90 days Y ≥ 90 but < 120 Active Cumulative Morphine Equivalents per day R ≥ 5 Practitioners in last 90 days R ≥ 5 Pharmacies in last 90 days R ≥ 120 Active Cumulative Morphine Equivalents per day

Questions?
- Slides: 47