Integrating Suicide Prevention within PBIS Lucille Eber Midwest
 Tim Knoster (Mc. Dowell")
Integrating Suicide Prevention within PBIS Lucille Eber (Midwest PBIS Network) Tim Knoster (Mc. Dowell Institute: Bloomsburg University) Danielle Empson (Mc. Dowell Institute: Bloomsburg University) Keywords: Mental Health, Systems Alignment, and Evaluation

Maximizing Your Session Participation Consider 4 questions… 1. Where are we in our implementation? 2. What do I hope to learn? 3. What did I learn? 4. What will I do with what I learned?

Where are you in the implementation process? Adapted from Fixsen & Blase, 2005 Exploration & Adoption • We think we know what we need so we are planning to move forward (evidencebased) Installation • Let’s make sure we’re ready to implement (capacity infrastructure) Initial Implementation • Let’s give it a try & evaluate (demonstration) Full Implementation • That worked, let’s do it for real and implement all tiers across all schools (investment) • Let’s make it our way of doing business & sustain implementation (institutionalized use)

i p T e a m L e A M a c e d tm e ib ro e sn r h i. P N p lo a t T n e e n a i. T m n a g k A i c W n to g ir o k W n so h r P e k Leadership Team Action Planning Worksheets : Steps S e l f A s. S se s e ss si o m A n e c n t A ti : so s

IDE W L O R SCHO BEHAVIO TIVE I S O P ORT P P U S ORK: W E FRAM ~5% ~15% Tertiary Prevention: Specialized Individualized Systems for Students with High-Risk Behavior Secondary Prevention: Specialized Group Systems for Students with At-Risk Behavior Primary Prevention: School-/Classroom. Wide Systems for All Students, Staff, & Settings ~80% of Students Student s Staff Parents /Familie s

Experimental Research on SWPBIS Experimentally Related to: 1. 2. 3. 4. 5. 6. 7. 8. 9. Reduction in problem behavior Increased academic performance Increased attendance Improved perception of safety Reduction in bullying behaviors Improved organizational efficiency Reduction in staff turnover Increased perception of teacher efficacy Improved Social Emotional competence

NPR The Silent Epidemic: The Mental Health Crisis in our Schools Published on-line September 7, 2016

NPR Story Conclusion: In Schools, Mental Health should be EVERYONE’s Job

Advancing Education Effectiveness: Interconnecting School Mental Health and School-Wide Positive Behavior Support Editors: Susan Barrett, Lucille Eber and Mark Weist pbis. orgcsmh. umaryland IDEA Partnership NASDSE

PBIS Provides a Solid Foundation…. but More is Needed… • Many schools implementing PBIS struggle to implement effective interventions at Tiers 2 and 3 • Youth with “internalizing” issues may go undetected • PBIS systems (although showing success in social climate and discipline) often do not address broader community data and mental health prevention.

ISF Defined • Structure and process for education and mental health systems to interact in most effective and efficient way. • Guided by key stakeholders in education and mental health/community systems • Who have the authority to reallocate resources, change role and function of staff, and change policy.

ISF Enhances MTSS Core Features • Effective teams that include community mental health providers • Data-based decision making that include school data beyond ODRs and community data • Formal processes for the selection & implementation of evidence-based practices (EBP) across tiers with team decision making • Early access through use of comprehensive screening, which includes internalizing and externalizing needs • Rigorous progress-monitoring for both fidelity & effectiveness of all interventions regardless of who delivers • Ongoing coaching at both the systems & practices level for both school and community employed professionals

is s s e c c A 2. NOT enough 1. Single System of Delivery Key Messages 4. MTSS essential to install SMH 3. Mental Health is for ALL

What Does it Mean to Integrate? Change in routines and procedures? (e. g. who needs to be available to participate in team meetings? ) Change in how interventions are selected and monitored? (e. g. team review of data/research vs individual clinician choice? ) Change in language we use? (e. g. identifying specific interventions vs generic terms such as “counseling” or “supports”? ) Changes in Roles/functions of staff? (e. g. clinicians coordinating/overseeing some interventions that nonclinicians deliver? )

INCORPORATE Coping Strategies for Managing Stress Teaching Matrix Expectations Respectful All Settings Achieving & Organized Be kind. Hands/feet to self. Help/share with others. Walk. Have a plan. Share Use equipment. normal Include others. voice volume. Walk to right. c i f ci e p S r o s s r o le i u v R eha . R 3 esponsible. B Recycle. Clean up after self. Playgroun ds s n io t a t c Be on task. Give your best effort. Be prepared. e p Ex 1. Halls Pick up litter. Maintai n physical space. Use equipment properly. Put litter in garbage can. Lunch Invite those sitting alone to join in Have a lunch plan and choose quiet or social lunch area Library / Assembl Comp y uter CLab O 2 NT. N EX AT T UR (L Study, oc ALWatch for Sit in one read, spot. at your stop. compute. io ns ) Whisper. Return books. Listen/wat ch. Use appropriat e applause. Use a quiet voice. Stay in your seat. Push in chairs. Treat books carefully. Pick up. Treat chairs carefully. Wipe your feet. Invite friends to join me Use my breathing technique Listen to my signals Bus
 Sample (sample academic skills group)")
“Social & Academic Instructional Groups” Daily Progress Report (DPR) Sample (sample academic skills group) NAME: ___________ DATE: _________ EXPECTATIONS 1 st block Be Safe 2 1 0 Walk to class Keep hands to self Be Respectful Mark will hold up a yellow card to indicate needing a break Be Responsible Mark will fill out assignment notebook Total Points Teacher Initials 2 nd block 3 rd block 4 th block “Individualized Student Card for Mark” (FBA/BIP) 5 th block 6 th block 7 th block 2 1 2 1 0 0 0 2 1 2 1 0 0 Possible 0 behaviors 0 taught 0 in previous 0 SAIG 0 grou Replacement behavior 2 1 2 1 0 0 0 0
 Sample NAME:")
Trauma. Informed Tier 2 Group EXPECTATIONS Be Safe Daily Progress Report (DPR) Sample NAME: ___________ DATE: _________ Teachers please indicate YES (2), SO-SO (1), or NO (0) regarding the student’s achievement in relation to the following sets of expectations/behaviors. 1 st block 2 nd block 3 rd block 4 th block 2 1 0 2 1 0 2 1 0 2 1 0 Self-Check Use calming strategy Be Respectful Use your words Use safe hands Be Responsible Ask for help Connect with safe person Total Points Teacher Initials Adapted from Grant Middle School STAR CLUB
")
Monitor – Fidelity (focus on features of the intervention)

Situating Suicide Prevention within PBIS Core Components • Evidence based interventions and strategies. • Data informed decision making. • System development to enable accurate and durable implementation Strategies to support students known to be at higher risk of suicide Individualized student interventions and supports Crisis response and community partnerships Ongoing program changes based on progress monitoring associated with students response to intervention School-based Suicide Prevention • Policies and procedures for prevention, intervention and postvention • Education for students, staff, and families • Screening and assessment Strategies to identify and support students that may be at risk for suicide Targeted training for specialized staff (e. g. , school mental health professionals, school nurses, administrators) Targeted small group interventions for students Suicide risk-screening and/or assessment Approaches that create emotionally and physically safe environments for students Gatekeeper training for staff, students and families Social-emotional learning interventions to enhance protective factors (e. g. , healthy coping, help-seeking) School-wide initiatives to increase protective factors to reduce risk factors (e. g. , bullying prevention, trauma-informed practices reflecting rapport, clarity of expectations, positive reinforcement) School-wide, classroom, and individual-level data collection and analyses

ISF Enhances MTSS Core Features • Effective teams that include community mental health providers • Data-based decision making that include school data beyond ODRs and community data • Formal processes for the selection & implementation of evidence-based practices (EBP) across tiers with team decision making • Early access through use of comprehensive screening, which includes internalizing and externalizing needs • Rigorous progress-monitoring for both fidelity & effectiveness of all interventions regardless of who delivers • Ongoing coaching at both the systems & practices level for both school and community employed professionals
 • Voluntary survey conducted with 6, 8, 10 and 12")
Pennsylvania Youth Survey (PAYS) • Voluntary survey conducted with 6, 8, 10 and 12 grade students to learn about their behavior, attitudes and knowledge concerning risk and protective factors in their lives. • The survey is conducted on an every other year basis and is sponsored through the Pennsylvania Commission on Crime and Delinquency in collaboration with the Pennsylvania Department of Education. • Approximately 75% of school districts in Pennsylvania are projected to conduct the PAYS during the 2017 -18 school year. • Primary focus is on 1) providing school leaders with critical information concerning changes in patterns in the use and abuse of harmful substances and behaviors, and 2) assessing risk factors that are related to undesired behaviors and the protective factors that help guard against concerning behavior.
: Mental Health & Risk")
Case Example: MASD Priorities Reflected in MASD PAYS Data (2015): Mental Health & Risk for Suicide 4 out of 10 students indicted “at times I feel I am no good at all” (41. 4%) 4 out of 10 students indicated “felt sad or depressed most days in the past 12 months” (44. 5%) 2 out of 10 students reported “seriously considered attempting suicide” (21%) Experiences with Bullying 2 out of 10 students reported “being bullied in the past 12 months” (21. 9%) Being Threatened with Violent Behavior 3 out of 10 students report being threatened to be hit or beaten up on school property in the past 12 months (31. 2%) 1 in 10 students report having been hit or beaten up in the past 12 months (13. 9%) Substance Access and Use 4 out of 10 students report having tried beer, wine or hard liquor in past 30 days (41. 3%) 1 out of 2 students report gaining access to alcohol from family / religious celebrations (51. 5%) Nearly 2 of 10 students report “having smoked cigarettes” (19. 4%) Approaching 1 of 10 students indicate “using prescription pain relievers without doctor telling them to take them” (7. 9%) with primary source of those drugs being family or friends Stress Associated with Limited Family Resources 2 out of 10 students report “worrying about the family running out of food” (19. 8%) Almost 1 out of every 10 students indicate having “skipped a meal due to limited family money” (8. 9%)

ISF Enhances MTSS Core Features • Effective teams that include community mental health providers • Data-based decision making that include school data beyond ODRs and community data • Formal processes for the selection & implementation of evidence-based practices (EBP) across tiers with team decision making • Early access through use of comprehensive screening, which includes internalizing and externalizing needs • Rigorous progress-monitoring for both fidelity & effectiveness of all interventions regardless of who delivers • Ongoing coaching at both the systems & practices level for both school and community employed professionals

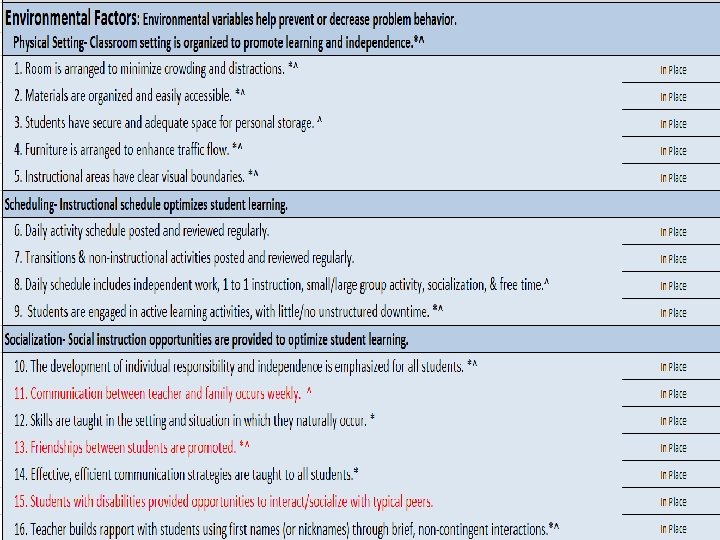
Practice Level: Data Driven Professional Development Universal Prevention Example Four Virtual Modules (coupled with in classroom coaching) * Adverse Childhood Experiences & Trauma * Rapport as a Protective Factor * Positive Reinforcement as a Protective Factor * Social & Emotional Behavior Expectations

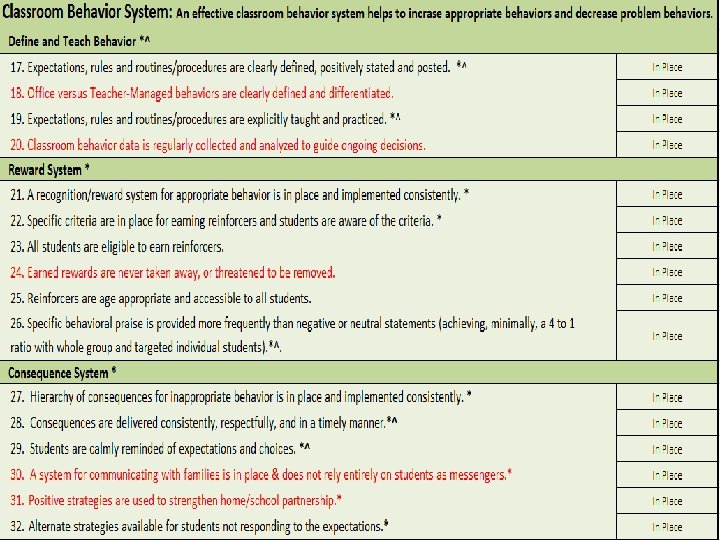
Classroom Assistance Tool

ISF Enhances MTSS Core Features • Effective teams that include community mental health providers • Data-based decision making that include school data beyond ODRs and community data • Formal processes for the selection & implementation of evidence-based practices (EBP) across tiers with team decision making • Early access through use of comprehensive screening, which includes internalizing and externalizing needs • Rigorous progress-monitoring for both fidelity & effectiveness of all interventions regardless of who delivers • Ongoing coaching at both the systems & practices level for both school and community employed professionals

 In conjunction")
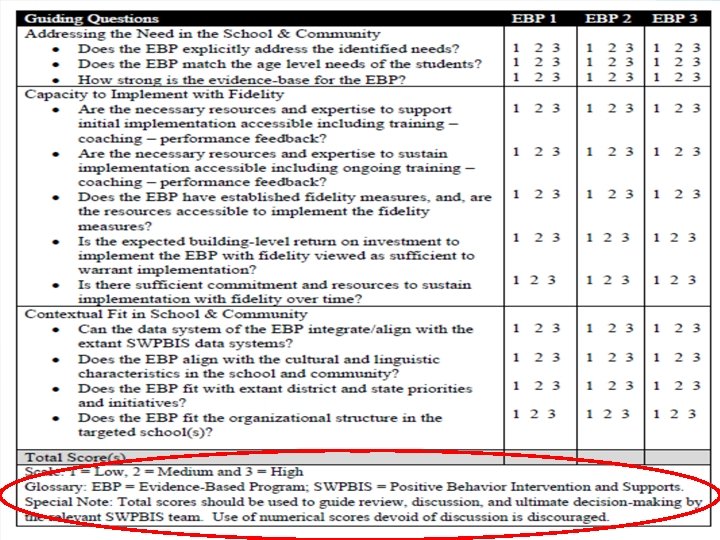
A Hybrid Model v The Hexagon Tool (Blasé et al. , 2013) In conjunction with: v Putnam et al. (n. d. ) 12 Guiding Questions Broad domains: Need of school and community Capacity to implement with fidelity Contextual fit in school and community v Suggested Scoring: Arithmetic average of team members’ ratings on the 12 questions + Hexagon Tool ratings
 • Universal")
Case Example- Selected EBPs Associated with Suicide Prevention • SEL (Positive Action) • Universal Screening (SSRS-IE) • Gatekeeper Trainings (YMHFA & QPR)

Gatekeeper Training Comparison Evidence-based Suicide Prevention Program Features QPR* YMHFA* Length of Training 1. 5 -2 hours 8 hours Format Face to Face (also available virtually) Face to Face Required Text yes ($2. 50 per pamphlet) yes ($18. 95 per text book) Range of Participants 30 -40 maximum (Felxible) 30 maximum (Rigid) Certificate Awarded Yes Time of Trainer to become credentialed 1 Day 3 -5 Days * It is recommended that co-instructors be utilized when providing QPR or YMHFA training.

ISF Enhances MTSS Core Features • Effective teams that include community mental health providers • Data-based decision making that include school data beyond ODRs and community data • Formal processes for the selection & implementation of evidence-based practices (EBP) across tiers with team decision making • Early access through use of comprehensive screening, which includes internalizing and externalizing needs • Rigorous progress-monitoring for both fidelity & effectiveness of all interventions regardless of who delivers • Ongoing coaching at both the systems & practices level for both school and community employed professionals
 Statements / Questions Survey 1 using a Likert")
Impact of YMHFA Training (Part 1) Statements / Questions Survey 1 using a Likert type scale for Responses: To occur between 1 – 4 weeks following initial training (response options are 1= strongly disagree, 2=disagree, 3= agree, and 4= strongly agree). 1) 2) 3) 4) 5) 6) 7) 8) 9) 10) 11) 12) As a result of YMHFA training, I am more aware of how social, emotional and behavioral matters might influence student learning. As a result of YMHFA training, I am more aware of my own social, emotional and behavioral health and well-being. As a result of YMHFA training, I am better able to recognize the signs that a student may be experiencing a mental health challenge. As a result of YMHFA training, I am better able to effectively reach out to a student who may be experiencing a mental health challenge. As a result of YMHFA training, I am better able to assess for risk of immediate harm when interacting with a student who appears to be experiencing a mental health challenge. As a result of YMHFA training, I am better able actively and compassionately listen in a nonjudgmental manner to a student in distress. As a result of YMHFA training, I am better able to offer a student who appears distressed basic “first aid” level mental health information and reassurance. As a result of YMHFA training, I am better able to assist a student who is experiencing a mental health problem or crisis seek professional help. As a result of YMHFA training, I am better able to assist a student who may be experiencing a mental health problem or crisis to connect with appropriate community, peer and personal support. As a result of YMHFA training, I am more aware of my own views and feelings about mental health problems and disorders and how my views and feelings can influence my interactions with my students. As a result of YMHFA training, I am better able to ask a student whether s/he is considering selfinjury and/or suicide. Based on my experiences with initial YMHFA training, I feel sufficiently prepared to provide mental health first aid to a student at school or in the community.
 Statements / Questions Survey 2: To occur between")
Impact of YMHFA Training (Part 2) Statements / Questions Survey 2: To occur between 3 - 4 months following initial training (responses will be in drop down menu form). 1) Since my initial training in YMHFA, have you been more sensitive to the social, emotional and behavioral health needs of your students? (Drop down menu with Yes, No, Uncertain options) 2) Since my initial training in YMHFA, have you applied aspects of the YMHFA action plan referred to as ALGEE (or applied the action plan known as ALGEE in its entirety) with a youth in either school or community settings? (Drop down menu of Yes or No) --------------------------------- Note: The following items become relevant for those who indicated they have applied aspects of the YMHFA action plan or ALGEE in its entirety: 1) 2) 3) 4) 5) 6) 7) Since your initial training in YMHFA, which aspects of the YMHFA action plan known as ALGEE have you applied with a youth? (drop down menu of ALGEE asking them to check all that apply) Since your initial training in YMHFA, have you pro-actively researched/explored local community-based mental health resources to support students in your school? (Drop down menu of Yes or No) With how many students /young people have you applied aspects of the YMHFA action plan or ALGEE in its entirety? (drop down menu of 1 -2, 3 -4, 4 -5, and more than 5 students/youth). When applying aspects of the YMHFA action plan or ALGEE in its entirety, were you able to readily recall the basic steps involved to provide YMHFA to the student/young person/people of concern? (Drop down menu of Yes, No, Uncertain) When providing YMHFA to youth, did you think back to / reference your YMHFA training experience/materials? (Drop down of Yes, No, Uncertain) As a result of your efforts in providing YMHFA, in your own opinion, did your provision of YMHFA have a constructive impact? (Drop down menu of Yes, No, Uncertain) To what degree have you been attentive to your own personal needs for support after providing aspects of the YMHFA action plan or ALGEE in its entirety? (Drop down menu of Yes- I thought about and/or addressed my own needs, Somewhat- I briefly thought about and/or partially addressed my needs, or No-I did not think about or address my own needs)
 Item Strongly Agree/ Agree Strongly Disagree/ Disagree 1)")
Pre-Service Training Example YMHFA (Part 1) Item Strongly Agree/ Agree Strongly Disagree/ Disagree 1) As a result of YMHFA training, I am more aware of how social, emotional, and behavioral matters might influence student learning. 92. 9 % 7. 1% 2) As a result of YMHFA training, I am more aware of my own social, emotional and behavioral health and well-being. 88. 2% 11. 8% 3) As a result of YMHFA training, I am better able to recognize the signs that a student may be experiencing a mental health challenge. 91. 8% 8. 2% 4) As a result of YMHFA training, I am better able to effectively reach out to a student who may be experiencing a mental health challenge. 91. 8% 8. 2 92. 5% 7. 4% 92. 6% 7. 4% 5) As a result of YMHFA training, I am better able to assess for risk of immediate harm when interacting with a student who appears to be experiencing a mental health challenge. 6) As a result of YMHFA training, I am better able actively and compassionately listen in a non -judgmental manner to a student in distress.
 As a result of YMHFA training, I am better able to offer a")
7) As a result of YMHFA training, I am better able to offer a student who appears distressed basic “first aid” level mental health information and reassurance. 91. 3% 8. 6% 91. 7% 8. 2% 91. 8% 8. 2% 88. 3% 11. 8% 92. 5% 7. 4% 89. 4% 10. 6% 8) As a result of YMHFA training, I am better able to assist a student who is experiencing a mental health problem or crisis seek professional help. 9) As a result of YMHFA training, I am better able to assist a student who may be experiencing a mental health problem or crisis to connect with appropriate community, peer and personal support. 10) As a result of YMHFA training, I am more aware of my own views and feelings about mental health problems and disorders and how my views and feelings can influence my interactions with my students. 11) As a result of YMHFA training, I am better able to ask a student whether s/he is considering self-injury and/or suicide. 12) Based on my experiences with initial YMHFA training, I feel sufficiently prepared to provide mental health first aid to a student at school or in the community.
 Number of ALGEE Frequency Elements Used Percentage of")
Pre-Service Training Example YMHFA (Part 2) Number of ALGEE Frequency Elements Used Percentage of Respondents 0 1 1. 5% 1 14 21. 2% 2 14 21. 2% 3 14 21. 2% 4 7 10. 6% 5 16 24. 2% Proportion of Respondents Indicating Using ALGEE Elements Note. N = 66; Percentages may not add up to 100. 0% due to rounding.

Suicide Prevention Video https: //www. youtube. co m/watch? v=3 BByqa 7 bhto
. The hexagon")
References Blase, K. , Kiser, L. , & Van Dyke, M. (2013). The hexagon tool: Exploring context. Chapel Hill, NC: National. FPBIS Project. (2018). Classroom Assessment Tool (CAT). Retrieved from http: //flpbis. cbcs. usf. edu/tiers/classroom. html Runge, T. J. , Knoster, T. P. , Moerer, D. , Breinich, T. , & Palmiero, J. (2017). A practical protocol for situating evidence-based mental health programs and practices within school-wide positive behavioral interventions and supports. Advances in School Mental Health Promotion, 10(2), 101 -112.

Please Provide Feedback Your feedback is important to us! Please take a few moments at the end of the session to complete an evaluation form for this session. Forms are available: • In our mobile application by clicking the link in the session description. • Online underneath the posted presentations at www. pbis. org/presentations/chicago_for um_18

National PBIS Leadership Forum | October 4 -5, 2018, Chicago, IL Please Complete the Session Evaluation to Tell Us What You Thought of This Session

Save the dates, February 20 – 23, 2019 for the… Pre-Conference Workshops FEBRUARY 20 Skill-Building Workshops FEBRUARY 23 Washington, DC Grand Hyatt Washington Breakout Sessions FEBRUARY 21 - 22 Networking | Posters | Exhibits For more information, visit: conference. apbs. org
- Slides: 44