Integrating PostCombat Care into the Patient Aligned Care
 Lucile Burgo, MD National")
Integrating Post-Combat Care into the Patient Aligned Care Team (PACT) Lucile Burgo, MD National Co-Director Post Deployment Integrated Care Initiative Associate Primary Care Director VA Connecticut

Disclosure Statement • I have no conflicts of interest to disclose 2

OUTLINE • Some primary care history • PACT as a framework for “best care” • Post combat care in the PACT • How can the WRIISC help?

VHA Primary Care Milestones 1993 Under Secretary for Health's Letter, Primary Care as a VHA Priority 1994 Guidance for the Implementation Of Primary Care in Veterans Health Administrative (VHA) 1995 Primary Care in VA Primer 1996 Kizer’s Vision for Change and Journey for Change 1998 Guidelines for Implementation of Primary Care 1998 Primary Care Management Module 1999 CPRS (EMR) 2004 Guidance on Primary Care Panel Size 2006 Primary Care Standards 2009 Universal Services Taskforce Report

Primary Care in the VHA Largest integrated health care system in the US Comprehensive electronic medical record >850 sites of Primary Care • 152 Medical Centers • >700 Community Based Outpatient Clinics (CBOC) 4. 8 million primary care patients-each assigned to an individual primary care provider • 53% in CBOCs 12 million encounters/year

VHA Primary Care by Age & Gender 44% 6. 1% Female 21% had encounter in Mental Health 25%
 (5% Trainees)")
VHA Primary Care Providers 7371 Providers, 5008 FTE (Avg. 0. 69 FTE) (5% Trainees) 7

VHA Primary Care Strengths Weaknesses Primary Care Model Team Concept Provider oriented, not “patient-centered” Interdisciplinary decision making unusual Some employees not working at "top of competence” Access: Delays for primary care visits Poor phone service; secure messaging proceeding infrequent slowly; Focus on face-to-face visits Service agreements implemented to Efforts to manage chronic disease to optimize support specialty care interface outcomes still limited Support programs and services (Home telehealth, HBPC) Limited coordination available to manage crucial transitions of care Comprehensive Electronic Medical Record Sub-optimal CPRS user functionality Minimal Decision Support Preventive Care Program Large burden of chronic diseases; Poor health behaviors contribute Health behaviors often not addressed and interventions often not provided Healthcare staff need additional training

Select Emerging National Health Care Delivery Trends • Patient-Centered Care • Access to Care • Exploding consumer information and direct marketing • Electronic Health Records • Personal Health Records • Increasing demand for transparency and quality • Increasing POC Diagnostics and Monitoring at home • Minimally Invasive Procedures • Convergence of Technology • Telehealth and Teleradiology • Social Media 26 September 2020 9 9

Patient Centered Care per IOM Health care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that patient values guide all clinical decisions • • Superb access to care Patient engagement Clinical information systems Care coordination Integrated and comprehensive care Smooth transfer of information Ongoing public information Publicly available information to choose a practice and a physician 10

First Step: American College of Physicians Medical Home Builder N= 850 VHA Primary Care Practices Overall Average Score: 69%

Total Score

Veteran Centered Care Physical Psychological Veteran Psychosocial
 Centered Care • Delivering “health” in addition to “disease")
Essential Transformational Elements: Patient (Veteran) Centered Care • Delivering “health” in addition to “disease care” • Veteran as a partner in the team – – Empowered with education Focus on health promotion and disease prevention Self-management skills Patient Advisory Board • Efficient Access – Visits – Non face-to-face • Telephone • Secure messaging • Telemedicine • Others? 14

Essential Transformational Elements: Comprehensive Team-based Care • Redesign Primary Care Practice – – – Tasks and relationships defined Redesign team member functions and tasks Improve Team Dynamics Build team roles to support a Chronic Care Model Working at top of competency Time for non-face to face activities • Encourage Primary Care staff professional growth – Leadership opportunities – Teaching opportunities – On-the-job provider training for comprehensive Primary Care • Women’s health • Pain management • Post-deployment health • Geriatrics • Specialty experience

Essential Transformational Elements: Coordination of Care • Improved coordination for all transitions Inpatient and outpatient Primary Care and Specialty Care VA and non-VA co-management (Dual Care) Incorporate telehealth and Home Based Primary Care (HBPC) services – Highlight home care & rural health – – • Care Management – Panel based – Connecting all services and points of care – Care across the continuum

Essential Transformational Elements: Case/Chronic Disease Management • Chronic Care Model – – – – Disease management Interface with specialty care Case managers Pain management Returning combat Veteran Depression Substance abuse • Disease registries – Identification of outliers – Veterans at high risk for adverse outcomes

Essential Transformational Elements: Technology • Improve technological clinical support – – – CPRS user-friendliness Decision support PCMM enhancements Predictive modeling Information processing • Telephone Support • My Healthe. Vet – Secure Messaging
 Community Health System")
CHRONIC CARE MODEL Ed Wagner & Institute for Healthcare Innovation (IHI) Community Health System Resources & Policies Health Care Organization Self. Management Support Informed, Activated Patient Delivery System Design Productive Interactions Decision Support Clinical Information Systems Prepared, Proactive Practice Team Functional and Clinical Outcomes

Personal Health Care Building a Relationship Provider skills • Cultural competency • Motivational interviewing • Enhanced communication skills • Managing disagreement Self Management Patients, not health care providers, are the primary managers of their health conditions • Education • Support Tools • Resources • Home Telehealth, My Healthe. Vet, Other tools • Preferred means of communication • Involving families and caregivers • Respect, Dignity, and Trust • Continuity • Clinical Management • Provider/Team • Information Patient-Centered Perspective Shared Decision Making Preference centered health care choice made by the patient together with the provider • Education • Decision Support Tools • Resources Patient Participation • New patient orientation • Personalized brochures • Staff information • Patient advisory board • Focus groups

PATIENT ALIGNED CARE TEAMS Replaces episodic care based on illness and patient complaints with coordinated care and a long term healing relationship Takes collective responsibility for patient care Is responsible for providing all the patient’s health care needs THE PRIMARY CARE TEAM Arranges for appropriate care with other specialties

VETERAN CENTERED, TEAM BASED, COORDINATED CARE PATIENT ALIGNED CARE TEAM PACT Care Coordination & Care Management Team Function and Culture Veteran VA (VHA and VBA) 22

Pillars of the Medical Home Patient-Driven • The primary care team is focused on the whole person • Patient-preferences guide the care provided to the patient Team-Based • Primary care is delivered by an interdisciplinary team led by a primary care provider using facilitative leadership skills Efficient • Veterans receive the care they need at the time they need it from an interdisciplinary team functioning at the highest level of their competency Comprehensive • Primary care serves as point of first contact for a broad range of medical, behavioral and psychosocial needs, fully integrated with other VA health services and community resources Continuous • Every patient has an established and continuous relationship with a personal primary care provider Communication • The communication between the Veteran patient and other team members is honest, respectful, reliable, and culturally sensitive Coordinated • The PCMH team coordinates care for the patient across and between the health care system including the private sector

24

25
 National Staffing Ratio Support Staff/PC FTE 2. 70 2. 60 2.")
Primary Care (PCMM) National Staffing Ratio Support Staff/PC FTE 2. 70 2. 60 2. 50 2. 40 2. 30 2. 20 2. 10 2. 00 Mar-10 Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10

Primary & Specialty Care: Becoming True Partners Shared Goals • Every Veteran gets optimal care • Primary & Specialty Care share same platform • Mutual communication & training • Everyone is responsible to achieve desired outcomes 27 Shared Agenda • Service “friendship” agreements • Who takes care of what? • Educate/mentor primary care champions • Forging a true “Learning Organization”

In the end we know… Primary care is best when it does these four things well: Access • I can get care when and how I need it Relationship over time Comprehensive services • I have a Team who knows me as a person • My Team takes care of the bulk of my needs Coordination • My Team coordinates any care I need in the health system

If Primary Care does those things well, then patients who receive care in those practices…. Are less likely to: • End up in the hospital • End up in the emergency room • Miss days from school or work And are more likely to: • Have preventive care needs met • Have good control of their chronic conditions • Say they understand their conditions • Receive good help from their practice
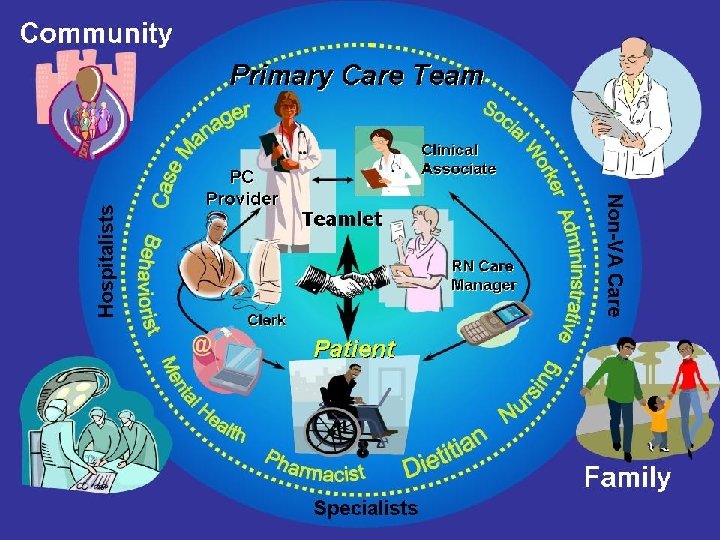

Other Team Members Clinical Pharmacy Specialist: ± 3 panels Clinical Pharmacy anticoagulation: ± 5 panels Social Work: ± 2 panels Nutrition: ± 5 panels Case Managers Trainees Integrated Behavioral Health Psychologist ± 3 panels Social Worker ± 5 panels Care Manager ± 5 panels Psychiatrist ± 10 panels Other Team Members For each parent facility Health Promotion Disease Prevention Program Manager: 1 FTE Health Behavior Coordinator: 1 FTE My Healthe. Vet Coordinator: 1 FTE Teamlet: assigned to 1 panel (± 1200 patients) Monitored via Primary Care Staffing and Room Utilization Data • Provider: 1 FTE • RN Care Mgr: 1 FTE • Clinical Associate (LPN, MA, or Health Tech): 1 FTE • Clerk: 1 FTE Patient The Patient’s Primary Care Team Panel size adjusted (modeled) for rooms and staffing

Patient-Centered Primary Care Model Implementation Strategies • Start-up resources – Gap analysis – Funding to support new staffing model • Team retraining and redesign – PCMH Summit, April 2010 – Learning Collaboratives • Medical Home including Chronic Disease • Telephone Care – Medical Home Learning Centers • Primary Care Team Dynamics • Care Management and Coordination – Consultation Teams • Demonstration “Laboratories” • Intensive research and effectiveness evaluation • Communication and Education • Informatics and Technology • Measurement

Patient Centered Prevention and Population Based Team Work Patient. Aligned Care Team Provides Value Continuous Improvement Data Driven, Evidence Based

Learning, Discovery, Continuous Improvement Readiness Assessment Staffing Support • ACP Medical Home Builder • Primary Care Staffing Training and Education • PCMH Summit • PACT Collaborative • TILC (Transformation Initiative Learning Centers) • Consultation Teams Demonstration Labs Measurement: PACT Compass IT Improvements Communication • Access • Continuity • Patient Engagement/Satisfaction • Coordination • Panel Management • Clinical Improvement • PCMM enhancements • CPRS enhancements • Identify high risk patients • Secure Messaging • MHV • Staff • Patients • Stakeholders Implementation Guidance and Support Centers of Excellence in Primary Care Education • PACT Handbook • Workload capture • Protocols PACT Certification Specialty Integration

Patient Aligned Care Team for Returning Combat Veterans Patient centered, team based, integrated care Evidence based, continuously improving care Communication Combat Veteran Care/Case Manager Collaboration Coordination Post-Combat Care moves our PACTs forward The PACTs move our Post-Combat Care forward

Post Deployment Care for Recent Combat Veterans ESSENTIAL ELEMENTS FOR CARE • Comprehensive psychosocial and medical intake performed on all veterans: Ideally Medical, Mental Health and Social Work see every new patient at the first visit. • PACT and extended team(MH, SW) trained and have tools to accomplish this • Integrated, de-stigmatized MH treatment • Active participation by OEF/OIF program staff and specialized teams in mental health, polytrauma, pain, SA featuring full integration of all post deployment services • Close links to allied clinics and programs • Align resources around Veteran • Integrated team meets to formulate Veteran centered care plan • Extended hours availability 36

Post Deployment Care for Recent Combat Veterans • The PACT will have tools and training to accomplish comprehensive intake ongoing support and coordination of post deployment care – Teamlet: Primary Care Provider(s), RN care manager, clinical associate, and clerk trained in combat Veterans unique needs – Extended team: PACT social worker, PC-MHI, pharmacist trained in combat Vet unique needs – OEF/OIF program : trains and supports PACT joining core team when needed – PDICI champions assist with facility education and consultative support of PACT – Coordination with specialty care: Polytrauma, PTSD, Pain, Ortrho, Rehab, Neurology, WRIISCs, (join the Veteran’s team) 37

TASKS FOR POST DEPLOYMENT CARE IN THE PACT ESSENTIAL ELEMENTS FOR CARE IN THE PACT – Risk assessment at each encounter F 2 F and non F 2 F – Proactive visit needs assessment by teamlet (prescreens? )to coordinate services on day of visit (MH, SW, 2 ary TBI, specialty care, labs, xrays) – Orientation to team, roles understood, partnership with Veteran – Assist with MHV-IPA, discuss communication methods (SM, telephone), demonstrate web resources – Weekly (extended) team huddles for complex cases – Assure knowledge of/connection to OEF/OIF program for each combat Vet 38

TASKS FOR POST DEPLOYMENT CARE IN THE PACT – Initiate appropriate assistance from OEF/OIF program manager and social worker, primary care champions, Consultative Team • • • Benefits, C+P Legal assistance Vet centers Case management Community resources and services Schools – Assure coordination of care with specialty clinics and programs especially Polytrauma, pain, substance abuse, specialty mental health(PTSD), physical therapy, orthopedics, neurology(points of contact, service agreements) – Consider care provision via telehealth ( telerehab, telepain , video conferencing), group visits for orientation, intake 39

VBA C+P PT Ortho Substance Abuse Pain Vet Centers PIDICI Champ DHC NCPTSD 9/26/2020 Core Team members • Clinical Pharmacy Specialist: ± 3 panels • Clinical Pharmacy anticoagulation: ± 5 panels • Social Work: ± 2 panels • Nutrition: ± 5 panels • Case Manager • Integrated Behavioral Health • Psychologist ± 3 panels • Social Worker ± 5 panels • Care Manager ± 5 panels • Psychiatrist ± 10 panels Teamlet PCP Clinical Associate (LPN, MA, or Health Tech) Clerk RN Care Manager OEF/OIF/OND Program staff PM/CM/SW Veteran PACT can care for special populations with support and training. The PACT expands as needed to meet the Veteran’s needs. We the team cares for the CV. WRIISC Chaplain Specialty Mental Health Polytrauma Neurology OEF/OIF/OND Consult Team 40

Where do the WRIISC fit in? • 80 -90% of Veterans have a primary care provider: longitudinal relationship of trust and connection • Over 50% are cared for in CBOCs/rural sites: poor access to specialty care • 35% of OEF/OIF/OND cared for in CBOCs • Focus groups : Vets want teams who understand their culture, their experience , thus we need more training, expectation of basic knowledge base in PACT • Risk assessment and communication and better communication skills are essential competencies • PACT with Veteran at the center is your stakeholder

How will the WRIISC best support the PACT? • PACTs need education and consultative support. • VA SCAN pilot • Exposure conferences • On site provider training • Virtual consultative service for MUS, exposure concerns ? • Comprehensive assessment complex cases

PC PROVIDER CLINICAL ASSOCIATE TEAMLET CLERK NCPTSD RN C A R E MANAGER WRIISC FAMILY 43

PACT Resources • http: //vaww. infoshare. va. gov/sites/primaryca re/mh/pcmhinfo/default. aspx
- Slides: 44