Integrated Basic Science Review Reproductive SystemA Dr Paul

Integrated Basic Science Review Reproductive System-A Dr. Paul S. Anderson Copyright – Medical Board Review Services

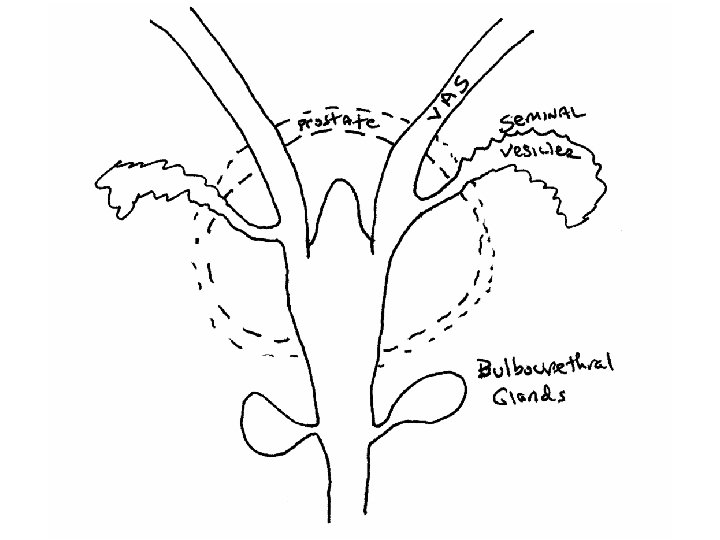
Penile Anatomy:

REPRODUCTIVE PHYSIOLOGY : MALE SYNTHESIS OF TESTOSTERONE IN THE TESTES

METABOLISM – SEX STEROIDS - 1

REPRODUCTIVE PHYSIOLOGY : MALE HORMONE SYNTHESIS AND CONTROL

METABOLISM – SEX STEROIDS - 2 • MECHANISM OF ANDROGEN ACTIONS

REPRODUCTIVE PHYSIOLOGY : MALE ACTIONS OF ANDROGENS

REPRODUCTIVE PHYSIOLOGY : MALE ANDROGEN PHYSIOLOGY

MALE PATHOLOGIES - 1 • Specific Urethritis: GC, males>pain, dysuria, purulent dc, frequency • Non-Specific Urethritis: Chlamydia, ureaplasma, E. coli, mild sx, urethral stricture, spread of infection to prostate, epididymis • HHV / HSV: Sexually transmitted. May be slowly or quickly symptomatic. • Syphilis: STD. Primary, secondary, and tertiary stages. (See micro notes) • Penile Inflammation: balanitis, usu in pts. with phimosis or redudant prepuce, staph, E. coli, candida • Penile Tumors: condyloma acuminatum, HPV 6 & 11, benign, sexually transmitted • Hypospadius & Epispadius: congenital misplacement of urethral canal ventrally or dorsally, may be associated with undescended testicles, may cause urinary obstruction or inability to inseminate • Phimosis: orifice of prepuce is too small to permit retraction. Also applies to inflammatory fusion of the foreskin to the glans. • Paraphimosis: prepuce is retracted & won’t replace • Klinefelter’s: male hypogonadism, 2 or more X chromosomes and 1 or more Y chromosomes • Cryptorchidism (UNDESCENDED TESTES): usu unilateral, even if corrected have increased risk of infertility & testicular cancer

MALE PATHOLOGIES - 2 • Epididymititis & Orchitis: assoc, with lower UTI & prostatitis, GC or Chlamydia in men under 35; E. coli & pseundomas in men over 35; mumps 1 wk after onset • Varicocele: scrotal varicosity, abnormal dilation & tortuosity of pampiniform plexus of veins, 99% left-sided, may cause infertility, sx corrected, bag of worms • Hydrocele: accumulation of serous fluid in scrotum, occurs developmentally in descent of testis or secondary to inflammations, painless, enlarged fluctuant scrotum • Hematocele/Torsion: blood in scrotal sac, dt trauma or sx, spontaneous in atherosclerosis, DM, scurvy, syphilis, tumors, will not transilluminate • Seminoma: most common tumor with cryptorchidism, best prognosis of testicular tumors, metastasis to lymphatics, some have increased HCG

MALE PATHOLOGIES - 3 • Bacterial Prostatitis: e. coli & other gram negative rods, staph, GC, dysuria, fever, tender, boggy prostate, painful; chronic prostatitis > mb asymptomatic or low backpain, dysuria, positive culture in expressed secretions, tx difficult • Chronic Abacterial Prostatitis: mostly common, Chlamydia, ureaplasma, no hx of recurrent UTI, 15 WBC per hpf, cultures negative • BPH/Nodular Hyperplasia: discrete nodules in periurethral area middle & lateral lobes, partial or complete obstruction, TURP sx, dihydrotestosterone causes hyperplasia • Carcinoma of Prostate: most common cancer of men, usu posterior lobe, hematogenous spread is mainly to lumbar spine, femur, pelvis, thoracic spine, ribs; local invasion, blacks higher incidence, PSA is marker

FEMALE PATHOLOGIES - Cervix • Acute Cervicitis: – GC, Chlamydia, trichomonas, procedures: – Cervical motion tenderness + mucopurulent dc • Chronic Cervicitis: – Vaginal bacterial overgrowth causing irritation of cervix, transformational zone • rarely symptomatic / may cause pelvic pain • CIN: (Cervical Intraepithelial Neoplasia) – Mostly benign dysplasia in transfomational zone – CIN I (Mild), CIN II (Moderate), CIN III (severe) dysplasia • Cervical Cancer: – HPV 16, 18, 31, 33…. – Exposure relayed spread: • Early age first intercourse • Multiple sexual partners
")
FEMALE PATHOLOGIES - Cervix • CIS: Carcinoma in situ – (In place, no invasion) • Cervical Squamous Cell Carcinoma: – 90% of cervical cancers – Peak age 40 -60. – Stage I-IV spread and prognosis: • Stage I 80% 5 yr survival • Stage IV has a 10 -15% 5 yr survival • Most are asymptomatic • *** Bleeding post intercourse can be a common sign

FEMALE PATHOLOGIES – Endometrium • Acute Endometritis: bacterial infection group A strep, staph following delivery or miscarriage • Chronic Endometritis: PID, IUDs, TB, Chlamydia • Endometrial Hyperplasia: mb precursor to endometrial cancer, PCO, prolonged estrogen effect • Endometriosis: endometrial cells outside of uterus. May fall anywhere, Ovary and adnexa are most common. • Endometrial Polyps: May be estrogen receptive or. Tamoxifen induced. Not considered precancerous. Cause menorrhagia.

FEMALE PATHOLOGIES – Uterus • Leiomyoma / Fibroid: – Most common tumor in women, –Estrogen dependent –Fibroid in myometrium –Asymptomatic or symptomatic: • Compressive Sn/Sx • Bleeding • Urinary frequency • Infertility

FEMALE PATHOLOGIES – Uterus • Uterine Adenocarcinoma: – Most common invasive cancer of female tract – Higher association: • Age 55 -65 • Obesity • DM • Hypertension • Nulliparous – *** Suspect when postmenopausal women starts bleeding

FEMALE PATHOLOGIES - Ovary • Oophoritis: – Inflammation of ovaries; uncommon • Follicular Cysts: – Common, physiologic, may cause pelvic pain. – • Luteal Cysts: – Normal, may rupture into peritoneum & cause inflammation • PCO/Stein-Leventhal Syndrome: – Hyperprolactinemia, Androgen excess, young women – Menstrual disorders, inability to conceive, hirsuitism

FEMALE PATHOLOGIES - Ovary • Tumors of Ovaries: – 80% are benign cysts – Malignant dz. increases after 40 yrs – Risk: • BRCA and other genetic markers • Nulliuparous – May be more fatal due to: • Usually asymptomatic – Dx. At high grade / Stage • May have GI Sx • Marker of known disease: serum CA 125 in 80%
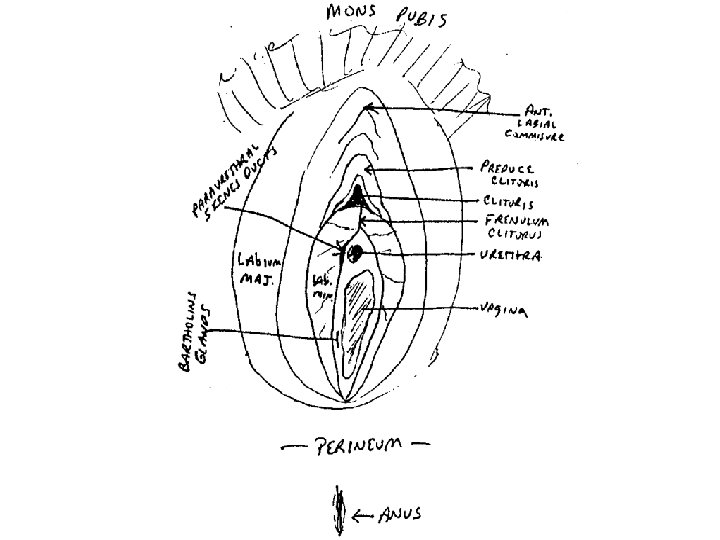

FEMALE PATHOLOGIES - Vulvovaginal • Bartholin’s Cysts: usu assoc, with PID, swelling of gland on wall of vestibule at base of labia majora; GC • Vulvar Dystrophy/Leukoplakia: inflammation, opaque, white scaly plaque, biopsy to find cause • Lichen Sclerosus/Chronic Atrophic Vulvovaginitis: after menopause, skin parchment like, vaginal mucosa thinned, dryness, discomfort • Squamous Hyperplasia: if atypia exist is pre-cancerous or cancerous > VIN, biopsy • Carcinoma & VIN: assoc. with HPV 16 & 18 • Gartner’s Duct Cysts: common, lateral wall of vagina, Wolffian duct remnants • Vestibular Adenitis: glands in posterior vestibule may become inflammed, idiopathic • Clear Cell Adenocarcinoma: in women whose mothers took DES during pregnancy, upper third of anterior vaginal wall or cervix, vaginal adenosis is precursor, no symptoms

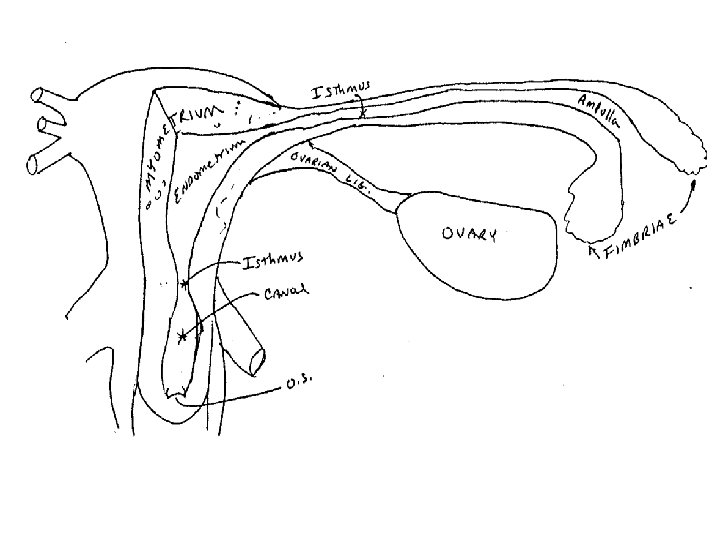
REPRODUCTIVE PHYSIOLOGY : FEMALE

REPRODUCTIVE PHYSIOLOGY : FEMALE MENSTRUAL CYCLE
 SEX STEROIDS - 3")
METABOLISM – (Ovarian) SEX STEROIDS - 3

REPRODUCTIVE PHYSIOLOGY : FEMALE PHYSIOLOGICAL ACTIONS OF ESTROGENS

REPRODUCTIVE PHYSIOLOGY : FEMALE PHYSIOLOGICAL EFFECTS OF PROGESTERONE

REPRODUCTIVE PHYSIOLOGY : FEMALE HORMONE CHANGES IN MENOPAUSE • Between the ages of 40 and 55 the levels of Ovarian estrogen and progesterone production decline. • Average in U. S. is 52 • Ovulation becomes less frequent, then ceases. • FSH and LH are uninhibited, and rise. • Estrogens and Progesterone decline • Androgens may decline or rise, based on Adrenal function. • Adrenal hormone production dominates. • All hormone fractions do not decline at the same rate
 conditions: – Congenital nipple inversion –")
FEMALE PATHOLOGIES – Breast -1 • Breast (benign) conditions: – Congenital nipple inversion – Galactocele (cyst in lactiferous duct or lobule) • Acute Mastitis: bacterial infection of lactating breast, staph, fever • Mammary Duct Ectasia: dilation of lactiferous ducts, usu multiparous women 50 -60 yrs. , mb abnormal mammogram • Fibrocystic Breast Dz: excess estrogen, methlyxanthines, age 20 -40, solitary, most cyst freely moveable, painful / changes with cycle, no increased risk of cancer • Fibroadenoma: most common benign tumor of breast in women under 30, solitary, discrete, moveable, upper outer quadrant

FEMALE PATHOLOGIES – Breast -2 • Carcinoma: in ductal & glandular tissue: – Number 1 female cancer – Family hx; • Mutation of BRCA 1 gene – Estrogen: • Early menarche / late menopause • Nulliparous • Paget’s Disease of the Breast: – Late stage infiltrating carcinoma causes inflammation of the tissue on the nipple. – Typically older patients. – Poor prognosis (sign of advanced disease).

FEMALE PATHOLOGIES – Breast-3 Anatomical locations of selected breast disorders
- Slides: 31