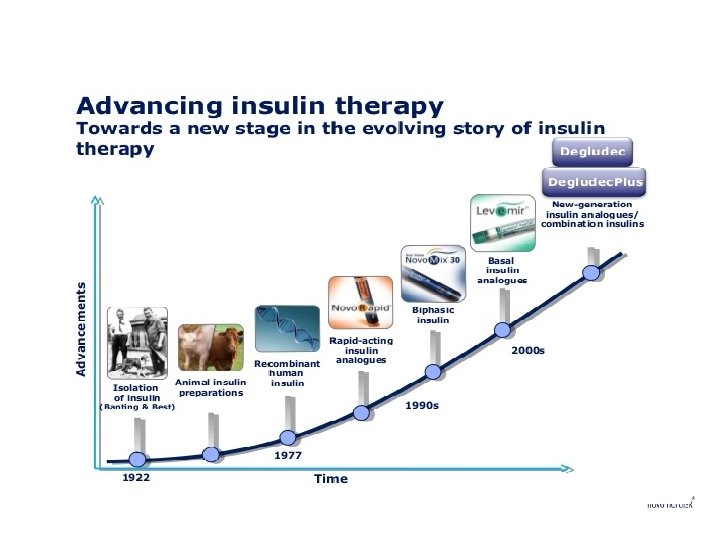
Insulin therapy type 1 diabetes The loss of



Insulin therapy
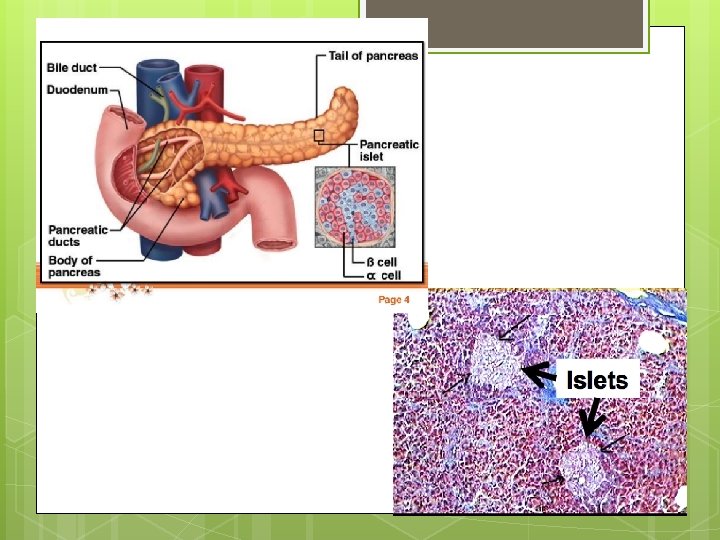

type 1 diabetes The loss of pancreatic function is a hallmark for the diagnosis of T 1 DM and is the reason , insulin is a necessary treatment modality for patients with that form of the disease. vol 32 , No 2 , 2014. clinical Diabetes

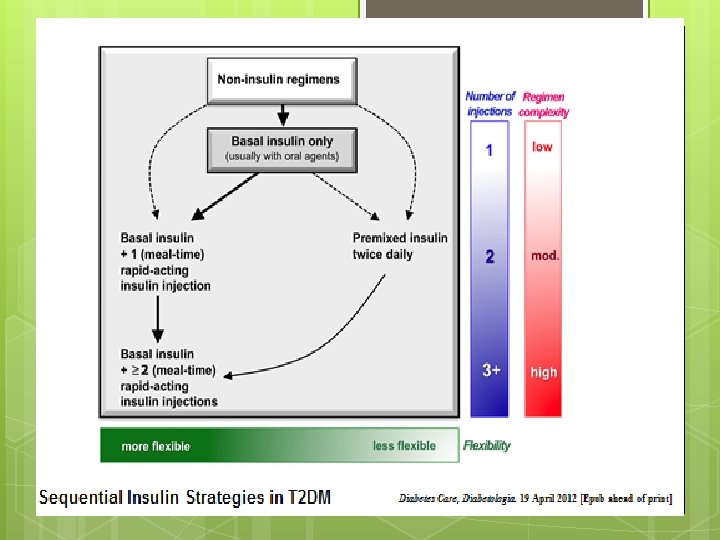
Indications of Insulin therapy Most people with type 1 diabetes should be treated with multiple-dose insulin (MDI) injections ( 3 – 4 injections per day of basal & prandial insulin) or continuous subcutaneous insulin infusion (CSII). [A]

T 2 DM Type 2 diabetes is also partially defined by a loss of pancreatic function. At the time of diagnosis of type 2 diabetes , ~ 50% of pancreatic function is already lost.

T 2 DM is a progressive loss that continues throughout treatment , leading to poor glycemic control and its associated complications. This The continued decline of β-cell function results in the need for medication(s) and eventually exogenous administration of insulin for type 2 diabetes.

T 2 DM Many patients with type 2 diabetes eventually require and benefit from insulin therapy. q The progressive nature of type 2 diabetes and its therapies should be regularly and objectively explained to patients.

ﺍﻧﺴﻮﻟیﻦ ﻣﻮﺛﺮﺗﺮیﻦ ﺩﺍﺭﻭ ﺩﺭ کﻨﺘﺮﻝ ﻗﻨﺪ ﺧﻮﻥ ﺍﺳﺖ Hb. A 1 c % Decrease in Hb. A 1 c: Potency of monotherapy Nathan et al. , Diabetes Care 2009; 32: 193 -203. Prese ntatio n title

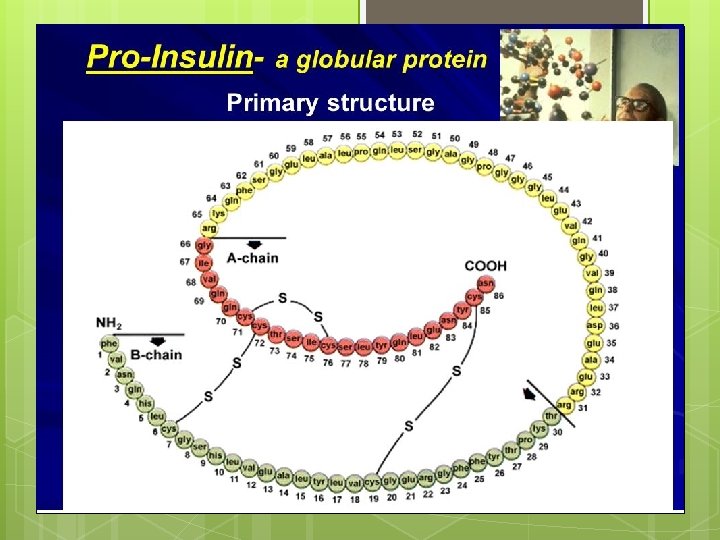
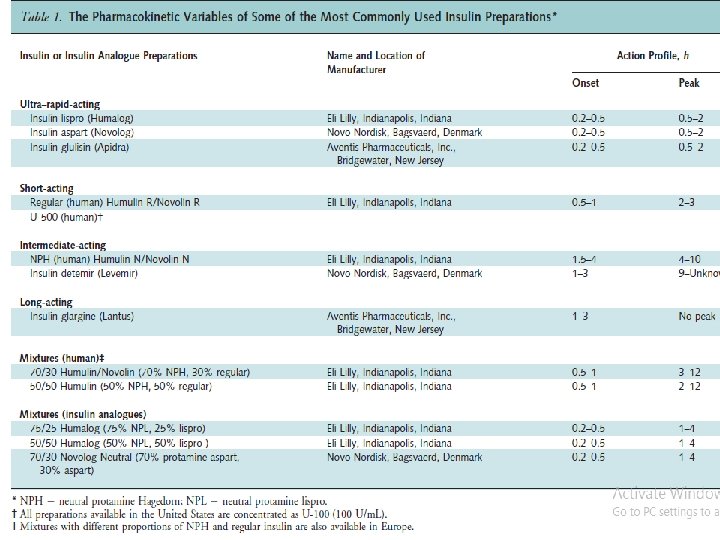
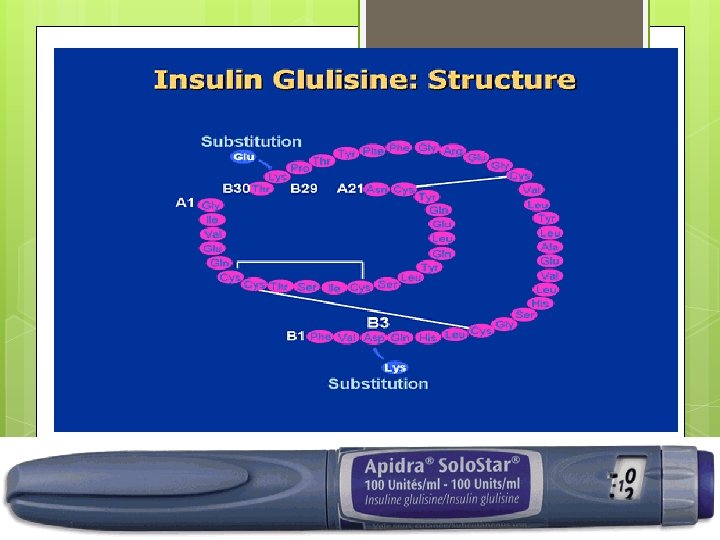
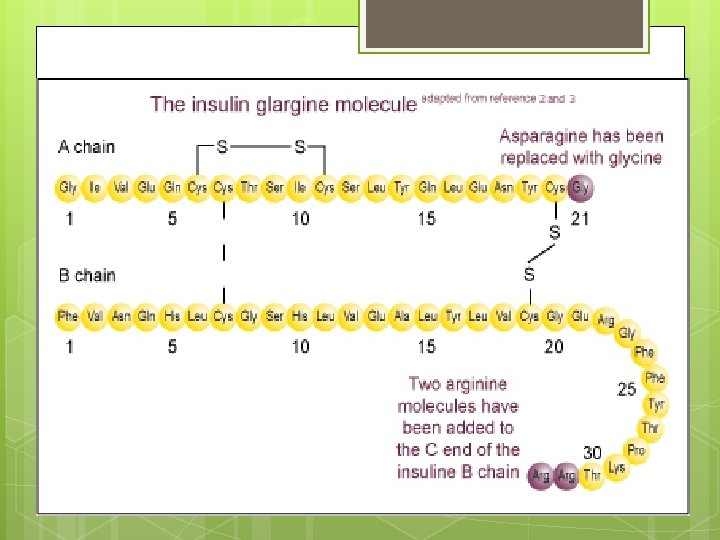
Insulin Preparations • Current insulin preparations are generated by recombinant DNA technology and consist of the amino acid sequence of human insulin or variations thereof. • In the United States, most insulin is formulated as units/m. L). U-100 (100

 Peak (h) (")
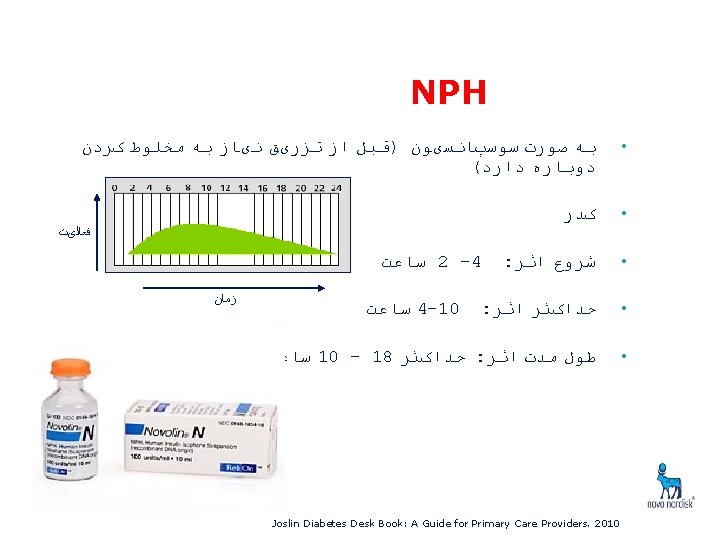
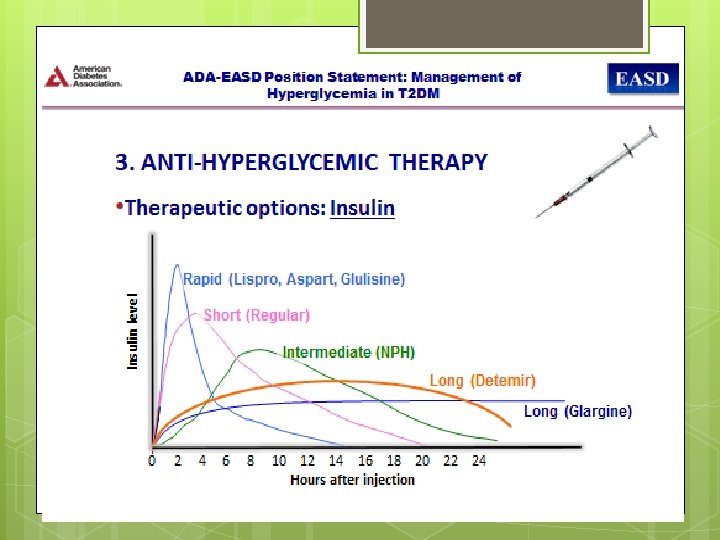
ﺍﻧﻮﺍﻉ ﺍﻧﺴﻮﻟیﻦ Onset of Action Insulin Duration of Action (h) Peak (h) ( )ﺳﺮیﻊ ﺍﺛﺮ Aspart/Glulisine/ Lispro 10 - 15 min 1 -2 3 -6 ( )کﻮﺗﺎﻩ ﺍﺛﺮ Human Regular 30 - 60 min 2 -4 6 -8 4 -8 12 - 16 ( )ﻣﺘﻮﺳﻂ ﺍﺛﺮ Human NPH 1 -2 h ( )ﻃﻮﻻﻧی ﺍﺛﺮ Detemir(Levemir®)* Insulin Glargine(Lantus) Up to 24 2 -4 h - Up to 24 Mudaliar S et al. Endocrinol Metab Clin North Am. 2001; 30: 935 -982. ; 2. Endotext. com * Levemir®; Locally approved labeling in Iran version (STF Q 2 2014)


Aspart Insulin

Insulin Lispro

Detemir


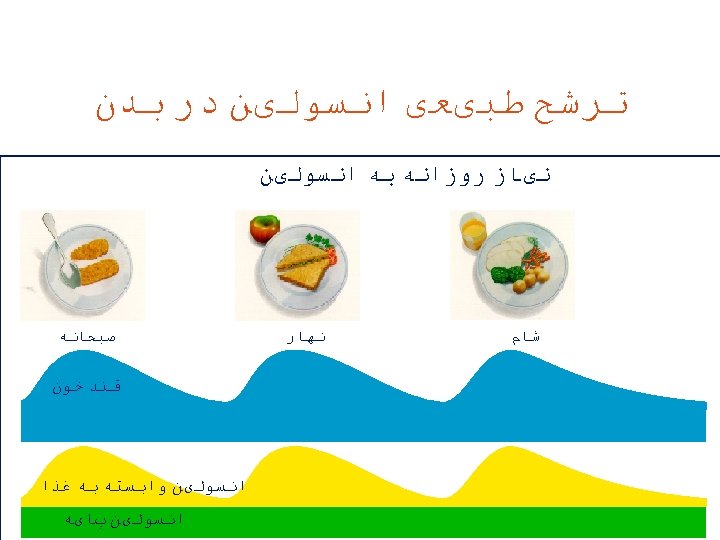
Basal Insulin Basal therapy includes long- and intermediate acting insulin products used to mimic physiological insulin secretion in the absence of food.

Bolus Insulin Rapid- and short-acting insulin products constitute bolus therapy , which is used to mimic the secretion of insulin from the pancreas in response to food. ( postprandial )

Rapid-acting insulin The rapid-acting insulin analogues should be injected 5 to 15 minutes before a meal. in infants or in older adults with dementia who both have unpredictable eating patterns , rapid-acting analogues can be administered after the meal without excessive deterioration of glycemic control. However,
 after subcutaneous injection")
Rapid-acting insulin These insulin analogues are rapidly absorbed ( 30 minutes) after subcutaneous injection , peak at 1 hour, and have a shorter duration of action (3 to 4 hours) than regular insulin. Furthermore, the intraindividual variability in time to maximum serum insulin concentration is clinically significantly less for rapid-acting insulin analogues than for regular human insulin preparations.

ADA Standards of Medical Care in Diabetes— 2017 Although oral therapy is generally the preferred option for most patients with type 2 diabetes at diagnosis, the progressive loss of β-cell function means that insulin replacement therapy will eventually become necessary for many patients.

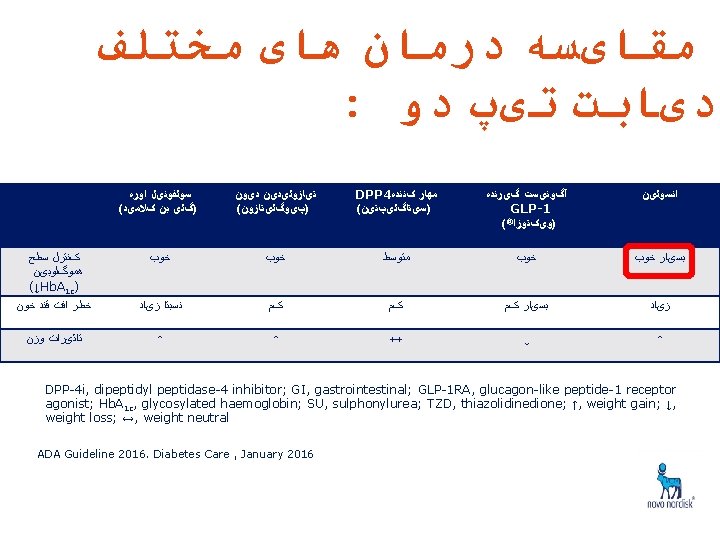
ADA/EASD 2017 Position Statement The ADA/EASD guidelines support the use of patient specific insulin therapy to achieve a glycemic profile as close to normal as possible while minimizing adverse effects such as weight gain and hypoglycemia.

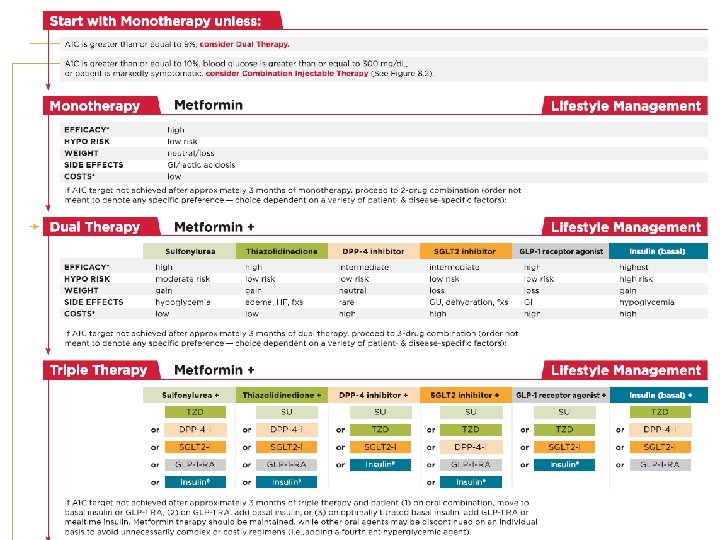
ADA/EASD 2017 Position Statement In accordance with the ADA standards of care , the ADA/EASD generally recommends oral therapy as first-line treatment for patients newly diagnosed with type 2 diabetes , typically initiating with one agent.

After ~ 3 months of monotherapy, providers may consider a second oral agent , the addition of a glucagon-like peptide-1 (GLP-1) receptor agonist , or the addition of basal insulin if glycemic goals are not attained.

The ADA/EASD guidelines reference certain situations in which immediate initiation of insulin therapy is likely indicated : 1 – specifically in patients who exhibit significant symptoms of hyperglycemia 2 - in those who present with drastically elevated plasma glucose levels (i. e. , > 300– 350 mg/dl) or A 1 C (i. e. , ≥ 10– 12%).

immediate initiation of insulin therapy : Some patients may require immediate multiple daily insulin doses rather than a more gradual progression in to insulin therapy.

Initiation of Insulin therapy 3 - When catabolic features , including : weight loss or ketonuria , are present , implementation of insulin therapy is considered mandatory.

Initiation of Insulin therapy 4 – Pregnancy & T 2 DM 5 – Surgery & T 2 DM 6 – ICU Admission & T 2 D 7 – NKHS & T 2 DM 8 – – Sepsis ; SIRS ; High Grade Burns & T 2 DM
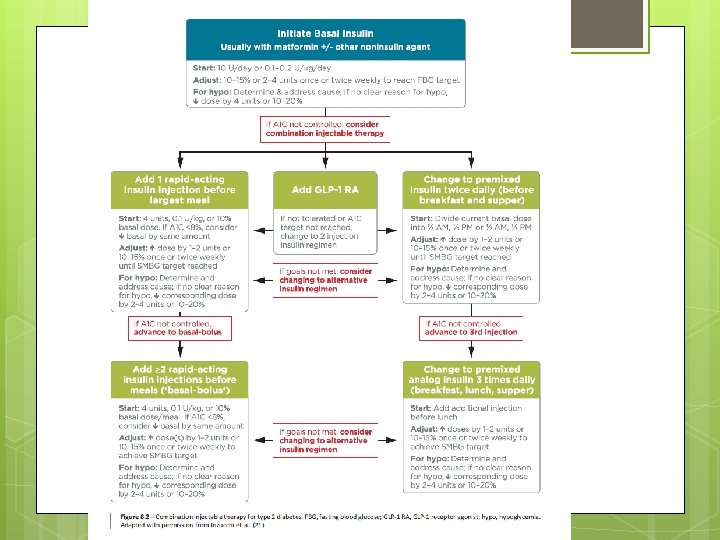

Basal Insulin & T 2 DM However, in patients with more severe hyperglycemia (undefined by the guidelines), therapy can begin with larger doses of 0. 3– 0. 4 units/kg/day.

Glargine & Detemir An advantage of both glargine and detemir is that they have been shown to cause less nocturnal hypoglycemia than NPH.

The ADA and suggest : That EASD elevations in postprandial glucose may be a contributing factor to elevated A 1 C when fasting glucose levels are at goal.

Bolus insulin When therapy basal insulin is not sufficient to maintain glycemic control, bolus insulin therapy with short-acting ( human regular ) or rapid-acting ( aspart , lispro , and glulisine ) insulin just before meals is recommended.

Bolus insulin therapy Rapid-acting insulins offer better postprandial glucose control than regular human insulin, likely because of their pharmacokinetic parameters. Nevertheless , cost considerations still make regular human insulin a viable option in cases in which cost containment is an issue and prandial insulin therapy is required.

When ? ? Providers should be aware that when a patient’s daily dose of basal insulin becomes > 0. 5 units/kg/day , the need for intensification with bolus insulin increases.

First prandial insulin q The guidelines suggest initiating prandial insulin with a single dose just before the meal that contains the largest carbohydrate content of the day. q For most patients , this is the evening meal.

Prandial Insulin From there , a second and third injection may be added before the other two meals if they require additional coverage to limit glucose excursions.

Premixed insulin However , some patients , such as those with a history of nonadherence to their diabetes treatment regimen , may not be appropriate candidates for basal - bolus therapy. q In such cases , premixed insulin products are available to increase convenience but come with the drawback of reduced flexibility in dosing.

Premixed Generally, insulin such products are dosed twice daily , before the morning and evening meals.

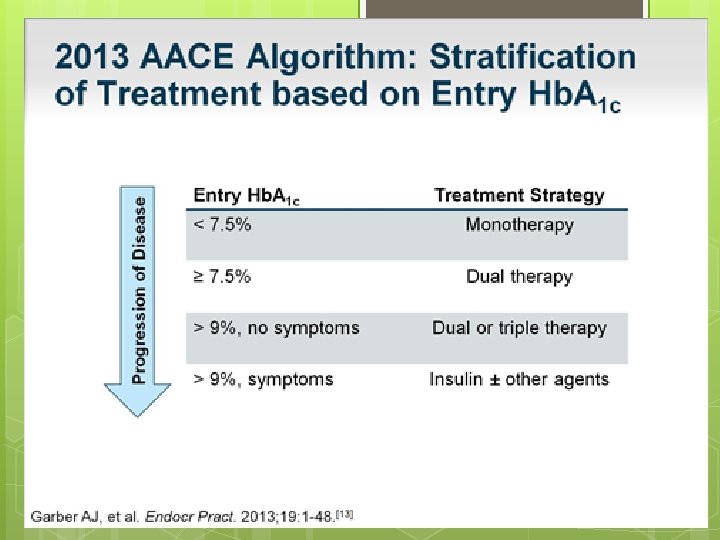
AACE guidelines Current AACE guidelines recommend initiation of insulin therapy for patients whose A 1 C level is > 9% and those who have not achieved their glycemic targets with combination oral therapy.

AACE v. Basal Insulin : For those with an A 1 C > 8% , a higher weight - based dose of 0. 2– 0. 3 units/kg/day is recommended , as opposed to the standard 0. 1– 0. 2 units/kg/day.

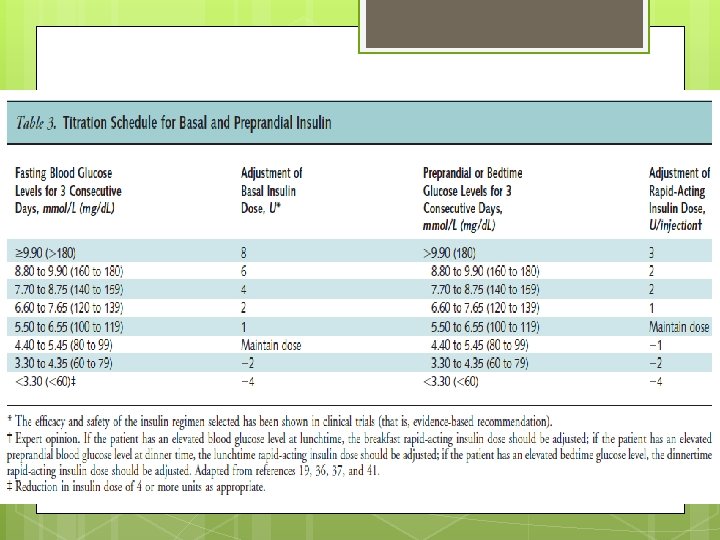
AACE Titration of Basal Insulin is based on fasting blood glucose levels, 4 U added for FPG > 180 mg/dl, - 2 U added of 140 < FPG < 180 mg/dl, - with and - 1 U added for 110 < FPG < 139 mg/dl.

- Slides: 66