Insulin Therapy Laura ShaneMc Whorter Pharm D BCPS

Insulin. Therapy Laura Shane-Mc. Whorter, Pharm. D, BCPS, BC-ADM, CDE, FASCP, FAADE

What is Diabetes? Disorder characterized by abnormal hyperglycemia due to abnormalities in carbohydrate, protein, fat metabolism Why do we want to control glucose? • To prevent complications

Criteria for Diagnosis: A Review • A 1 c > 6. 5% OR • Fasting plasma glucose (FPG) > 126 mg/d. L† OR • 2 hr PG during Oral Glucose Tolerance Test (75 g OGTT) is > 200 mg/d. L OR • Random PG > 200 mg/d. L plus Sx (3 Ps, wt loss) † Fasting: no caloric intake for at least 8 hours. - In absence of unequivocal hyperglycemia, confirm by repeating criteria 1 -3 - OGTT not for routine use (use for IFG or in GDM) Diabetes Care 2017; 40(Suppl 1): S 13
 • A 1 c is primary target for glycemic goal")
ADA Glycemic Goals: (2017) • A 1 c is primary target for glycemic goal • Goal is < 7% for most adults; <7. 5% for children/healthy elderly • Goal is < 8% if intermediate life expectancy, vulnerable; hypoglycemia, fall risk • Goal is < 8. 5% if limited life expectancy • Preprandial – 80 to 130 mg/d. L • Postprandial - < 180 mg/d. L • Goals should be individualized: • Duration of DM • Age/life expectancy • Co-morbidities • Known CVD or advanced microvascular complications • Hypoglycemia unawareness • Individual patient considerations Clinical challenge: What does prandial mean? Diabetes Care 2017; 40(Suppl 1): S 52 -53; S 101

Type 1 or Type 2? • Type 1 • No insulin production • Type 2 • Insulin resistance • Decreased insulin production …Type 3 c? (pancreatogenic issues)

Objectives • State physiologic effects of insulin • List available insulins; describe difference, including OOA, DOA • Distinguish between short acting, rapid acting, and basal insulins • List main adverse effects of insulin • Know place in therapy of different insulins • Design pharmacotherapy regimens for different insulins

Insulin Action at the Cellular Level Bloodstream Insulin Glucose Receptor Cell interior Translocation IRS-1 Substrate-PO 4 Protein synthesis Glycogen, lipid synthesis Mitogenesis Ion transport Glucose transporter GLUT-4 From: www. dmeducate. org Glucose metabolism

Role of Insulin Suppresses • Hepatic glucose production • Lipolysis • Proteolyis • Gluconeogenesis Promotes • Glycogen synthesis • Transport of glucose into adipocytes • Transport of glucose into myocytes

Insulin Secretion • In adults without DM, the pancreas secretes 25 -50 units of insulin/day • Basal insulin secretion 0. 5 -1 units/hour • Additional insulin is secreted when BG > 100 mg/d. L • Insulin is secreted in response to CHO intake (1 Unit/10 -15 gram of CHO) • In humans without DM, BG: 40 -160 mg/d. L • BG> 40 mg/d. L needed for normal brain function
 • Suppresses glucose production between meals")
The Basal/Bolus Insulin Concept Basal Insulin (Background insulin) • Suppresses glucose production between meals and overnight • Nearly constant levels • Supplies 50% of daily needs Bolus Insulin (Mealtime or Prandial) • Limits hyperglycemia after meals • Immediate rise and sharp peak at 1 hour • 10% to 20% of total daily insulin requirement at each meal 6 -
 Basal Insulin (~0. 5 -1. 0 U/hr)")
NORMAL PANCREAS “Bolus” Insulin Effect (Meal Associated) Basal Insulin (~0. 5 -1. 0 U/hr) Breakfast Lunch Supper Insulin is released in response to varying blood glucose levels and hypoglycemia does not occur
 Insulins • Short-Acting • Rapid-Acting Basal Insulin")
Types of Insulin Bolus or Prandial (Mealtime) Insulins • Short-Acting • Rapid-Acting Basal Insulin • Slow-acting Mixes • Mixtures of short or rapid-acting and longer-acting insulins Concentrated insulin • Humulin R 500 insulin
")
Short and Rapid-Acting Insulins Insulin Short-Acting Regular Humulin/Novolin R Rapid-Acting Lispro (Humalog U-100; U-200) Aspart (Novolog or Fiasp) Glulisine (Apidra) Technosphere Insulin Afrezza Onset Peak Max Duration 30 -60 min 2 -3 hours 6 -8 hours 5 -15 min; Fiasp: 2. 5 min ~12 min (measured effect) 1 -2 hours 4 -6 hours 35 -45 min ~ 1 ½ to 3 hours
 2 -4 hours 4 -6")
Basal Insulins Insulin Onset Peak Max Duration NPH (Intermediate) 2 -4 hours 4 -6 hours 14 -18 hours Detemir (Levemir) 2 hours 6 -8 hours Flat? 0. 2 Units/kg 12 hours 0. 4 Units/kg 20 hours 2 -4 hours Flat 20 -24 hours Basal Glargine Lantus (U-100) Basaglar (U-100) Toujeo (U-300) Degludec (Tresiba) U-100 and U-200 < 36 hours 30 -90 min Flat ~ 42 hours
 Peak Max Duration Humulin 70/30")
Mixed Insulins Insulin Onset Premixed Regular (Regular + NPH) Peak Max Duration Humulin 70/30 Novolin 70/30 30 -60 min 7 -12 hours (Dual) 14 -18 hours Humalog Mix 75/25 Humalog Mix 50/50 (Lispro + Neutral Protamine Lispro) 5 -15 min 7 -12 hours (Dual) 14 -18 hours Novolog Mix 70/30 (Aspart + Aspart Protamine Suspension) 5 -15 min 7 -12 hours (Dual) 14 -18 hours Premixed Rapid

Concentrated Regular Insulin Onset Humulin R U-500 30 min Diabetes Care 2010; 33: 281 -3 Peak Max Duration 3. 5 -8. 5 hours 10 hours; May be up to 24 hours due to delayed absorption of larger doses
 Short (Regular) NPH Long (Detemir)")
Insulins – Peak/Duration Insulin level Rapid (Lispro, Aspart, Glulisine) Short (Regular) NPH Long (Detemir) 0 2 4 6 8 Hours 10 12 14 16 Hours after injection 18 Long (Toujeo) (Degludec) Long (Glargine) 20 22 24 26 30 36 40 42

Insulin Review • Which insulin types are short-acting? Another name for prandial insulin? • Which insulins are rapid-acting? Are they prandial? • Which insulin is intermediate-acting? • Which insulins are long-acting? What is another name for long-acting insulin? • Patients MUST be taught to eat at regularly scheduled times!!!

How Long to Leave at Room Temperature? Insulin Type Glargine Duration U 100 – 28 days U 300 – 42 days Detemir U 100 – 42 days Degludec Pens (single insulin) Pens (mixed insulin) Inhaled U 100 and U 200 – 56 days U 100 and U 200 – 28 days U 100 – 10 to 14 days 10 days
 § U 50 (50 Units)")
Delivery Devices • Syringes § U 30 (30 Units) § U 50 (50 Units) § U 100 (100 Units)

Delivery Devices • Pens § Manufacturer specific

Delivery Devices • Continuous Subcutaneous Insulin Infusion § e. g. , an “insulin pump”

Insulin Pumps May provide insulin at a slow, continuous rate • Pts receive a small stream of bolus insulin over 24 hours • Simulates post-absorptive insulin secretion • In boluses, mimics normal insulin peaks released after a meal Good candidate: person requiring large insulin doses Pumps “approximate” physiologic insulin • Emerging: negative feedback component to automatically measure BG and adjust insulin dose § May be matched with continuous glucose monitors to create a “closed loop system” (artificial pancreas)

Insulin Pumps – Spring 2017 “Artificial Pancreas” Medtronic Mini. Med 670 G System • “Closed-loop insulin delivery system for 14 y/o + with T 1 DM • Still requires separate insertions for pump and sensor • Sensor measures interstitial glucose q 5 min and uses 3 levels of automation: § Suspend before low - suspends insulin delivery if glucose approaching a “preset” low value and resumes when BG begins to rise § Suspend on low - suspends insulin delivery for up to 2 hours when sensor reaches a “preset” low value § Auto mode - automatically adjusts insulin doses throughout the day to a standard target BG of 120 mg/d. L or a temporary value of 150 mg/d. L (such as for exercise) • Users will still have to input grams of CHOs and accept recommended “bolus” doses • Includes: Mini. Med 670 G insulin pump, Guardian Link transmitter, Guardian Sensor, One. Press Serter, Contour NEXT Link 2. 4 glucose meter http: //www. medtronicdiabetes. com; http: //www. fda. gov/Medical. Devices/Productsand. Medical. Procedures/Device. Approvalsand. Clearances/Recently. Approved. Devices/ucm 522764. htm
 • Mild, clinically")
Insulin ADRs Hypoglycemia ( < 70 mg/d. L, + symptoms; ) • Mild, clinically significant (< 54 mg/d. L); severe (need others’ help) • Must do self monitoring of blood glucose (SMBG) • Treatment – 15 gm of glucose; Glucagon if unconscious • If it’s still low after 15 min, administer 15 gm more: § ½ cup orange juice or milk or NON-DIET soda § 5 -6 Lifesavers § Glucose tablets (each one has 4 -5 gm CHO) § Small box of raisins Once BG returns to normal, pt should eat meal/snack to prevent hypoglycemic recurrence Weight Gain – Another Adverse Effect

Defective Counterregulation After 2 -5 years of having type 1 DM, deficiency in glucagon secretion Therefore, there must be an appropriate response to epinephrine After more time (8 -15 years), defective epinephrine secretion also occurs Hypoglycemia must be treated with glucagon injections NOT CANDIDATES FOR INTENSIVE INSULIN THERAPY!!

Insulin Adverse Effects • Dermatologic § Lipohypertrophy § Skin thickening; repeatedly injecting same site § Management: “skin checks; ” insure site rotation § Lipoatrophy § Injection site pitting; immune system dysfunction § Management: “skin checks; ” insure site rotation § Local skin reactions § Redness, swelling: § Management: “skin checks; ” check appropriate injection technique
 • Short-acting (OOA is")
Insulin Types - Older Regular (Humulin R or Novolin R) • Short-acting (OOA is 30 min; inject then MUST EAT in 30 min) NPH (Humulin N or Novolin N) • Intermediate-acting • Affects BG ~ 2 meals after injection § e. g. , don’t have to eat right away but don’t delay/skip meals • Morning NPH will be reflected in 5: 00 pm reading Mixtures (Regular/NPH) • 70/30 (70% NPH; 30% Regular) for Humulin/Novolin

The Bioengineered Insulins
 – FYI Lysine exchanged with proline Thr Lys B 30 Pro")
® Humalog (Lispro) – FYI Lysine exchanged with proline Thr Lys B 30 Pro Thr A 1 Phe Tyr Phe Gly Arg Glu Gly B 20 Cys B 28 Asn A 21 B 29 Cys Gly Val Tyr Le u Tyr Asn Ile Glu Val Leu Gln Gln Cys Leu Ala Glu Tyr Cys Thr Ser Ile Cys Ser Val Leu His Ser B 1 Phe Val Asn Gln His Leu Cys Gly

Humalog – An Example of Amino Acid Changes in the Insulin Molecule Changes in the insulin molecule • B-28 lysine • B-29 proline Result of changes in molecular structure • Hexamer dissociates quickly into dimers and monomers • Rapid absorption occurs
, Aspart (Novolog®), Glulisine (Apidra®) Through amino acid changes, the pharmacokinetics is affected:")
Lispro (Humalog®), Aspart (Novolog®), Glulisine (Apidra®) Through amino acid changes, the pharmacokinetics is affected: • Bolus effect – onset in 5 -15 minutes • Peak effect within 1 to 2 hours • Duration of action is 4 -6 hours Availability • Vials, pens
, Aspart (Novolog®), Glulisine (Apidra®) Place in therapy • Alternative to Regular •")
Lispro (Humalog®), Aspart (Novolog®), Glulisine (Apidra®) Place in therapy • Alternative to Regular • Inject immediately before (or even right after a meal) • Improved PPG • Convenience • Used in insulin pumps • May mix with NPH in the same syringe Combinations? • Yes – Humalog Mix 75/25; Novolog Mix 70/30 § Mix of basal plus bolus • No - glulisine

Basal Insulins NPH Glargine Detemir Degludec

Intermediate-Acting Insulin: NPH Slower release of insulin Onset of action – 2 to 4 hours Peak – 4 to 6 hours Duration of action – 14 to 18 hours Must inject twice/day • e. g. basal dose must be divided in half and injected twice/day May be used in Type 1 and Type 2 DM (insulin-requiring)
 Molecular structure is changed to allow")
Long-Acting Insulin: Glargine (Lantus , Basaglar , Toujeo®) Molecular structure is changed to allow for slow release of insulin When injected, a precipitate forms Insulin releases slowly

Glargine: Changes in Molecular Structure Clear Solution p. H 4 p. H 7. 4 Dissolution Hexamers 10 -3 M Change in isoelectric point so it is an acidic solution (p. H 4. 0) Precipitati on Dimers 10 -5 M Monomers 10 -8 M Capillary Membrane Insulin in Blood Adapted from: Kramer W. Exp Clin Endocrinol Diabetes 107(1999) Suppl 2 Precipitation of Glargine in subcutaneous tissue (p. H 7. 4) Slow dissolution of free Glargine hexamers from precipitated Glargine (stabilized aggregates) Insulin releases slowly; Protracted action

Glargine: Pharmacokinetics • • Onset of action – 2 to 4 hours U-100 Duration ~ 20 -24 hours U-300 Duration ~ 36 hours “Peakless” profile
 insulin used in")
Glargine Type 1 DM: • Glargine used once/day and bolus (mealtime) insulin used in Type 1 DM • NOT mixed in the same syringe; separate injections Type 2 DM: • Glargine used once/day and pt continues oral DM meds • Can eventually inject both glargine and bolus (mealtime) insulin (may stay on some oral meds) • NOT mixed in the same syringe; separate injections
 6 5 Glargine - Place in Therapy:")
Glargine vs NPH Glucose Utilization Rate (mg/kg/h) 6 5 Glargine - Place in Therapy: 4 • Less weight gain and hypoglycemia than with NPH • Bridge to exclusive insulin treatment in pts with type 2 DM 3 • Different pharmacokinetics; equivalent to NPH for A 1 c lowering 2 Glargine 1 0 0 10 20 Time (h) After SC Injection 30 End of observation period Lepore, et al. Diabetes. 1999; 48(suppl 1): A 97.

Glargine at HS + Short Acting Insulin Effect Short acting Glargine B L S HS B 6 -
 • Molecular structure is changed to allow for slow release")
Detemir ® (Levemir ) • Molecular structure is changed to allow for slow release of insulin • Binds to albumin • Insulin releases slowly Onset of action: 2 hours Peak: 6 -8 hours Duration: dose dependent • 12 hours for lower doses (0. 2 Units/kg/day) • ~ 20 hours for higher doses (0. 4 Units/kg/day) Dose once or twice daily

Detemir Used with shorter acting insulins • Bolus insulins injected with meals • Detemir once or twice/day • Start at same dose as other basals (May have to adjust) Cannot mix detemir with other insulins in same syringe In Type 2 DM, may add to regimen of oral agents Place in therapy? Same as glargine or NPH Stings less than glargine; less glycemic variability; less weight gain
 • Molecule changed to allow for slow release • Multihexamer")
Long-Acting Insulin: Degludec (Tresiba®) • Molecule changed to allow for slow release • Multihexamer • Insulin releases slowly – t ½: 25 hours; DOA: 42 hours • U 100 (1 Unit increments) and U 200 (2 Unit increments) Place in therapy? U-100 has less hypoglycemia than U-100 glargine
 Duration of action • 42 hours; detectable up to 96")
Degludec ® (Tresiba ) Duration of action • 42 hours; detectable up to 96 hours • May be dosed at variable times during day Available by itself/will be combined with aspart (70/30; Ryzodeg®) Compared to glargine? • No difference in A 1 C • No benefit to PPG • Lower FPG Hypoglycemia? • Less overall than glargine • Less nocturnal hypoglycemia

What if a Person is Injecting Hundreds of Units of Insulin Daily?

What About Large Insulin Doses? If pt is on really large doses of insulin? (e. g. , > 200 -300 Units/day) • Humulin R U-500 (20 m. L vials; ~ $210/vial) • Not usually stocked in pharmacies (allow 24 -72 hrs) Consider that insulin syringes go up to 100 Units (1 m. L) Max amount injected at one site: 2. 5 m. L • Have to use 2 ½ syringes of 1 m. L size • U-500 special syringe (11 -2016) § Only by prescription

Humulin R U-500 - 5 x more concentrated than U-100 • More like NPH than Regular • Onset of effect within 30 min • Peak 3. 5– 8. 5 hrs • Duration usually > 10 hours but may be up to 24 hrs due to delayed absorption of larger dose Disadvantages • Hypoglycemia 18 -24 hrs after injection • Requires careful prescription writing, EDUCATION, labeling • If using vials and traditional syringes: § Tuberculin syringes (state volume but may be an approximation; 0. 1 m. L=50 Units) § U-100 syringe in “Marks” (1 mark=5 Units) Diabetes Care 2010; 33: 281 -3

Converting U-100 to U-500 Insulin If A 1 c < 8% or FPG < 183 mg/d. L in previous 7 days, start at 80% of total daily U 100 insulin dose If A 1 c > 8%, start at 100% of total daily dose Dose 2 -3 daily doses • No less than 4 -6 hrs apart Dose 30 min before meals Regimen 2 doses 60%, 40% (Pre-breakfast, pre-dinner) 3 doses 40%, 30% Pre-breakfast, pre-lunch, pre-dinner ENDOCR PRACT 2015; 21: 782 -93

Humulin R U-500 – When to Consider? • When daily dose exceeds 200 Units/day • Multiple injections are required to deliver a single dose • Adherence issues due to several daily injections • Severe insulin resistance (associated with morbid obesity/physical inactivity) • Patients on high dose glucocorticoids

Afrezza®: Technosphere Insulin Human insulin electrostatically linked to a proprietary Technosphere particle Insulin Type: Ultra-Rapid Acting Insulin (e. g. , a prandial insulin) Indication: Type 1 (+ long-acting insulin) or Type 2 Diabetes Time to measurable effect: 12 min Time to peak effect: 35 -45 min Duration ≈ 90 -180 minutes T 1/2 = 28 -39 minutes
 • Frequent")
Afrezza®: Technosphere Insulin Contraindicated • Chronic lung disease (Asthma, COPD, etc. ) • Frequent episodes of hypoglycemia • Hypersensitivity to human insulin or Afrezza excipients ADRs Cough • Hypoglycemia • Throat Irritation/Pain • Bronchial Spasm (REMS) •

Monitoring Insulin Effects • Most significant side effect is hypoglycemia • Counsel patients not to delay/skip meals § If alcohol is consumed, drink slowly/eat carbs • Instruct patients to use a BG meter • Ideally test BG to look at patterns • Check FPG • Check before meals and/or PPG § Especially after largest meal and hs • In Type 1 DM, check BG at 3: 00 am

Insulin Dosing Regimens

Insulin Dosing Regimens “Bolus” Basal Type 1 At diagnosis: 0. 3 to. 5 U/kg /day • Half is basal • Half is bolus (prandial) “Honeymoon” 0. 2 to 0. 5 U/kg • Stay on half basal + half prandial

Insulin Dosing Regimens No one correct way in Type 2 • Initially add basal insulin to oral meds – start at 10 U/day • Eventually will dose and will possibly add prandial insulin • Dose adjusted according to SMBG • May eventually require very large doses of basal/bolus • 2 to 2. 5 Units/kg/day or more

Case Question NT weighs 72 kg. If the starting dose is 0. 5 Units/kg and half the dose should be basal and half the dose should be bolus then: Which of the following is the most appropriate starting dose of insulin? a. b. c. d. 72 Units of insulin – 36 Units of NPH once/day and 36 Units of Regular once/day 72 Units of insulin – 36 Units of NPH twice a day 36 Units of insulin – 36 Units of NPH once a day 36 Units of insulin – 9 Units of NPH twice/day and 6 Units of Regular 3 times/day
 Starting or adjusting a regimen")
Insulin Administration Times Different strategies (according to individual’s needs/habits) Starting or adjusting a regimen • Twice/day dosing (am/pm: breakfast/dinner) • 3 times/day dosing (am, pm, hs) • 3 times/day dosing (am, noon, pm) • 4 times/day dosing (mealtime, hs) § Detemir, glargine, degludec at bedtime • 5 times/day dosing (prandial 3 times/day; basal 2 times/day) Ann Intern Med 2006; 145: 125 -34; Postgrad Med J 2016; 92: 152 -64

J. P. HPI: JP is a 28 y/o female, referred to DM Clinic by STH b/c a routine physical revealed glucosuria. Random glucose was 300 mg/d. L. She recently started her DNP program. She has noted polydipsia, nocturia x 5 times/night, fatigue, & 20 lb weight ↓ over a 2 month period (she thought it was the stress of Pharmacology classes). PMH: Recurrent Sinus Infections, 2 Abscessed teeth in last 6 mo. F/H neg for DM; takes no meds. Physical Exam: WNL; Ht 5’ 9” Wt 60 kg; Labs: FPG – 280 mg/d. L; A 1 C – 10% (normal 4 -5. 6%) Urine glucose – positive; trace ketones

J. P. • Question • Findings in history/Physical Exam consistent with type 1 DM? • Question • What medication should be started? • What dose? • How do you know when to adjust the dose?

Insulin Twice A Day Before breakfast/supper May mix 2 insulins Or, use a pre-mixed insulin • Humulin or Novolin 70/30 • Humalog Mix 75/25 • Novolog Mix 70/30 Many different ways to dose • One way to start: § 1/2 in morning (breakfast) § 1/2 in evening (supper) +

Dosing Regimen Examples 7: 00 am AC 12: 00 pm AC 6: 00 pm AC 11: 00 pm HS NPH: Reg* *or lispro, aspart, glulisine *or lispro or aspart, glulisine or 70/30 or 75/25 ½ of total daily dose
 7: 00 am AC")
Dosing Example: 60 kg at 0. 5 U/kg (30 Units) 7: 00 am AC 12: 00 pm AC NPH+Reg* * (or rapid-acting) 6: 00 pm AC 11: 00 pm HS NPH+Reg* * (or rapid-acting) Or Pre. Mix Total dose ~ 15 Units

Twice-daily Split-mixed Regimens Insulin Effect Bolus NPH B L S HS B

Insulin Twice a Day Advantage • Easier for person to understand start out initially Disadvantage • No flexibility with meals (remind patient not to delay or skip meals • Potential for NPH to peak at 3: 00 am (if given at supper instead of HS) §This may result in nighttime hypoglycemia (and early morning hyperglycemia) §Glucose control is not as optimal (per the DCCT 1 study) 1 N Engl J Med 1993; 329: 977 -86

Intensive or Conventional Insulin Treatment • Intensive Insulin Treatment - Dosing to mimic the body’s normal insulin release. Thus, requires more than 2 injections/day. Uses insulin with different action profiles. • Conventional Insulin Treatment – 1 to 2 injections/day using intermediate-acting or long-acting insulin. • Goal: to achieve near normal glucose values

Intensive Insulin Treatment • Candidates for Intensive Insulin Treatment § Highly-motivated, adherent patients (must be willing to check glucose several times daily) § Patients who have a longer expected life span (intent is to reduce complications) § Pregnant or planning to conceive (with DM) § Poorly controlled and wanting to improve control

Intensive Insulin Treatment • Who are not candidates? § Hypoglycemic unawareness § Older individuals § Young children § CAD or cerebral vascular disease § Severe DM complications

Insulin 3 Times a Day Before breakfast Before supper At bedtime Can mix 2 insulins (one basal; one bolus) for one of the doses (am) Or, pre-mixed insulin (for am dose) Rest of dose given in the evening • Short acting (bolus) with supper • Basal at bedtime

Dosing Regimen Examples – 3 Shot Regimen 7: 00 am AC 12: 00 pm 6: 00 pm AC AC 11: 00 pm HS NPH+Reg* NPH ½ of TDD** ¼ of TDD *May use lispro or aspart or glulisine instead of Regular ** TDD = Total Daily Dose
 7: 00 am AC")
Dosing Example: 60 kg at 0. 5 U/kg (30 Units) 7: 00 am AC 12: 00 pm 6: 00 pm AC AC 11: 00 pm HS NPH+Reg* NPH ½ of TDD** (10 U NPH 5 U Reg) ¼ of TDD 7 -8 U Reg 7 -8 U NPH * May use lispro or aspart instead of Regular ** TDD = Total Daily Dose
 3 Shot Regimen Insulin Effect Regular NPH B L S")
Multiple Daily Injections (MDI) 3 Shot Regimen Insulin Effect Regular NPH B L S HS B NPH + Bolus AC AM Bolus AC QPM NPH HS

What About…. ?

Inject 3 Times/Day Must Mix 2 Times/Day 7: 00 am AC 12: 00 pm 6: 00 pm 11: 00 pm AC AC HS NPH: Reg* *May use lispro or aspart or glulisine instead of Regular
 Insulin Effect Regular NPH B L")
NPH + Regular (3 -Shot Regimen, Mix Twice) Insulin Effect Regular NPH B L S HS B NPH/Bolus at breakfast Bolus Before Lunch NPH/Bolus at supper

Insulin 3 Times/Day Advantage • A bit more physiologic than twice/day • Lower A 1 C (per DCCT 1) • If injecting last dose of NPH at night then that avoids middle of the night hypoglycemia Disadvantage • Morning NPH decreases mealtime flexibility • Must monitor BG qid (meals/hs) • If injecting last dose of NPH with supper may experience middle of the night hypoglycemia (from the NPH peaking) 1 N Engl J Med 1993; 329: 977 -86
 What is the Difference? Regular at")
Regular vs. Rapid-Acting Insulin (3 -Shot Regimen Profile) What is the Difference? Regular at Breakfast Regular at Lunch Regular at Supper Rapid-Acting Regular Insulin Effect Rapid at Breakfast Rapid at Lunch Rapid at Supper B L S Stacking HS B B L S HS

Insulin 4 Times/Day Advantage • More physiologic • Lower A 1 C (per DCCT 1) Disadvantage? • 4 injections • Should monitor BG qid 1 N Engl J Med 1993; 329: 977 -86
 • Bedtime (basal); could")
Insulin 4 Times/Day: Glargine HS • Breakfast, Lunch, Supper (bolus) • Bedtime (basal); could be anytime (but consistent) • ½ total daily dose is glargine (dosed once/day) • Other ½ of total daily dose is prandial, divided among the 3 meals • 1/6 prandial at breakfast • 1/6 prandial at lunch • 1/6 prandial at supper

Dosing • What if a patient weighs 60 kg and you will be prescribing basal (glargine or degludec) and bolus (prandial) insulin. • Using a starting dose of 0. 5 Units/kg, how many units will be basal and how many units will be bolus (prandial)?

Dosing Example: 60 kg at 0. 5 Units/kg Answer 30 Units/day Total Daily Dose 7: 00 am AC 12: 00 pm AC 6: 00 pm AC 11: 00 pm HS Reg (1/6) Glargine (1/2) Lispro Glargine (1/2) Aspart Glargine (1/2) 5 Units 15 Units

Glargine/Degludec at HS + Short Acting Insulin Effect Short acting Glargine or Degludec B L S HS B
 Needs to be Split: 5 Injections/Day Why? • Huge doses")
Sometimes… Glargine (or Degludec) Needs to be Split: 5 Injections/Day Why? • Huge doses of basal Split the dose • Use ½ total daily dose of glargine (am and hs) • Other ½ of total daily dose is split up among number of meals/day (usually 3) • Disadvantage? 5 injections/day

Remember: if Basal is Detemir or NPH Split the dose • Use ½ total daily dose qam/qpm • Equal doses first, then individualize • Disadvantage? 5 injections/day Some individuals may be able to use detemir once/day

Dose Adjustments • A common starting dose is 0. 5 Units/kg/day • If all BG values are elevated (>200 mg/d. L), increase daily dose by ~ 0. 1 Unit/kg/day • For instance, if current daily dose is 0. 5 Units/kg but all BG values are elevated, increase daily dose to 0. 6 Units/kg

For Example: Adjusting Doses Pt weighs 60 kg and TDD is 0. 5 U/kg/day (30 Units). BG values: 7: 00 am 12: 00 pm 5: 00 pm 11: 00 pm 3: 00 am 260 mg/d. L 240 mg/d. L 290 mg/d. L 250 mg/d. L 230 mg/d. L How should regimen be changed? a. b. c. d. Increase total daily dose by 0. 1 U/kg (0. 6 U/kg=36 Units/day) Increase today daily dose by 0. 3 U/kg (0. 8 U/kg=40 Units/day) Increase today daily dose by 0. 5 U/kg (1 U/kg=50 Units/day) Increase today daily dose by 1 U/kg (1. 5 U/kg=75 Units/day)

If all BG values are not elevated: Adjust one insulin dose at a time START WITH THE INSULIN DOSE AFFECTING THE HIGHEST BLOOD GLUCOSE OF THE DAY

BG Patterns Pt is on lispro/NPH at breakfast/dinner. BG values: Fasting Before lunch Before dinner 90 201 78 97 185 99 101 230 80 92 205 82 Which is most appropriate action? a. b. c. d. morning NPH morning lispro Bedtime 110 108 120 123

BG Patterns Pt is on lispro/NPH at breakfast/dinner. BG values: Fasting Before lunch Before dinner 90 120 48 97 135 49 101 130 50 92 145 57 Which is most appropriate action? a. b. c. d. morning NPH morning lispro Bedtime 110 108 120 123

BG Patterns Pt is on lispro at breakfast/lunch/dinner and glargine at bedtime. Fasting Before lunch Before dinner 90 120 130 97 135 125 101 130 115 92 145 112 Which is most appropriate action? a. b. c. d. morning lispro lunchtime lispro evening lispro bedtime glargine Bedtime 210 218 215 223

BG Patterns Pt is on lispro at breakfast/lunch/dinner and glargine at bedtime. Fasting 60 50 52 48 Before lunch 135 130 145 128 Before dinner 125 112 126 Which is most appropriate action? a. b. c. d. morning lispro lunchtime lispro evening lispro bedtime glargine Bedtime 160 155 163 148

Dose Adjustments - Summary If all glucose values are elevated (e. g. , > 200 mg/d. L), increase total dose a small amount (0. 1 U/kg) • Or… 1 -2 Units/dose Look for glucose patterns If all values are not elevated, adjust one time of insulin dose • Start out with dose affecting highest BG • Or…some clinicians believe: “fix the fasting first”

GW GW Pt is on lispro at breakfast/lunch/dinner and glargine at bedtime. He has the following BG values (mg/d. L): Fasting 203 181 210 300 Before lunch 135 130 145 128 Before dinner 125 112 126 Bedtime 160 155 163 148 Which abnormal value should be corrected first? What med change can correct the abnormal value?

J. P. JP is a slender 22 y/o female newly diagnosed with Type 1 DM. She is 5’ 9” and weighs 60 kg. She is to start insulin. Using a starting dose of 0. 5 U/kg, list the appropriate doses/draw appropriate graphs for 4 different methods of administering insulin, using the following regimens: 2 -injections of a pre-mixed insulin (dose, regimen, when to administer, insulin graph) 3 -injection regimen where pt has to mix insulins for one of the doses (or use a pre-mix for one dose) 3 -injection regimen where pt has to mix insulins for two doses 4 -shot regimen

FYI: Insulin Curves Twice-daily Split-mixed Regimens Insulin Effect Regular NPH B L S HS B
 3 Shot Regimen Insulin Effect Regular NPH")
FYI: Insulin Curves Multiple Daily Injections (MDI) 3 Shot Regimen Insulin Effect Regular NPH B L S HS B NPH + Bolus AC AM – has to mix (or used a pre-mix) Bolus AC (only) before supper NPH (only) HS

FYI: Insulin Curves NPH + Regular (3 -Shot Regimen, Mix Twice or Pre-Mix Twice and Prandial Only at Lunchtime) Insulin Effect Regular NPH B L S HS B NPH/Bolus at breakfast Bolus Before Lunch NPH/Bolus at supper
 HS + Short Acting Glargine (Lantus) for Basal")
FYI: Insulin Curves Glargine (or Degludec) HS + Short Acting Glargine (Lantus) for Basal coverage Could use Detemir (Levemir) or NPH for Basal coverage (but may need to dose bid) Insulin Effect Short acting Glargine or Degludec B L S HS B

Summary: Ways to Dose/Adjust Doses for Basic Insulin Dose? Adjust doses if pattern is observed under stable diet/exercise circumstances Adjust basic dose moving towards ideal goal slowly Unless all values > 200 mg/d. L, adjust one time of day dose at a time

Starting Glargine in Type 2 DM FY is a 66 year old male who has an A 1 C of 9. 1%. He is currently on oral DM meds (metformin 1000 mg twice daily and glipizide 20 mg daily). You think he would benefit from losing weight, being more physically active, and starting insulin. How would you start insulin? Type 2 on oral agents • 10 U SQ hs or • 0. 1 Units/kg hs or • 0. 2 Units/kg hs • Increase the dose every few days

Dose Adjustment for Basal Insulin in Type 2 DM IF adjusting single-dose evening (or bedtime) insulin (in Type 2 DM patients who are still on oral DM meds) increase dose according to following regimen: • Can follow different algorithms 1 Or, can increase dose by 2 Units every 3 days until reach a designated point (120, 130? ) Or, can increase dose by 1 Unit every night until reach a designated point (120, 130? ) 1 Diabetes Obes Metab 2014; 16: 193 -205

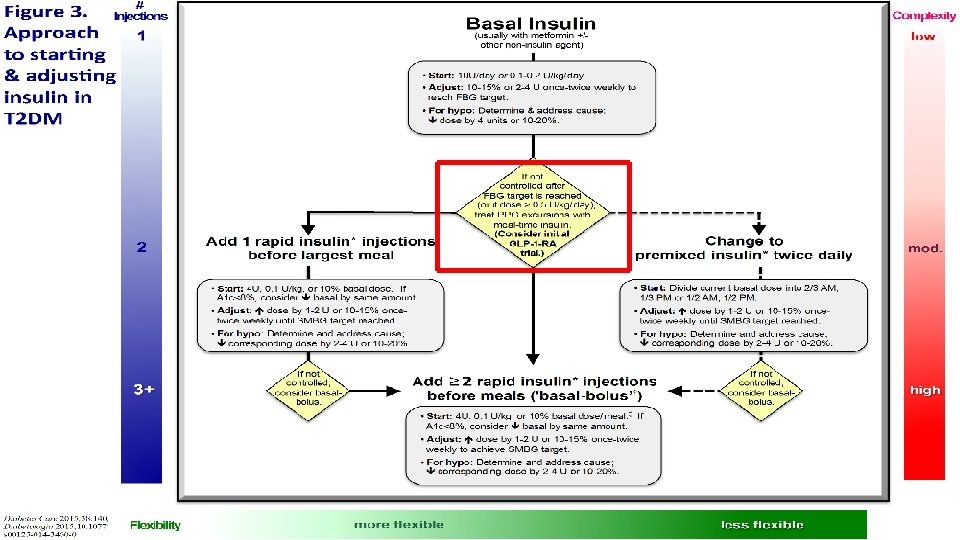
Starting Insulin in Type 2 Diabetes © 2017 by American Diabetes Association Dia Care 2017; 40: S 64 -S 74

Shared Decision Making: When to Add Prandial to Basal Insulin in T 2 DM WD is a 42 year old white female that is on metformin, glipizide, and glargine insulin 40 Units at bedtime. She weighs 132 lb. • How many Kg does she weigh? • How many units/kg is she injecting? • Would you add prandial insulin? • What other information is needed? § Hint: Fasting glucose? A 1 C?

Prandial Insulin in Type 2 DM? Once the basal insulin dose is > 0. 5 U/kg, consider adding prandial insulin • Happens when ~ 40 -60 Units/day of basal Adding prandial insulin – several ways • Add 4 to 5 Units of prandial to largest meal of the day (continue most oral DM meds) • Or add 0. 1 Unit/kg Or 10% of basal dose to largest meal • Eventually add 4 to 5 Units of prandial insulin to other meals § Must work with the patient to see if willing to inject 3 doses of prandial along with basal

Prandial Insulin in Type 2 DM? Or, switch from Basal to Pre-Mix Take total basal dose and divide as the pre-mix (~ 1/2 in morning and 1/2 in evening) • Can be cautious and start ~ 80% of total dose: § Example: If injecting 40 Units of glargine and switching to pre-mix, 80% is 32 Units • 16 Units before/right after breakfast • 16 Units before/right after supper New development: New algorithm states advancing to 3 pre-mix insulin injections if twice/day of pre-mix does not control A 1 C *NOTE: When adding prandial insulin: D/C the secretagogue (e. g. , SU or glinide)

Prandial Insulin in Type 2 DM? Or go directly to Basal/Bolus ½ of the total daily dose will be basal ½ of the total daily dose will be bolus • Split up among the major meals *REMEMBER: When adding prandial insulin, D/C the secretagogue (e. g. , SU or glinide)

Sick Day Management Don’t stop insulin and test BG q 2 -4 hours Drink plenty of fluids (1 cup/hour) Supplemental doses of Regular (1 -2 U for every 30 -50 mg/d. L > 250 mg/d. L) If BG > 240 mg/d. L, test urine for ketones (T 1 DM) • Call provider for BG > 300 mg/d. L + positive ketones or difficulty breathing (RR > 24/min) or nausea, vomiting, or diarrhea, etc. Type 2 DM – > 400 mg/d. L (a suggestion) • If on insulin, administer 2 -3 extra units of fast-acting insulin and check BG 4 x/day • If BG does not go down or if BG > 500 mg/d. L, go to ER • If not on insulin, go to clinic; if clinic closed, re-check glucose and if > 450 to 500 mg/d. L, go to ER

Immediate Clinic/Hospital Treatment • Glucose has remained high in spite of extra insulin • Persistent vomiting/inability to tolerate fluids by mouth • Persistent diarrhea and progressive weakness • Orthostasis • Difficulty breathing, rapid/labored respirations • Change in mental status

Different Scenario: What If? Pt is using 14 U NPH/7 U lispro before breakfast, 7 U lispro at Lunch, 7 U lispro 20 U NPH before dinner. BG patterns are now: 7: 00 am 260 mg/d. L 12: 00 pm 130 mg/d. L 5: 00 pm 110 mg/d. L 11: 00 pm 90 -120 mg/d. L 3: 00 am 40 -60 mg/d. L Why does the patient have fasting hyperglycemia?

Different Scenario: What If? Pt is using 14 U NPH/7 U lispro before breakfast, 7 U lispro at Lunch, 7 U lispro 20 U NPH before dinner. BG patterns are now: 7: 00 am 260 mg/d. L 12: 00 pm 130 mg/d. L 5: 00 pm 110 mg/d. L 11: 00 pm 90 -120 mg/d. L 3: 00 am 40 -60 mg/d. L Why does the patient have fasting hyperglycemia? a. Evening NPH dose may not be sufficient? b. Excessive bedtime snack? c. Somogyi reaction? d. Dawn phenomenon?

Somogyi Phenomenon Very low blood glucose at 3: 00 am Rebound fasting hyperglycemia • glucose production from cortisol, epinephrine, GH Symptoms – night terrors, night sweats, restless sleep, morning HA Treatment – move pm dose of NPH to hs and add a bedtime snack

Dawn Phenomenon Increased BG between 4: 00 and 8: 00 am Follows a physiologic drop in BG between midnight and 3: 00 am Low in the night is not as low as for Somogyi Occurs due to early morning production of cortisol and GH Occurs inconsistently from day to day Treatment – increase evening NPH dose

Distinguishing Somogyi from Dawn Pt is using 14 U NPH/7 U lispro before breakfast, 7 U lispro at Lunch, 7 U lispro/20 U NPH before dinner. BG patterns: 7: 00 am 12: 00 pm 5: 00 pm 11: 00 pm IF: 3: 00 am 260 mg/d. L 130 mg/d. L 110 mg/d. L 90 -120 mg/d. L 40 -60 mg/d. L (Somogyi)…. Tx? 70 -100 mg/d. L (Dawn)…. Tx?

Insulin Correction Doses Divide 1800 by total amount of insulin to determine how much 1 Unit of insulin will lower BG • If on 50 Units/day of insulin: 1800/50 = 36 • So 1 Unit of insulin will lower BG by 36 mg/d. L Decide on a target glucose • Say, a target glucose is 140 mg/d. L and current reading is 210 mg/d. L • 2 Units may be given and that will lower BG by ~ 72 mg/d. L • Should achieve BG of ~138 mg/d. L Not exact, but pretty close

Correction Doses for CHOs Divide 500 by total amount of daily insulin to determine how many CHOs 1 Unit of prandial insulin is needed to eat those extra CHOs • If on 50 Units/day of insulin: 500/50 = 10 CHOs • So 1 Unit of insulin will cover 10 g of CHOs A patient wants to eat a whole baked potato at dinner (that contains ~ 60 gm of CHOs) • Will need 6 extra Units of prandial insulin at that meal A patient wants to eat an extra-rich brownie for dessert (that contains ~ 30 gm of CHOs) • Will need 3 extra Units of prandial insulin at that meal Not exact, but pretty close

Example: Correction Doses for CHOs A patient is injecting 26 Units of glargine at bedtime and 8 Units of lispro three times/day with breakfast/lunch/supper. The patient’s glucose before supper is 200 mg/d. L. They also want to eat a whole baked potato. How much insulin should they inject with supper? 1. Will still inject 8 Units of lispro (prandial) 2. Pre-meal Correction dose: At 200 mg/d. L – want to be at 140 mg/d. L; need to decrease glucose by 60 mg/d. L. • So the correction dose would be 1800/50 = 36; so approximately 2 Units of prandial insulin would have to be injected. 3. Meal correction dose: Patient wants to eat a whole baked potato at dinner (has ~ 60 gm of CHOs) • Will need 500/50 or 1 Unit will cover 10 Grams of CHO • 6 extra Units of prandial insulin at that meal

Example: Correction Doses for CHOs Total pre-meal dose of lispro would be: • 8 Units that they normally inject • + 2 Units (correction for BG of 200 mg/d. L) • + 6 Units to cover the baked potato Total supper dose would be 16 Units Not exact, but pretty close

Must Evaluate Glucose Patterns If on > 2 insulin doses/day, observe SMBG patterns and think about insulin curves Observe SMBG patterns (the following will work only if pts are willing to check pre/post meal BG) A general example of how to do correction doses: • If pre-meal BG < 70 mg/d. L, dose of prior meal Regular (or lispro or aspart or glulisine) by 1 -2 Units • If pre-meal BG > 150 mg/d. L, dose of prior meal Regular (or lispro or aspart or glulisine) by 1 -2 units • If supplemental doses are or for > 3 days, adjust the dose to reflect the actual doses being used

Selected Insulin Drug Interactions Drug Effect Mechanism Glucocorticoids �Blood glucose Impair insulin action Atypical Antipsychotics �Blood glucose Weight gain; �insulin sensitivity Oral Contraceptives �Blood glucose Unclear Protease Inhibitors �Blood glucose �Insulin Resistance; Impair first phase insulin release Diuretics �Blood glucose �Insulin Resistance or �insulin release; May involve K+ change Phenytoin �Blood glucose �Insulin Secretion Sympathomimetics �Blood glucose �Glycogenolysis and Gluconeogenesis ACEIs; ARBs �Blood glucose �Insulin Sensitivity Salicylates (High dose) �Blood glucose Inhibition of different Kinases Alcohol �Blood glucose Inhibits Gluconeogenesis

QUESTIONS?
- Slides: 122