Insulin and Insulin Pumps Dr Waqar Malik Consultant












 Protein glycation b-cell (genetic background) Amyloid deposition Insulin resistance “lipotoxicity” elevated")
, glucagon-like peptide-1 (GLP-1) mimetics")




 5 4 3 2 1 0 0")
 75 Breakfast Lunch Dinner 50 25 4: 00 8: 00 12:")


: A")












 200 CSII (n=93) MDI (n=91) 180 160 140 120 100")

 CSII (n=14) 7. 5 7")
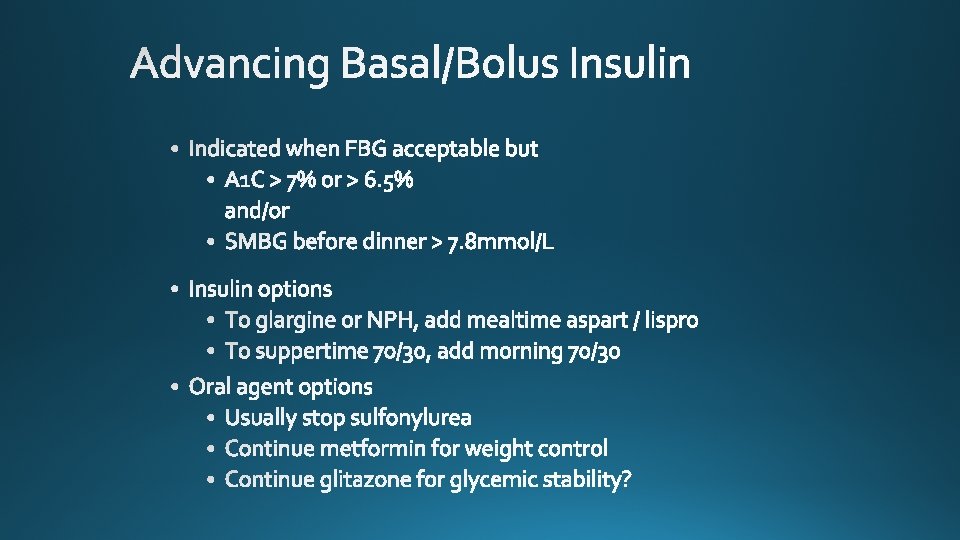
 therapy is recommended as")



- Slides: 62
Insulin and Insulin Pumps Dr Waqar Malik Consultant Diabetologist Blakesley Hall, Blakesley Road, Birmingham 9 th Jan. 2017
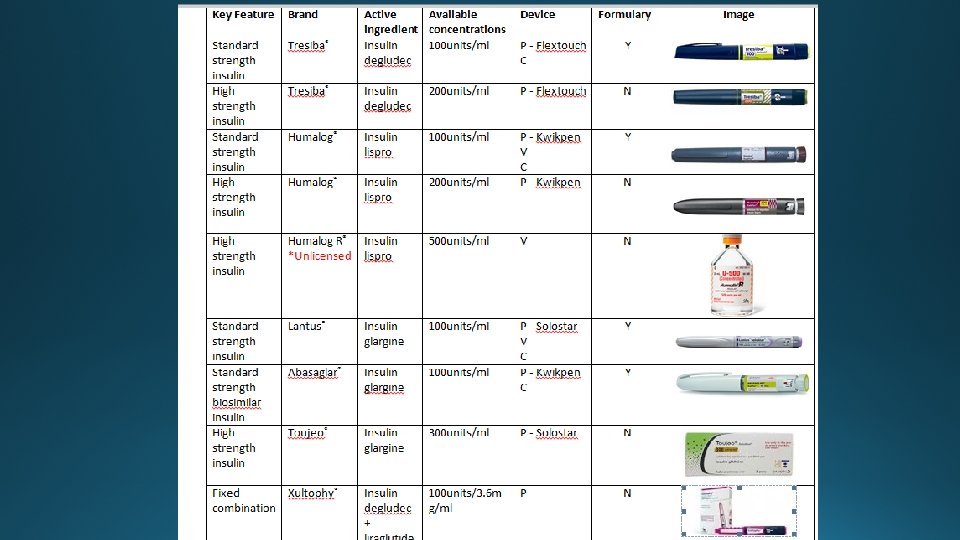
Lay Out • Why glycaemic control is important and what role insulin plays • Different insulins old and new • Some tips about dose titration • Different devices • Continuous subcutaneous insulin infusion (CSII or 'insulin pump')
RELATIVE RISK Mean A 1 C DCCT Research Group, N Engl J Med 1993, 329: 977 -986.
15. 3 years 5. 1 years DCCT Study Group, JAMA 1996, 276: 1409 -1415.
Effect of A 1 C On Complications in the UKPDS Study Stratton IM et al. BMJ 2000; 321: 405 60 50 A 1 C 5. 5% 6. 5% 7. 5% 8. 5% 9. 5% 10. 5% 40 30 20 10 0 Myocardial Infarction Microvasc Disease
Lessons from the DCCT and UKPDS: Sustained Intensification of Therapy is Difficult DCCT (Type 1) UKPDS (Type 2), Insulin Group EDIC 10 8 9. 0 8. 1 7. 9 8 A 1 C (%) 7. 3 A 1 C (%) 7 Baseline 6 Normal 6 4 0 0 6. 5 DCCT +4 + 6 yrs EDIC DCCT/EDIC Research Group. New Engl J Med 2000; 342: 381 -389 Steffes M et al. Diabetes 2001; 50 (suppl 2): A 63 UK Prospective Diabetes Study Group (UKPDS) 33 Lancet 1998; 352: 837 -853 0 2 4 6 8 10 yrs
Mortality of DM Patients Undergoing CABG 16 14 Cardiac-related mortality Noncardiac-related mortality Mortality 12 10 8 6 4 2 0 <150 150 -175 175 -200 200 -225 225 -50 Average Post-operative glucose (mg/dl) Furnary et al J Thorac Cardiovasc Surg 2003; 123: 1007 -21 >250
Surgical ICU Mortality Effect of Average BG Van den Berghe et al (Crit Care Med 2003; 31: 359 -366) P=0. 0009 BG>150 110<BG<150 P=0. 026 BG<110
Hyperglycemia and Hospital Mortality 1826 consecutive ICU patients 10/99 thru 4/02, Stamford CT Krinsley JS: Mayo Clin Proc 78: 1471 -1478, 2003
Patient J. L. , December 15, 1922 February 15, 1923
Precipitating Event Beta-cell mass Genetic predisposition Antibody Normal insulin release Progressive loss of insulin release Glucose normal Overt diabetes C-peptide present No C-peptide present Age (y) Adapted from: Atkinson. Lancet. 2002; 358: 221 -229.
Hyperglycaemia (glucose toxicity) Protein glycation b-cell (genetic background) Amyloid deposition Insulin resistance “lipotoxicity” elevated FFA, TG
- Recommendations that cover dipeptidyl peptidase-4 inhibitors (DPP 4 i), glucagon-like peptide-1 (GLP-1) mimetics and sulfonylureas (SUs) refer to these groups of drugs at a class level - SGLT-2, sodium-glucose cotransporter -2 Adapted from Type 2 diabetes in adults: management. NICE Clinical guideline update (NG 28) 2015 [Accessed Dec 2015]. a. b. c. d. e. f. g. h. When prescribing pioglitazone, exercise particular caution if the person is at high risk of the adverse effects of the drug. Pioglitazone is associated with an increased risk of heart failure, bladder cancer and bone fracture. Known risk factors for these conditions, including increased age, should be carefully evaluated before treatment: see the manufacturers’ summaries of product characteristics for details. Medicines and Healthcare products Regulatory Agency (MHRA) guidance (2011) advises that ‘prescribers should review the safety and efficacy of pioglitazone in individuals after 3– 6 months of treatment to ensure that only patients who are deriving benefit continue to be treated’. Treatment with combinations of drugs including sodium–glucose cotransporter 2 inhibitors may be appropriate for some people at first and second intensification; see NICE technology appraisal guidance 288, 315 and 336 on dapagliflozin, canagliflozin and empagliflozin respectively. All three SGLT-2 inhibitors are recommended as options in dual therapy regimens with metformin under certain conditions. All three are also recommended as options in combination with insulin. At the time of publication, only canagliflozin and empagliflozin are recommended as options in triple therapy regimens. The role of dapagliflozin in triple therapy will be reassessed by NICE in a partial update of TA 288. Serious and life-threatening cases of diabetic ketoacidosis have been reported in people taking SGLT-2 inhibitors (canagliflozin, dapagliflozin or empagliflozin) or shortly after stopping the SGLT-2 inhibitor. MHRA guidance (2015) advises testing for raised ketones in people with symptoms of diabetic ketoacidosis, even if plasma glucose levels are near normal. Only continue GLP-1 mimetic therapy if the person has a beneficial metabolic response (a reduction of Hb. A 1 c by at least 11 mmol/mol [1. 0%] and a weight loss of at least 3% of initial body weight in 6 months). Be aware that, if metformin is contraindicated or not tolerated, repaglinide is both clinically effective and cost effective in adults with type 2 diabetes. However, discuss with any person for whom repaglinide is being considered, that there is no licensed non-metforminbased combination containing repaglinide that can be offered at first intensification. Be aware that the drugs in dual therapy should be introduced in a stepwise manner, checking for tolerability and effectiveness of each drug. MHRA guidance (2011) notes that cases of cardiac failure have been reported when pioglitazone was used in combination with insulin, especially in patients with risk factors for the development of cardiac failure. It advises that if the combination is used, people should be observed for signs and symptoms of heart failure, weight gain, and oedema. Pioglitazone should be discontinued if any deterioration in cardiac status occurs. The recommendations in this guideline also apply to any current and future biosimilar product(s) of insulin glargine that have an appropriate Marketing Authorisation that allows the use of the biosimilar(s) in the same indication. A consultant-led multidisciplinary team may include a wide range of staff based in primary, secondary and community care.
18
19
Regular Human Insulin Subcutaneous Tissue Insulin Aspart or Lispro Peak Time = 40 -50 min Capillary Membrane Peak Time = 80 -120 min
Regular Lispro 350 300 250 200 150 100 50 0 0 30 60 90 120 150 180 210 240 Plasma insulin (pmol/L) 400 500 450 400 350 300 250 200 150 100 50 0 Regular Aspart 0 50 Time (min) Meal SC injection 100 150 200 Time (min) Meal SC injection Heinemann, et al. Diabet Med. 1996; 13: 625– 629; Mudaliar, et al. Diabetes Care. 1999; 22: 1501– 1506. 250 300
6 NPH Glargine Glucose utilization rate (mg/kg/h) 5 4 3 2 1 0 0 10 20 Time (h) after SC injection End of observation period Lepore, et al. Diabetes. 1999; 48(suppl 1): A 97. 30
Plasma insulin (µU/ml) 75 Breakfast Lunch Dinner 50 25 4: 00 8: 00 12: 00 16: 00 Time 20: 00 24: 00 8: 00
Plasma insulin Breakfast Lunch Dinner Aspart Lispro or or or Glargine 4: 00 8: 00 12: 00 16: 00 Time 20: 00 24: 00 8: 00
6 -37
Results Rosenstock J, Riddle M, HOE 901/4002 Study Group. Diabetes 2002; 51(suppl 2): A 482. Abstract 1982 -PO
Riddle et al, Diabetes June 2002, Abstract 457 -p
Morning vs Bedtime Insulin Baseline: 9. 1 1. 0 A 1 C Change From Baseline (%) 0 Morning Glargine Bedtime Glargine -1 – 0. 96 Bedtime NPH – 0. 84 – 1. 24 -2 P=0. 008 P<0. 001 Adapted from Fritsche A et al, and the 4001 Study Group. Ann Intern Med. 2003: 138: 952
Large push button with low resistance Maximum dose 50 units Clear & uncomplicated dial, dials forward and back Large-scale numbers Audible clicks 1 unit increments Contains 300 units Novolin® 70/30, NPH, or R Novo. Fine® disposable needle Needle storage compartment Support shoulder
Normal insulin secretion at mealtime Change in serum insulin Regular insulin NPH insulin Premix 70/30 Baseline level SC injection Time (h)
Analog Mix 70/30: Serum Insulin Levels in Type 2 Diabetes * * Novo. Log® Mix 70/30 Premix Serum insulin (m. U/L) 100 Cmax 80 60 40 20 0 6: 00 PM 10: 00 PM Dinner *P<0. 05. Mc. Sorley. Clin Ther. 2002; 24(4): 530 -539. Time 8: 00 AM 1: 00 PM Breakfast Lunch 6: 00 PM
Analog Mix 70/30 vs 75/25 vs 70/30 Premix: Serum Insulin Levels in Type 2 Diabetes Serum insulin (m. U/L) 80 Aspart Mix 70/30 Lispro Mix 75/25 70/30 Premix 60 40 20 0 0 1 2 Time (h) Hermansen. Diabetes Care. 2002; 25(5): 883 -888. 3 4 5
Aspart Mix 70/30: Serum Glucose Levels in Type 2 Diabetes * Serum glucose (mg/d. L) 300 Aspart Mix 70/30 Premix * * 250 200 150 0 6: 00 PM 10: 00 PM Dinner *Glucose excursions 0 -4 h, P<0. 05. Mc. Sorley. Clin Ther. 2002; 24(4): 530 -539. 8: 00 AM Breakfast 1: 00 PM Lunch 6: 00 PM
Plasma insulin Breakfast Lunch Bolus Dinner Bolus Basal infusion 4: 00 8: 00 12: 00 16: 00 Time 20: 00 24: 00 8: 00
Photograph reproduced with permission of manufacturer.
Self-monitored BG (mg/d. L) 200 CSII (n=93) MDI (n=91) 180 160 140 120 100 BB AB BL AL Mean ± 2 SEM Bode, et al. Diabetes 52, (Suppl 1), 2003 Abstract 438. BD AD Midnight 3 AM
† p = 0. 0027 † Measurement of AUC 3000 mg/d. L during the 48 -hour continuous glucose monitoring period 2500 AUCglu (mg • hr/d. L) 2000 (glu) ≥ 80 n=63 in each treatment 1500 1000 500 0 CSII MDI Novo Nordisk, data on file (Study 2155/US)
9 8. 5 A 1 c 8 Glargine (n=16) CSII (n=14) 7. 5 7 6. 5 6 Baseline 4 weeks 8 weeks 12 weeks Boland, E. Diabetes 52, (Suppl 1), 2003 Abstract 192. 16 weeks
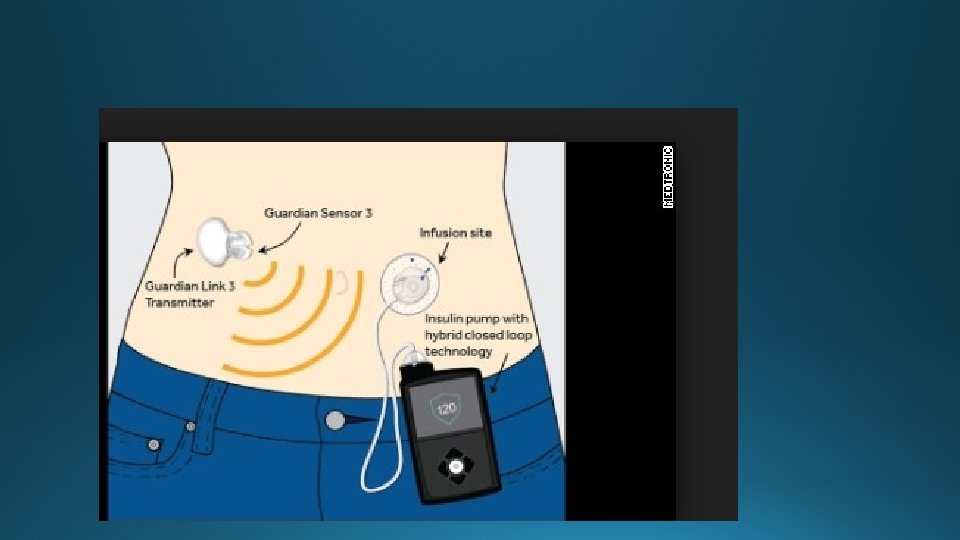
NICE GUIDANCE Continuous subcutaneous insulin infusion (CSII or 'insulin pump') therapy is recommended as a treatment option for adults and children 12 years and older with type 1 diabetes mellitus provided that: attempts to achieve target haemoglobin A 1 c (Hb. A 1 c) levels with multiple daily injections (MDIs) result in the person experiencing disabling hypoglycaemia. For the purpose of this guidance, disabling hypoglycaemia is defined as the repeated and unpredictable occurrence of hypoglycaemia that results in persistent anxiety about recurrence and is associated with a significant adverse effect on quality of life or Hb. A 1 c levels have remained high (that is, at 8. 5% [69 mmol/mol] or above) on MDI therapy (including, if appropriate, the use of long-acting insulin analogues) despite a high level of care.
CSII therapy is recommended as a treatment option for children younger than 12 years with type 1 diabetes mellitus provided that: MDI therapy is considered to be impractical or inappropriate, and children on insulin pumps would be expected to undergo a trial of MDI therapy between the ages of 12 and 18 years.
• Person has to look after pump rather than other way need for having back up insulin