Instituto de Ciencias del Corazn ICICOR Hospital Clnico
 Hospital Clínico Universitario de Valladolid Intra-cardiac shunts following")



 post-TAVR consists of an intracardiac fistulae that can")
 1. 2. 3. Mechanical compression of calcium Damage")


 1. 2. 3. Mechanical compression of calcium Damage")

 and the last in")




 in the aortic subannular region between the noncoronary valve and the")


 More symptomatic")

- Slides: 24
Instituto de Ciencias del Corazón (ICICOR) Hospital Clínico Universitario de Valladolid Intra-cardiac shunts following TAVR Ignacio J. Amat-Santos, MD, Ph. D, FESC Interventional Cardiologist Valladolid, Spain
Dr. Amat-Santos Dr. Zunzunegui Dr. Rojas Dr. Rodés-Cabau Dr. San Román
Complications following TAVR • TAVR is considered a less invasive treatment option • Specific periprocedural and late cardiac (5% to 61%) and non-cardiac (5% to 84%) complications may occur (1). • Several registries have addressed the most prevalent and worrisome complications post-TAVR, enabling a better understanding of how to predict and manage these situations: • • • annular rupture (2), coronary obstruction (3), cardiac tamponade (4), conduction disturbances (5), infective endocarditis (IE) (6), stroke (7). 1. 2. 3. 4. 5. 6. 7. Hamm CW, et al. Eur Heart J 2016 Barbanti Met al. Circulation 2013 Ribeiro HB, et al. J Am Coll Cardiol Intv 2013 Rezq A, et al. J Am Coll Cardiol Intv 2012 Urena M, et al. J Am Coll Cardiol 2012 Amat-Santos IJ, et al. J Am Coll Cardiol Intv 2015. Nombela-Franco L, et al. Circulation 2012
- 2011 -
Intra-cardiac shunts • Intracardiac shunts (ICS) post-TAVR consists of an intracardiac fistulae that can occur immediatedly or delayed after TAVR procedure • ICS may share mechanisms with other lifethreatening post-TAVR complications, such as annular rupture • This complication had been poorly described
Mechanism of ICS Potential aetiology (hypothesis) 1. 2. 3. Mechanical compression of calcium Damage caused by sheaths / guidewires Infective endocarditis
lni di A Aortic Prosthes is st nt f me 9 pt (17. 0 ) Aort c Prosth sis I I 30 pts (56. 6%) lsolat d n iv valv 7 p s (13. 2%), 1 solat d prosthet ic valv 4 pts (7. 5%}, nd combin d h TAVI-IE 2 p s (3. 8%) §
Ca ete· za ion a Car 6 10 r 10 o C rlo Co co J. Am Baseline characterist'cs Journal (Year) Case reported Rev sp Cardiol 2015 Can J Car·d ol 20 4 Eur Heart J 2014 J horac Cardiovasc 2009 Age (years) 75 86 72 84 66 Gender Male Male 'AVI procedure detail Valve type Corc. Valve 26 Core. Valve 26 lnit'al symptoms AR degree Moderate Mild Moderate (months) 4 0. 2 NO . 5 Yes + Ventricular 6 I Organism w n h enuiermuli Staoh a u r e u f nterococcu jaecali Staph epidermidi, Cor nehw re, ium arrhythmia 3 J Thorac Cardiovasc 20()() 88 Male Moderate Ye Strep. am. ; inosus
Mechanism of ICS Potential aetiology (hypothesis) 1. 2. 3. Mechanical compression of calcium Damage caused by sheaths / guidewires Infective endocarditis
Aseptic ICS
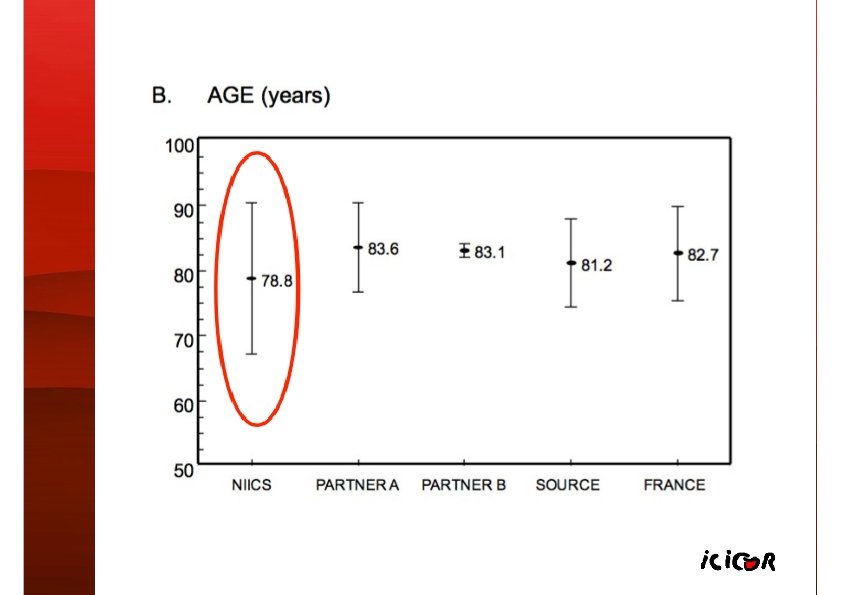
Baseline characteristics. The first case was published in 2009 (22) and the last in 2016 3 cases with transapical fistulas 28 cases with aseptic intra-cardiac shunts
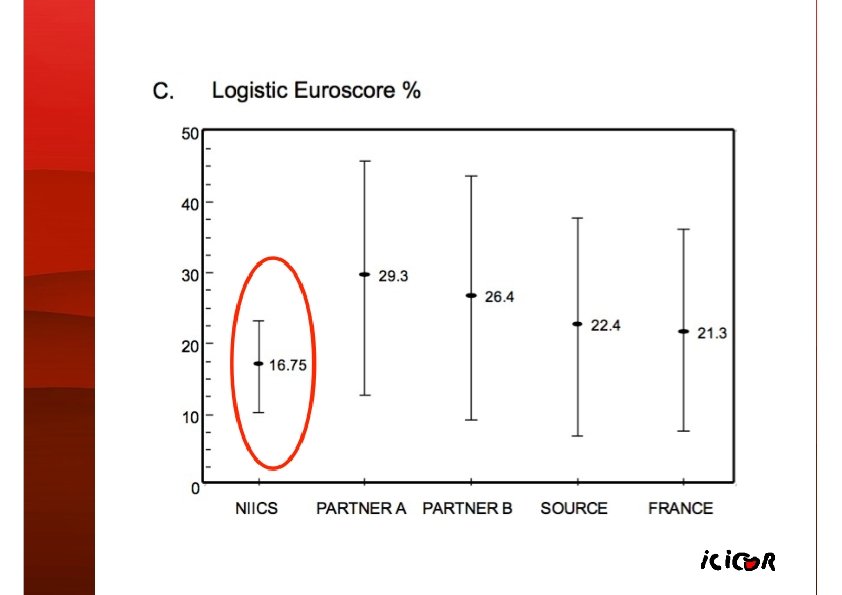
14. 3% prior chest wall radiation 39% coronary artery disease 10. 7% porcelain aorta CALCIFICATION 42. 8% severe aortic valve calcification (MDCT) 21. 4% asymmetrical extension to the LVOT.
Procedural characteristics • AVA: 0. 5+0. 5 cm 2, mean gradient: 53+10 mm. Hg • • Balloon-expandable TAVR: 85. 7% TF: 60. 7%, TA: 14. 3%, TSc: 3. 5% Post-TAVR moderate-severe AR: 1 pt Post-dilation: 14. 3% (not hemodynamic deterioration) • • Concomitant TAVR-related Complication: 39. 3%: AV block in 21. 4% Cardiac arrest in 7. 2% Cardiac tamponade in 7. 2%.
Development of AICS • 28 cases across 25 centers • Incidence ~ 0. 5% • • • Median time: 21 days (IQR: 7 -30) Intraprocedural diagnosis: 12 patients (43%) Mechanism: prosthesis / balloon / introducer • SYMPTOMS: • Heart failure (46. 4%) • • stroke (3. 6%) Asymptomatic (50%) • Mean Qp/Qs: 1. 8 + 0. 6 (range: 1. 3 to 3. 1)
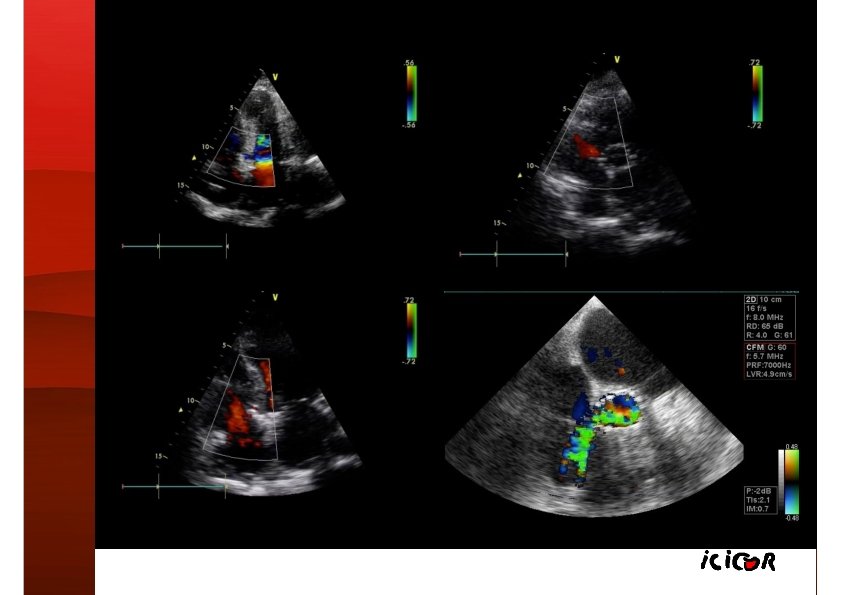
Location of AICS
Tear (black arrows) in the aortic subannular region between the noncoronary valve and the right coronary artery, near a calcium nodule (white arrows).
Management & Outcomes
Mark SD, et al. J Am Coll Cardiol Intv 2015.
Management & Outcomes All deaths in symptomatic patients (p = 0. 020) More symptomatic if higher Qp/Qs (1. 9+0. 6 vs. 1. 4+0. 1)
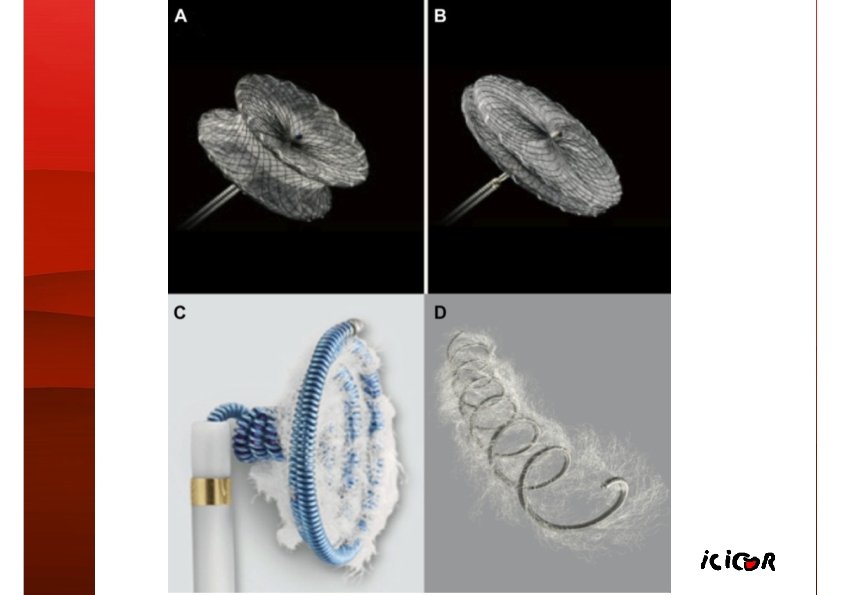
Final comments Post-TAVR AICS are uncommon Symtomatic: High 30 -day mortality if un-treated Symptomatic & High-risk: Percutaneous shunt closure with low-profile closure devices Asymptomatic ? ? further evaluation if high Qp/Qs ratios