Innovations in STD Clinic Practice Kees Rietmeijer MD




























 integrated with lab database – Electronic")






































 questions can rapidly reveal")
































 All patients")
 STI at index visit Yes 0.")






 Agency")
 of STD clinics")
 were actually playing the")







 STI Identified on e. CARD N % (95% confidence")



 sent")
")







- Slides: 147
Innovations in STD Clinic Practice Kees Rietmeijer, MD, Ph. D 2011 STD Update Indianapolis, April 20, 2011
GYT 2011 STD Awareness Month www. gytnow. org
Resources www. denverstdclinic. org
Resources www. cdc. goc/std/treatment/2010
Resources www. denverptc. org
Resources www. stdpreventiononline. org
Why STD Clinics Matter
Proportion of STIs Reported from STI Clinics Golden and Kerndt. Sex Transm Dis 2010; 37: 264 -265
Origin of STI Case Reports by Gender City and County of Denver - 2009 Denver Metro Health Clinic Men Women % % Chlamydia 46 13 Gonorrhea 54 20 Early syphilis 24 12 Rietmeijer and Mettenbrink. Sex Transm Dis 2010; 37: 591
Topics • • • Express / Fast-Track Visit System Electronic Medical Record Online Results Normalizing HIV testing EPT implementation Counseling Safe in the City In. Spot Online STI Testing Text Messaging for results and reminders
Express / Fast-Track Clinic Visits
Express / Fast Track Visits • Purpose – To enhance clinic efficiency and patient satisfaction through a process by which qualifying patients are offered a testing-only, no-exam visit
Express / Fast Track Visits • Who is eligible? – Asymptomatic patients regardless of • Demographics • Risk or contact status • Sexual preference
Express / Fast Track Visits • How is it done? – All patients go through triage after registration – Triage staff determines eligibility – Patients can opt for comprehensive visit if they desire regardless of eligibility for express visit – Patients are discouraged to opt for express visit if symptomatic, but are not denied
Express / Fast Track Visits • What is done? – HIV rapid test (unless opt-out) – RPR – CT and GC NAAT • Males: urine • Females: self-obtained vaginal swab – Gonorrhea cultures among at-risk MSM • Anal swab • Pharyngeal swab
Shamos et al. Sex Transm Dis 2008; 35: 336 -340.
Shamos et al. Sex Transm Dis 2008; 35: 336 -340.
Time & Motion Study • N = 751 – 182 Express – 569 Comprehensive • Wait time until triage – 30 (28 – 35) minutes • Triage – 2 (1 – 22) minutes Shamos et al. Sex Transm Dis 2008; 35: 336 -340.
Time & Motion Study • Median visit duration men – Comprehensive: 85 – Express: 52 minutes – Reduction: 39% • Media visit duration women – Comprehensive: 105 – Express: 46 – Reduction: 56% Shamos et al. Sex Transm Dis 2008; 35: 336 -340.
Return
Stockholm, September 3 1967: 5: 00 AM
Transfer to Electronic Medical Record System Denver, March 14 2005, 8: 00 AM
Health. Doc: The DMHC Electronic Medical Record
DMHC Electronic Medical Record • • Implemented in March 2005 to replace an outdated medical record system that was based on scannable forms and had been in existence since 1988 Built from a public health perspective – For example allows automatic reporting to state health department for reportable infections – Not focused on billing
DMHC Electronic Medical Record • Combines – registration system – electronic form document system – rules engine to ensure accurate and appropriately coded information – web portal interface – interface with the Denver Health patient registration (Siemens Invision) – interface with the Sunquest laboratory system – multiple inbound/outbound interfaces with the State Health Department.
DMHC Electronic Medical Record Java-based application – two application servers – a Siemens Rules Engine server – a Biztalk server – an OPENLink interface engine – a Microsoft SQL database server – An FTP server for transmitting encrypted data to/from State Health – a Crystal Report application for reporting, and clinical form data stored in XML.
Health. Doc: Advantages • All STI services in one system – DMHC – Jail services – Title X Family Planning – HIV counseling and testing • Yes, it does PEMS! – Outreach testing • • Bath House testing program Reproductive Health for Young Adults (Re. HYA) – Special testing events
Health. Doc: Advantages • Data Exchange – (partially) integrated with lab database – Electronic transfer of data between DMHC and state health department • • • PEMS data HIV (WB and NAAT) results RPR results – Automatic reporting of reportable infections – Easy abstraction and transfer of data to other parties: • STD Surveillance Network (SSu. N)
Health. Doc: Advantages • Relatively flexible – Many changes and updates can be performed inhouse at low cost • Data quality • Cost-effective • – Internal error checking system – Has reduced clerical data input and associated risk for errors Easily accommodates innovations – Online results – Automatic text messaging
Health. Doc: Disadvantages • • Steep learning curve, especially among staff not accustomed to electronic interfaces and data entry Potentially distracting from provider-patient interaction
Return
Providing STD Test Results Online
Results Online • How it works – Program started June 2008 – Originally, patients opted in and had to create their own (strong) password (opt-in) – Since December 2008, patients are given a login code and a predetermined password (opt-out) – Results available online after 5 days
Providing Test Results Online Lessons Learned • Proportion of patients receiving results online – Opt-in Phase: 25% – Opt-out Phase: 50% • • No net increase or decrease of patients receiving results Substantial savings in clerical time spent on answering phone calls
Wanted!! • Partnerships with clinics to evaluate the use of the Internet interface for their clinics
Return
Normalizing HIV Testing
Denver Metro Health Clinic • • • Largest STD clinic and HIV testing facility in Rocky Mountain region Provides: – confidential HIV testing in the STD clinic – confidential and anonymous testing in the HIV counseling and testing site integrated in the clinic In 2006: – ~16, 000 visits – 11, 300 HIV tests – 119 HIV diagnoses: ~50% of new HIV infections in the Denver Metro area; ~30% in Colorado.
HIV Testing at Denver STD Clinic Before November 2003 • • General consent for all procedures and testing, except HIV testing, obtained at registration HIV testing offered by clinician during the clinic visit, based on risk assessment Blood drawn for syphilis and HIV (if accepted) testing during the clinic visit HIV test used: standard EIA
HIV Testing at Denver STD Clinic After November 2003 • November 2003: Rapid HIV testing (Ora. Quick) offered – First as optional alternative to standard EIA – Routine after July, 2004 • • May 2004: Change in testing logistics March 2005: Introduction electronic medical record and switch from opt-in to opt-out HIV testing
HIV Testing at Denver STD Clinic Change in Testing Logistics • To avoid adding another 20 minutes to the visit, prior to clinic encounter: – Draw RPR blood before clinician sees patient – Offer HIV testing routinely – Obtain additional consent – Use RPR blood draw to collect extra tube for rapid HIV test
Evaluation • HIV testing acceptance and HIV test positivity was evaluated for 4 time periods: – Period 1: The year before introduction of rapid testing • December 2002 – November 2003 – Period 2: The 6 months following introduction or rapid testing, before logistical adjustment in the clinic and discontinuation of the standard test • December 2003 – May 2004 – Period 3: The 10 months following logistical adjustment, but before introduction of the electronic medical record and opt-out testing • June 2004 – March 2005 • April 2005 – September 2005 – Period 4: The 6 months following opt-out testing
Evaluation • Inclusion/Exclusion criteria – New problem visits – RPR performed – Previously known HIV+ excluded • Main outcome: HIV/RPR ratio – RPR used as the gold standard of routine testing
Impacts of Rapid Testing Denver Metro Health Clinic Percentage of patients who received their positive test results: Before: After: 66% 100%
HIV/RPR Ratio and HIV Positivity Rate by Period 0. 96 1. 00 0. 92 1. 5% 0. 86 0. 79 0. 80 0. 8% 0. 6% 0. 5% 0. 7% 0. 60 0. 0% Period I: Jan 2003 Nov 2003 Period II: Dec 2003 - Period III: Jun 2004 - May 2004 Mar 2005 Period IV: Apr 2005 Oct 2006 HIV: RPR Ratio HIV+ Rate HIV(+) Rate Ratio (HIV: RPR) January 2005 - October 2006
Return
Expedited Partner Therapy The DMHC Experience
EPT Legal Status in Colorado • • No legal impediments to provide EPT specifically endorsed by: – Colorado State Board of Medical Examiners • Policy 40 -10, issued 5/10/2001 – “It is the position of the Colorado Board of Medical Examiners that the public risk of untreated sexually transmitted infection is greater than the risk of complications from prescribing in this less than ideal setting” – Colorado State Board of Pharmacy • Policy 40 -4, issued 7/19/2007 – “It is the position of the Colorado Pharmacy Board that the public risk of untreated sexually transmitted infection is greater than the risk of complications from dispensing in this less than ideal setting”
EPT in Colorado http: //www. dora. state. co. us/Medical/policies/40 -10. pdf
EPT in Colorado www. dora. state. co. us/pharmacy/policies/40 -4. pdf
EPT in the STD Clinical Setting Questions • • • How to implement EPT in a busy STD clinic? What are the EPT acceptance rates among patients eligible for EPT? What are the reasons eligible patients decline EPT?
Denver Metro Health Clinic • 2007 Stats: – 19, 706 clinic visits – 1, 874 Ct cases (9. 5% of all visits) – Men: 9/9% – Women: 8. 9% – 700 GC cases (3. 5% of all visits) – Men: 4. 3% – Women: 2. 4%
History of EPT at DMHC • 11/2006 – 3/2007 –Demonstration Project • 3/2007 – 8/2007 –Review by pharmacy board • 9/2007 – Current –Standard of care
Partner Pack Chlamydia
Implementation of EPT at DMHC • Provider training • Changes to the electronic medical record –Treatment information includes EPT –Partner services questions include EPT and reasons why declined • Chart review and provider feedback
Acceptance Rates of EPT at Denver Public Health STD Clinic 70% EMR Prompt 60% Initiated 50% 40% Chart review and QA Begins 30% 20% EPT Documentation Required QA 10% Pilot Month/Year Mickiewicz et al. ISSTDR 2011 10 9/ 10 7/ 10 5/ 10 3/ 10 1/ 9 /0 11 09 9/ 09 7/ 09 5/ 09 3/ 09 1/ 8 /0 11 08 9/ 08 7/ 08 5/ 08 3/ 08 1/ 7 /0 11 9/ 07 0%
Chlamydia and Gonorrhea Reinfection Rates in Relation to EPT Acceptance Denver Metro Health Clinic, 2007 -2010 Re-infection rates among those returning to clinic for re-testing CT GC CT or GC* Accepted EPT 7/77 (9. 1%) 5/31 (16. 1%) 12/108 (11. 1%) Refused EPT 22/144 (15. 3%) 25/87 (28. 7%) 47/231 (20. 4%)
EPT Provider Rate - 2008 % Accepting EPT Number of Eligible Patients by Provider (N= 28)
Conclusions • • • Acceptance for EPT at the Denver Metro Health Clinic is about 50% Those accepting EPT had a 45% lower rate of GC or CT at (passive) follow-up Main reasons to decline EPT: – Partners already treated or currently in clinic – Patients want their partners to be seen by medical provider
Return
Counseling No Respect?
Rachel’s story D. What brings you in today? R. I’d like an STD check-up D. Just a check-up? R. Yes D. OK, sounds good. I first need to ask you a few questions, OK? R. OK D. How many sex partners have you had in the past 3 months? R. One
Rachel’s story D. Is your partner male or female? R. Male D. What types of sex do you have, oral, vaginal, anal? R. Oral and vaginal. D. You use condoms pretty much all the time? R. Yes D. OK, good. Doesn’t sound like you have a lot of risk, but you should always be using condoms, OK? Please feel free to take some when we’re done R. OK
Rachel’s story – Take 2 D. What brings you in today? R. I’d like an STD check-up D. What made you decide to get checked today? R. Well…. . I’m a bit embarrassed… D. I understand. It is not easy to come to a clinic like this, but the more I know about the reason why you came today, the better I can help you. So, what’s up? R. Well, it’s a bit of a story D. That’s fine, please tell me what happened R. Well, I broke up with my boyfriend about 3 months ago and I haven’t had sex since then.
Rachel’s story – Take 2 D. I see R. But then about 10 days ago, I went to this bar with a friend. I really wasn’t looking for sex or anything, but I met this cute guy and we kind-of got into it. I guess I had a few glasses too many and we ended up at his place and before I knew it we had sex end… D. Yes? R. Well I’m always very careful, with using condoms I mean, but we didn’t have condoms and now I’m really worried I may have gotten something….
Rachel’s story – Take 2 D. So what do you think you might be able to avoid something like this from happening again? R. I don’t know. Probably avoid bars… You know, I have this friend who met a guy on the Internet and they’re hitting it off pretty well. What do you think about that? D. Well, I have actually read some interesting research about that recently; as it turns out the Internet may be a pretty safe place for women to meet partners because you have the time to get to know a guy a bit better before you actually meet him in person R. So, perhaps that’s what I’ll try… D. Sounds like a great plan.
What’s the difference? • • The use of inquisitive (open-ended) questions can rapidly reveal the critical issues that formed the motive of the patient to seek care This information in turn can be used to start the patient to reflect on his/her risk behaviors and forms the entry point in the patient formulating and taking responsibility of setting a first (small) step to reduce this risk
Steps in Client-Centered Counseling • Personalized risk assessment • Support patient-initiated behavior change • Help patient recognize barriers to risk • • reduction Negotiate an acceptable and achievable risk reduction plan Refer patient to other specialized services, if needed
Open-ended Questions • What do you think your risk is for STD? • What happened the last time you had • • • sex? What made you decide not to use a condom? What made you decide to use a condom? What do you think you can do to reduce your risk for STDs the next time you have sex?
Does it work? YES!
Project Respect Main Results • Compared to standard education • messages, client-centered counseling resulted in overall STD reduction of 30% after 6 months and 20% after 12 months 2 -session prevention counseling was as effective as the 4 -session enhanced counseling Kamb et al. JAMA 1998; 280: 1161
Project Respect Relative effectiveness was greatest among those at highest risk for STI # STI prevented per 100 persons counseled – 20 years and younger – Exchange sex for money or drugs – STD at baseline – Lower education (<12 th grade) – Female – African American 9. 1 5. 9 5. 3 4. 3 3. 9 3. 2 Bolu et al. Sex Transm Dis 2004; 31: 469.
The bad news is… . . . that the good news is old news…
Prevention Counseling the main Challenge • How to implement prevention counseling in the busy practice setting? – Competing needs – Resource constraints – Lack of provider buy-in – Lack of supervisory buy-in
Prevention Counseling in The Real World Potential Solutions • Use ancillary counseling staff • Use ancillary, easily implementable devices – Written materials – Video – CDROM-based products
Prevention Counseling in The Real World Potential Solutions • • • Move away from the concept of counseling as a stand-alone intervention Rather, incorporate the core elements of effective counseling into the standard provider -patient interaction This requires: – A shift from the interview process as solely a closed-ended form-filling exercise – Training of clinicians to develop/enhance clientcentered counseling skills – an ongoing process
Effective behavior change at the patient level begins with behavior change at the provider level…
Return
Safe in the City
Study Rationale § 19, 000 incident STDs annually § STD clinics provide access to men and women likely to be infected and to acquire new infections over time § Yet behavioral interventions with counseling or multiple sessions are difficult to implement in busy medical settings § Recent interest in simple, easy to use, and low cost interventions for waiting rooms
Rationale continued § Previous research suggests benefits of videobased approaches, but subject to limitations: § Controlled research settings § Tailored videos § Single site § Inclusion of group counseling § Effectiveness of stand-alone video in ‘real-world’ setting is unknown
Safe in the City Project Overview § 5 -year CDC-funded multi-site study § Develop a brief video-based STD clinic waiting room intervention to reduce (or eliminate) STI and risky sexual behavior § Evaluate effectiveness in 3 publicly funded STD clinics in Denver, San Francisco, and Long Beach, CA.
Denver Waiting Room 2 nd TV
San Francisco Waiting Room
Long Beach Waiting Room
Intervention Development Considerations Waiting rooms in medical settings provide an underused opportunity to reach patients who are thinking about their health. Yet to be feasible and sustainable, interventions must: § Be easy and inexpensive to administer § Result in minimal interruption of patient flow § Require few clinic resources, especially staff time § Be acceptable to diverse clients
Formative Process § Identification of intervention medium, theoretical framework, and key messages by research team § Collaboration with award-winning film maker to integrate framework in an appealing product § Multi-step participatory process involving target audience, clinic staff, and community advisors § Intervention research study in 3 STD clinics
Intervention Development: Integrated Theoretical Framework Theory of Planned Behavior Social Cognitive Theory Information Motivation Behavior Model Core constructs grouped into interconnected elements → HIV/STD risk, knowledge, perception → Positive attitudes toward condom use → Self-efficacy/skills for condom negotiation, acquisition, use → Modeling of appropriate behaviors
Focus Groups § 3 sites held 12 focus groups with 176 participants § 3 different stages of video development: § § § Story line development Script development Post-production editing
What Is the Intervention? § 23 -minute video § 3 story lines § 2 cartoon animations § Condom variety and selection § Instructions for use § Posters in waiting and exam rooms
Story Line – Paul and Jasmine Things are getting more serious between Paul and Jasmine, but Paul “slips” and has a sexual encounter with Teresa gets an STD and tells Paul. Now Paul has to tell Jasmine.
Story Line – Rubén, Tim and Christina Rubén’s girlfriend Christina doesn’t know about his interest in men. Rubén and Tim have a casual sex encounter after meeting in a bar. Days later, Christina suspects something is wrong. She insists on a visit to the STD clinic.
Story Line – Teresa and Luis Teresa has recently met Luis. After her STD scare with Paul, Teresa is serious about wanting to use condoms. Now she has to convince Luis.
Safe in the City Evaluating Effectiveness of the Intervention
Maximizing Intervention Delivery § Identify environmental characteristics of waiting rooms § Observe waiting room flow § Determine appropriate playback frequency § Identify factors to assure viewership (goal: 80%) § § Assess and adjust to clinic staff acceptance of video Monitor viewership and audience response
Video Viewership as defined by watched most or all of the video + identified a main message
Overview of Study Design § Population: =~40, 000 patients attending 3 STD clinics from December 2003 – August 2005 § Study design: 2 arm non-randomized controlled trial § Arm assignment: alternating 4 -week control & intervention periods § Data collection: Passive review of clinic data & external surveillance records to ascertain new STI diagnoses* * gonorrhea, chlamydia, trichomoniasis, syphilis, and HIV
Characteristics of Clinic Populations, by Condition Control Intervention Sex Male 70% 69% Female 30% 31% Black, non-Hispanic 19% 18% White, non-Hispanic 46% Hispanic Other 25% 10% 25% 11% Age <25 >25 31% 69% Sexual orientation: MSM 22% 21% STI at index visit 15% 16% Race/ethnicity Warner et al. PLo. S Med. Jun 24 2008; 5(6): e 135.
Overall Effect of the Intervention on Laboratory-Confirmed Infection* Hazard Ratio (95% CI) All patients * = 9% reduction in STI incidence Warner et al. PLo. S Med. Jun 24 2008; 5(6): e 135. 0. 91 (0. 84 -0. 99)
Intervention Effect, by Characteristic Hazard Ratio (95% CI) STI at index visit Yes 0. 86 (0. 75 -0. 99) No 0. 93 (0. 84 -1. 04) Sex Males 0. 87 (0. 78 -0. 96) Females Sexual orientation Heterosexual MSM Age <25 >25 1. 06 (0. 89 -1. 25) Warner et al. PLo. S Med. Jun 24 2008; 5(6): e 135. 0. 84 (0. 71 -0. 98) 0. 90 (0. 79 -1. 03) 1. 02 (0. 88, 1. 17) 0. 85 (0. 77, 0. 95)
Advantages of Study Design • Evaluation in “real-world” setting • Use of STI outcomes • Inclusion of all clinic patients, wide generalizability • Controlled trial
Conclusions Safe in the City intervention was associated with a nearly 10% reduction in new STI This reduction can have significant public health benefit, with wide adoption by clinics. This relatively easy-to-implement, low cost intervention has the potential to reach large numbers of STD clinic patients and other high-risk populations.
CDC Diffuses Safe in the City § § Research article published by PLo. S Medicine on June 24, 2008 at 8 AM EST. Same day § Safe in the City website launched: § www. safeinthecity. org § SITC page and online kit request form launched on DEBI website: § www. effectiveinterventions. org
www. safeinthecity. org – since launch in June 2008: >10, 000 Page Visits
§ SITC viewed on DEBI site over 14, 000 times, including over 9, 000 views of online kit request form.
Safe in the City Kit Materials § DVD with video § § § and pdf posters User’s Guide Now Showing poster CDC documents
Safe in the City Kit Requests (June 24, 2008 – March 25, 2009) Agency type # of kit requests /shipped STD Clinics 424 / 347 (82%) Health Services Clinics 245 / 212 (87%) Community-Based Organizations (CBOs) 242 / 0 (--) Health Departments 252 / 153 (61%) Family Planning Clinics 169 / 131 (78%) Others (e. g. , Hospitals, Univ. Research, Univ. 369 / 141 (38%) Student Health Centers) Total 1, 701 / 984 (58%)
Implementation Evaluation • • Survey among: – A random sample (N=70) of STD clinics ordering the video through August (N=216) – All STD clinics who had ordered the video and requested technical assistance (N=58) Clinics surveyed between 3 and 6 months of ordering the video Survey response: 66% (N=85) Average clinic population: 4, 170 pt/yr
Implementation Evaluation • Of 85 respondents: – 31 (33. 7%) were actually playing the video • • 18 (34. 6%) from random sample 13 (32. 5%) from TA sample – Time from receipt to implementation • • 7 immediately 7 within a week 8 within 2 - 3 weeks 9 longer than 1 month – An additional 5 clinics indicated they would start playing the video within a month
Implementation Evaluation • Survey repeated 3 months after the first survey among clinics who responded on the first round, to: – Capture laggards – Capture longevity • Status: in progress
Return
In. Spot
Online PN - In. Spot
Results Clinic - Level Survey 1 Survey 2 Total Respondents 453 481 N % (95% CI) Heard of in. SPOT Ever Sent e. Card 22 4. 9 (3. 0 – 7. 4) 28 5. 8 (3. 8 – 8. 4) 1 0. 2 (0 – 0. 7) 10 2. 0 (0. 9 – 3. 7) Ever Received e. Card 2 0. 4 (0. 05 -1. 4) 5 1. 0 (0. 3 – 2. 3)
Results Clinic - Level • If you were diagnosed with an STI, how would you tell your partners? SURVEY 2 N % 95% CI Face-to-Face 430 89. 4 (86. 7 – 91. 1) Telephone 176 36. 6 (32. 3 – 40. 9) Written note or letter 18 3. 7 (2 – 5. 4) Text message 53 11. 0 (8. 2 – 13. 8) E-mail / Internet 23 4. 8 (2. 9 – 5. 7) Would not tell 12 2. 5 (1. 1 – 3. 9) Ask someone else to tell them 8 1. 7 (0. 6 – 2. 8)
Results – State Level PLo. S Publication 2008 2009 e. Cards Sent
Results State-Level (1/2008 – 6/2009) STI Identified on e. CARD N % (95% confidence interval) Chlamydia 297 15. 8 (14. 2 – 17. 4) Gonorrhea 307 16. 3 (14. 7 – 17. 9) Syphilis 225 11. 9 (10. 4 – 13. 4) Crabs/Scabies 537 28. 5 (26. 5 – 30. 5) Hepatitis A 73 3. 9 (3. 1 – 4. 7) Molluscum Contagiosum 85 4. 5 (3. 6 – 5. 4) Non-gonococcal urethritis 41 2. 2 (15. 5 – 2. 9) Shigella 23 1. 2 (0. 7 - 1. 7) Other STD 297 15. 7 (14. 1 – 16. 3) Total Cards 1885
Return
I Know Campaign • • Social marketing campaign to promote chlamydia and gonorrhea testing among high risk adolescent women of color in LA area – started in 2007 – Website – Bill boards in high-risk areas – Radio PSA Added online home test kit program, including online results in summer 2009 – Women only – Self-obtained vaginal swabs Rotblatt et al. STD Prevention Conference 2010, Atlanta GA.
“I Know” Campaign Results 6/09 – 2/10 • • • 25, 600 site visits 2, 572 kits ordered: 96% online 1, 350 kits returned 1, 286 kits testable 108 positive results (8. 4%) • • Received results: 87% Treatment confirmed: 88% Total cost project: ~ US 1 million Cost-effectiveness: $696, 000/QUALY Reported chlamydia cases Los Angeles 2008: 55, 276 – Chlamydia: 7. 9% – Gonorrhea: 0. 9% – Chlamydia and Gonorrhea: 0. 4% Rotblatt et al. STD Prevention Conference 2010, Atlanta GA.
Dutch National Chlamydia Screening Program • 315, 000 adolescents/young adults (16 -29 years) sent letter to participate, 2008 -10 – Amsterdam (sexually active) – Rotterdam (sexually active) – South Limburg (high-risk profile) • • • Invited to visit website and order kit Return kit Obtain results online after 1 week
Dutch Chlamydia Screening Program Preliminary Results • • 57, 000 letters sent (April-June, 2008) Response rate: 21% Participation rate: 15% (anticipated: 30%) Chlamydia positivity – Women: 4. 3% – Men: 4. 2% RIVM Report 210261006, Rijks Instituut voor de Volksgezondheid, 2009
Return
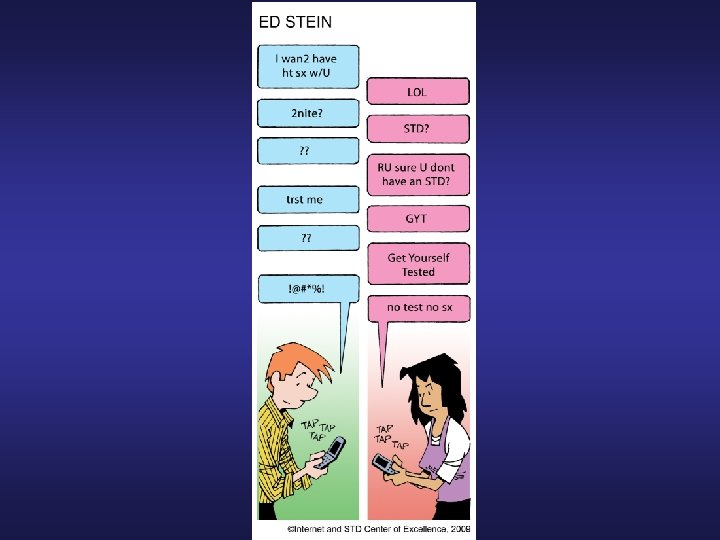
Cell Phone & Text Messaging Use Among STD Clinic Patients Clinic Survey Results Do you use a cell phone? 84. 7% Do you use text messaging on your cell phone? 90. 2% Is it OK to contact you via text message? 93. 5% Presented at ISSTDR, 2007
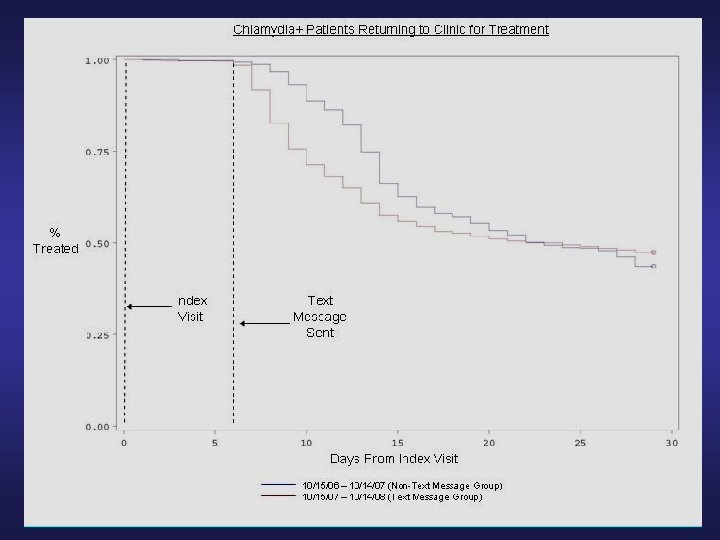
Text Messaging Projects Denver Metro Health Clinic • Project 1 Send text message to those testing positive for gonorrhea or chlamydia to call the clinic to receive their results (if they haven’t called back after 7 days)
Return
Final Thought “If you don’t change your direction, you’re going to end up where you’re headed” Chinese Proverb
THANKS!! kees. rietmeijer@dhha. org