Initiation of Insulin therapy in Type 2 Diabetes

Initiation of Insulin therapy in Type 2 Diabetes Saeid Kalbasi Ass. Prof. of Endocrinology and metabolism Loghman Hospital

Agenda • ADA-EASD Guideline • Why Basal? • Selection of Initial Insulin Regimens • Basal plus • Dosing and Titration

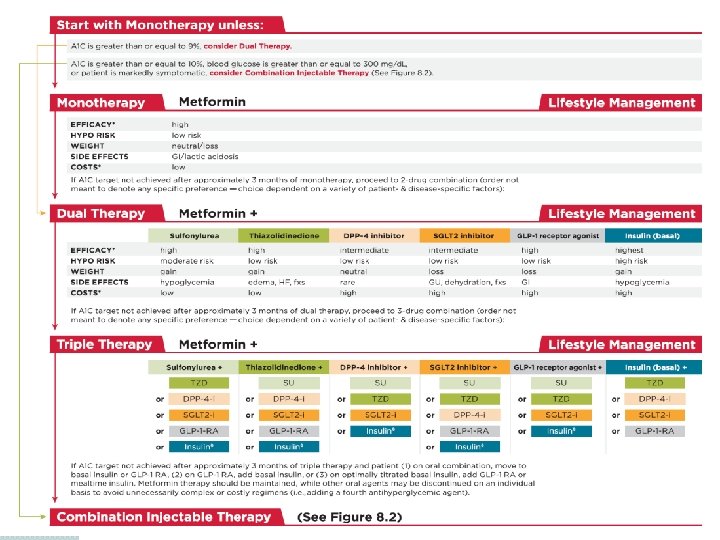
Modulation of the intensiveness of glucose lowering therapy in T 2 DM Diabetes Care 2015; 38: 140 -149; Diabetologia 2015; 10. 1077/s 00125 -014 -3460 -0
 Hb. A 1 c ≥ 10%or BS >300 mg/dl 2)")
Insulin Therapy Indications 1) Hb. A 1 c ≥ 10%or BS >300 mg/dl 2) Symptomatic (e. g. , sudden persistent weight loss, ketosis) 3) When multiple non-insulin therapies fail to achieve targets

Why Basal?

In T 2 DM contribution of fasting hyperglycaemia to overall glycaemia increases with worsening diabetes 290 patients with T 2 DM treated with diet or OHAs Baseline (normal) PG defined as 6. 1 mmol/l (110 mg/dl) ― threshold defined by ADA as the upper limit of normal PG at fasting or preprandial times 100 Relative contribution (%) 70% 50 Fasting 30% 0 <7. 3― 8. 4 8. 5― 9. 2 9. 3― 10. 2 Hb. A 1 c (%) quintiles >10. 2 ADA=American Diabetes Association; OHA=oral hypoglycaemic agent; PG=plasma glucose. Adapted from Monnier L, et al. Diabetes Care 2003; 26: 881― 5.

Treating fasting hyperglycaemia lowers the entire 24 -hour plasma glucose profile Type 2 diabetes 20 300 15 Hyperglycaemia due to increase in fasting glucose 200 10 100 5 Normal 0 6 Meal 10 14 Meal 18 Plasma Glucose (mmol/L) Plasma Glucose (mg/d. L) 400 0 22 2 6 Time of Day (h) Comparison of 24 -hour glucose levels in control subjects vs patients with diabetes (p<0. 001). Adapted from Hirsch I, et al. Clin Diabetes 2005; 23: 78– 86.

Selection of Initial Insulin

4 -T study: Optimal Insulin Treatment in Type 2 Diabetes Inclusion criteria • • Study design ≥ 18 years Type 2 DM ≥ 12 month Hb. A 1 c 7 -10% Metformin & SU N=708 Biphasic insulin 双相门冬胰岛素 2 x/day twice daily n=235 Prandial insulin 餐时门冬胰岛素 3 x/day thrice daily N=239 n=239 Exclusion criteria • • History of insulin History of TZD Cr ≥ 1. 47 mg/d. L Unstable angina, MI, CHF Basal insulin 基础地特胰岛素 once 1 x/day daily n=234 N=234 Primary outcome at year 1 + prandial insulin + basal insulin Primary outcome at year 3 + prandial insulin

4 -T Study 708 T 2 DM on dual OAD Year 1 Years 2 and 3 Comparison of 3 single insulin regimens, added to OADs* If A 1 C > 6. 5%, stop sulfonylurea and add a second insulin formulation R Add biphasic insulin twice a day Add prandial insulin at midday Add prandial insulin three times a day Add basal insulin before bed Add basal insulin once (or twice) daily Add prandial insulin three times a day *Intensify to a combination insulin regimen in year one if unacceptable hyperglycemia Holman RR et al. N Engl J Med. 2007; 357: 1716 -1730.

4 -T Study - Overview of Main Results Biphasic Prandial Basal Hb. A 1 c targets achieved + ++ ++ Mean SMBG level achieved + ++ ++ Fewer hypoglycemic episodes ++ + +++ Less weight gain + + ++ Less increase in waist circumference + + ++ N Engl J Med, 2009; 361: 1736 -47

Is it really necessary to cover every meal with an insulin bolus as soon as basal insulin therapy fails?

Six clinical trails supporting the Basal Plus strategy in T 2 DM

OPAL Study Oral Plus Apidra and Lantus 17

OPAL: Study Design the 1 st study supporting the Basal Plus approach Lankisch M, et al. Diabetes Obes Metab 2008 18

OPAL: Basal Characteristics Lankisch M, et al. Diabetes Obes Metab 2008 19

OPAL: Efficacy Data 20

OPAL: Safety Data 21

OPAL: Main findings § A single bolus of insulin glulisine added to once-daily basal insulin glargine results in an improvement of both Hb. A 1 c and PPBG levels. § The change in Hb. A 1 c is independent of the time of insulin glulisine administration, ie. Breakfast or main meal. ü Slightly better responder rate in main meal group § Low risk of hypoglycemia in both groups § No major weight gain with a Basal Plus approach

1. 2. 3 Study 23

1. 2. 3 study: insulin glargine with addition of one, two or three daily doses of glulisine Subjects: � Insulin naïve (785 entered study, 343 randomized) with type 2 diabetes (Hb. A 1 c ≥ 8. 0%) � Receiving 2 or 3 OHAs for ≥ 3 months (OHAs continued except sulfonylurea) Additional insulin glulisine once daily (n=115) Randomization (subjects with Hb. A 1 c >7. 0%, n=434) Insulin glargine (n=785) Additional insulin glulisine twice daily (n=113) 14 weeks Mean study entry values: Additional insulin glulisine three times daily (n=115) 24 weeks • Hb. A 1 c (%): 9. 8 • BMI (kg/m 2): 35. 0 Davidson MB, et al, Endocr Pract 2011

1. 2. 3 study: insulin glargine with addition of one, two or three daily doses of glulisine Responders in the whole population (n=785) Evolution of Hb. A 1 c in the randomized population (n=343) Glargine (alone) All subjects (n=785) 60 23% 10. 0 Additional subjects who achieved Hb. A 1 c <7. 0% with glulisine added to glargine 40 37% 20 0 Subjects who achieved Hb. A 1 c <7. 0% with glargine during run in 10. 19 10. 16 Hb. A 1 c (%) % achieving Hb. A 1 c <7. 0 80 Glargine plus glulisine (patients with Hb. A 1 c >7%) 9. 0 Glulisine 1 x Glulisine 2 x Glulisine 3 x 7. 44 8. 0 7. 40 7. 29 7. 0 Run in Hb. A 1 c in all subjects (n=785) = 9. 8 at run in and 7. 3 at randomization Davidson MB, et al, Endocr Pract 2011 Randomization Wk 8 Wk 16 Wk 24

1. 2. 3 study: insulin glargine with addition of one, two or three daily doses of glulisine 4 3 3. 7 3. 8 3. 9 2 1 20 0. 35 17. 1 15 10 12. 2 12. 9 5 0 0 x 1 x 2 Glulisine x 3 Severe or serious hypo (event/patient-year) Mean body weight change from baseline (kg) 5 Confirmed symptomatic hypo (event/patient-year) p=NS for all other pairwise comparisons p=0. 043 0. 30 0. 25 0. 26 0. 20 0. 15 0. 10 0. 00 x 1 x 2 x 3 Glulisine Sanofi-aventis data on file (1. 2. 3 study) x 1 x 2 Glulisine x 3

1. 2. 3 Study: Conclusion § Once- and twice-daily insulin glulisine were non -inferior to insulin glulisine administered three times daily.

Which Insulin Regimen? Stepwise Basal-Plus vs. Basal-Bolus? 28

Full. STEP Study Treatment intensification with stepwise addition of prandial insulin aspart boluses compared with full basal-bolus therapy A randomised, treat-to-target clinical trial Rodbard HW, et al. The Lancet Diabetes & Endocrinology 2014; 2 (1): 30 -37. 29

Full. STEP Study: Demographics & Characteristics Rodbard HW, et al. The Lancet Diabetes & Endocrinology 2014; 2 (1): 30 -37. 30

Full. STEP Study Rodbard HW, et al. The Lancet Diabetes & Endocrinology 2014; 2 (1): 30 -37. 31

Who should titrate the insulin dosage? Patient vs. Physician 32
 § Diabetes self-management is universally")
The START Study (Self-Titration with Apidra to Reach Target) § Diabetes self-management is universally regarded as a foundation of diabetes care. § In a randomized non-inferiority trial, we determined whether comparable glycemic control could be achieved by self-titration vs. physician titration of a once-daily bolus insulin dose in patients with T 2 DM who are unable to achieve optimal glycemic control with a basal insulin. Harris et al. Diabetes Care. 2014; 37(3): 604 -10. 33

START Study: Conclusions § In stable patients with T 2 DM who are receiving doses of basal insulin glargine who require bolus insulin, a simple bolus insulin patientmanaged titration algorithm is as effective as a physician-managed algorithm. Harris et al. Diabetes Care. 2014; 37(3): 604 -10. 34

How to titrate the insulin dosage? Simple algorithm vs. Carbohydrate counting 35
 study Basal Bolus therapy delivers comparable good efficacy whatever the")
3. 1 3502 (CHO) study Basal Bolus therapy delivers comparable good efficacy whatever the titration algorithm used 8. 5 p=NS 80 60 8. 0 73 69 40 20 Hb. A 1 c (%) % achieving Hb. A 1 c <7. 0 100 Simple algorithm CHO counting 8. 16 7. 5 7. 0 6. 70 ADA/EASD target 6. 5 0 Simple algorithm CHO counting 6. 0 Baseline 6. 54 p=NS 2 6 12 18 Endpoint Weeks Bergenstal RM, et al. Diabetes Care 2008; 31: 1305– 10 36

• The most precise and flexible prandial coverage is possible with “basal-plus/bolus” therapy Hb. A 1 c > target FPG on target PPG > target Hb. A 1 c > target FBG > target Basal insulin Basal plus Basal bolus Basal plus Basal + 2 prandial Basal + 1 prandial once daily (treat-to-target) Lifestyle ± Metformin ± 2 nd/3 rd Drug Hb. A 1 c > target Progressive deterioration of -cell function Adapted from Raccah et al. Diabetes Metab Res Rev 2007; 23: 257. Basal + 3 prandial

When to add the first prandial insulin

Dosing and Titration

Dosing

Titration

Key Message Individualization of therapy is key, incorporating the degree of hyperglycemia needing to be addressed and the overall capacities of the patient. 42

Conclusion § Any insulin will lower glucose and Hb. A 1 c. �A timely insulin therapy in type 2 diabetes could protect β-cell function and facilitate effective glycemic control. § No insulin is working by itself alone § All insulins are associated with some weight gain and some risk of hypoglycemia. § Effective dose titration is required to optimise insulin therapy. § First, Basal insulin and after that, the Prandials. 43

So, why not to do! Start Insulin At The Right Time! Adjust & Follow! 44
- Slides: 43