Initial Therapy for Follicular Lymphoma Does it Matter








 1. 0 Median (months) 0. 9 0. 8 B-R n. y.")

 PR OR of CR")
 100 – Survival 80 – 60 – 40")

? Lancet, Jan 1, 2011.")

 1 st line FL")







 • Accruing 389 patients with low-tumor-burden stage III/IV FL Rituximab 375")





- Slides: 32
Initial Therapy for Follicular Lymphoma – Does it Matter What Treatment We Use? Brad Kahl, M. D. Skoronski Chair of Lymphoma Research University of Wisconsin
FL Treatment • Disease generally “incurable” • Prognosis generally “good” • Lots of treatment options – Can make decision making difficult
My approach to a patient with newly diagnosed with FL Low Tumor Burden High Tumor Burden Symptoms absent Watch/Wait vs. single agent rituximab R-chemo +/- MR vs. Watch/Wait Symptoms present Single agent rituximab vs. R-chemo +/- MR
GELF Criteria – 3 nodes greater than 3 cm – Single node greater than 7 cm – Systemic symptoms or any symptoms – Compression or risk of compression of vital organ – Leukemic phase – Cytopenias due to marrow infiltration – Splenomegaly greater than 16 cm
Spanning the Continuum of Care: Optimizing Patient Outcomes in NHL clinicaloptions. com/oncology The Follicular Lymphoma International Prognostic Index (FLIPI) § FLIPI score used to predict outcomes of therapy based on adding number of risk factors (each factor = 1 point) – Older than 60 yrs of age – LDH > ULN – Ann Arbor stage III/IV disease – > 4 involved nodal sites – Hb < 12 g/L FLIPI Risk Group Low Intermediate High Risk Factors, n Patients, % 5 -Yr OS, % 10 -Yr OS, % Relative Risk 0 -1 36 90. 6 70. 7 1. 0 2 37 77. 6 50. 9 2. 3 ≥ 3 27 52. 5 35. 5 4. 3 Solal-Céligny P, et al. Blood. 2004; 104: 1258 -1265.
Symptomatic, High Tumor Burden FL Low Tumor Burden High Tumor Burden Symptoms absent Watch/Wait vs. single agent rituximab R-chemo +/- MR vs. Watch/Wait Symptoms present Single agent rituximab vs. R-chemo
Which chemo backbone? • R-CHOP vs. R-CVP vs. R-FM – No OS difference – R-CHOP and R-FM better PFS than R-CVP • 3 yr - 60% vs 47% – R-CHOP better safety profile than R-FM • Fewer infections • What about R-bendamustine? Federico et al, JCO April 2013.
Lancet, Feb 2013
PFS: follicular (n=279) 1. 0 Median (months) 0. 9 0. 8 B-R n. y. r. CHOP-R 40. 9 0. 7 0. 6 0. 5 0. 4 0. 3 0. 2 Hazard ratio, 0. 61 (95% CI 0. 42 - 0. 87) 0. 1 p = 0. 0072 0. 0 0 12 24 36 48 60 72 84 96 months MJR
Blood, May 2014
Primary Endpoint: Complete Response Rate Evaluable: IRC CR (95% CI) PR OR of CR + PR (95% CI) NI, noninferior; Sup, superior. BR (n = 213) R-CHOP/R-CVP P Value (n = 206) (NI) (Sup) CR Ratio 31 (25. 3 -38. 2) 25 (19. 5 -31. 7) 65 66 97 (93. 3 -98. 7) 91 (86. 0 -94. 4) 1. 26 (0. 93 -1. 73) 0. 0225 0. 1269
PFS: Investigator Assessment Randomized Patients (immature) 100 – Survival 80 – 60 – 40 – 20 – — BR — R-CHOP/R-CVP │ Censored 0– I I I I 0 4 8 12 16 20 24 I I 28 32 Months I I I I 36 40 44 48 52 56 60 64
Conclusions • R-bendamustine appears to be a reasonable alternative to R-CHOP • Stil Trial – More efficacious and less toxic • BRIGHT trial – Comparable efficacy – Toxicity tradeoff
What about maintenance rituximab (MR)? Lancet, Jan 1, 2011.
Maintenance Rituximab? • • Is PFS and time to next chemo benefit enough? Does QOL need to be improved by MR? Do infections cause concerns? Will patients respond less well to rituximab based regimens later? • What to tell patients? – I discuss “pros” and “cons”. – I find most (but not all) patients choose MR
RELEVANCE Study Design (Rituximab and LEnalidomide versus Any Ch. Emotherapy) 1 st line FL N=1000 R 2 Maintenance R + Chemo Rituximab Maint. R • R+Chemo: • Investigator’s choice of R-CHOP, R-CVP, BR • Lenalidomide 20 mg for 6 cycles, then 10 mg if CR • GELA + North American Cooperative Effort
Asymptomatic, High Tumor Burden FL Low Tumor Burden Symptoms absent Watch/Wait vs. single agent rituximab Symptoms present Single agent rituximab vs. R-chemo High Tumor Burden R-chemo +/- MR
Asymptomatic, High Tumor Burden • Generally recommend R-chemo followed by MR – Likely to recommend BR induction – MR optional as before • Some patients barely qualify as HTB – Reasonable to start on W&W but monitor closely for progression
Asymptomatic, Low Tumor Burden Symptoms absent Symptoms present High Tumor Burden R-chemo +/- MR vs. Watch/Wait Single agent rituximab vs. R-chemo +/- MR
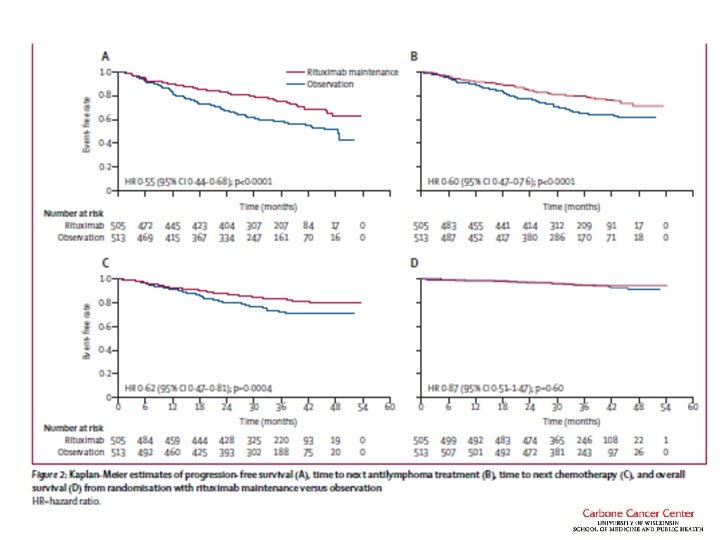
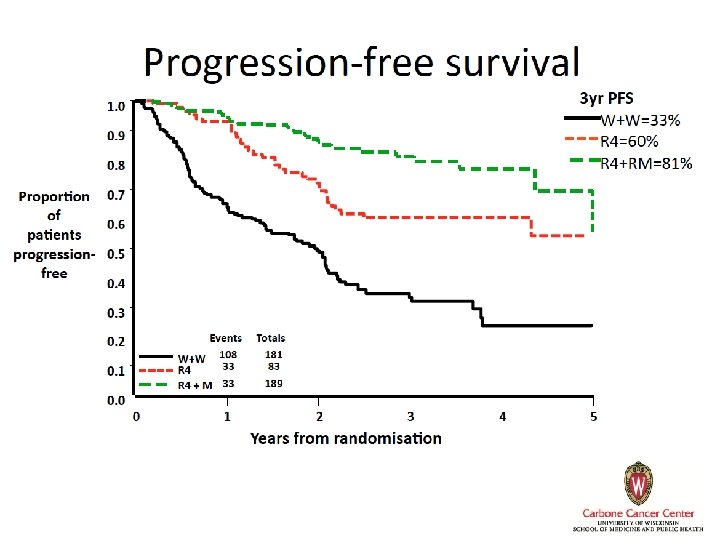
Asymptomatic, Low Tumor Burden • Watch and wait remains a reasonable standard – 3 RCTs failed to demonstrate any overall survival advantage for immediate therapy • All in the pre-rituximab era – No trials of R-chemotherapy in this patient population – One trial of rituximab vs. watch and wait
How to interpret? • PFS benefit without an OS benefit – Does that warrant routine Rx with rituximab? – What endpoints do you and your patients value? • Is there a QOL benefit for associated with remission?
QOL Results • A minority of patients suffered from anxiety and depression (13% and 3%) • Patients assigned to rituximab had less anxiety than those on W&W • Most patients functioned quite well and adapted to their illness over time
My conclusions • Given lack of OS advantage, perfectly acceptable to W&W • Some benefits to rituximab – PFS and Time to Next Treatment – Discuss with patients • For a minority of patients with significant anxiety and coping issues, rituximab has benefit – Try and ascertain who these folks are • Some patients better served by rituximab
ECOG 4402 (RESORT) • Accruing 389 patients with low-tumor-burden stage III/IV FL Rituximab 375 mg/m 2 qw 4 CR or PR R A N D O M I Z E Rituximab maintenance 375 mg/m 2 q 12 w Rituximab re-treatment at progression 375 mg/m 2 qw 4 • Primary end point: time to rituximab failure • Secondary end point: time to first cytotoxic therapy http: //www. clinicaltrial. gov/ct/show/NCT 00075946? order=2. Accessed May, 2005.
E 4402 Results • No difference in time to treatment failure • Slight benefit in time to first chemo – 95% vs. 86% chemo free at 3 yrs • Came at a cost of 3. 5 x more rituximab • Both arms well tolerated – Slightly more toxicity on maintenance • Conclusion – Retreatment is our preferred strategy Kahl at el, JCO. In Press.
Symptomatic, Low Tumor Burden Symptoms absent Symptoms present Low Tumor Burden High Tumor Burden Watch/Wait vs. single agent rituximab R-chemo +/- MR vs. Watch/Wait R-chemo +/- MR
Symptomatic, Low Tumor Burden • CC is usually fatigue – Make sure not some other cause • Single agent rituximab seems reasonable – Low risk “experiment” • R-chemo – >95% response rate
Summary
Questions?