INHALATION INJURY Presented by Ghofran mahmood Yasmeen doumi

INHALATION INJURY Presented by: Ghofran mahmood Yasmeen doumi Aseel khresat Supervised by: Dr. Saleh Abualhaj

OUTLINE: ● ● ● Introduction Epidemiology Classification Risk factors Pathophysiology Diagnosis Management Prognosis Complications Differential diagnosis References

INTRODUCTION inhalation injury causes a heterogeneous cascade of insults that increase morbidity and mortality among the burn population. Manifest within the first 5 days after injury. despite major advancements in burn care for the past several decades there remains a significant burden of disease attributable to inhalation injury. smoke inhalation injury can be defined as damage to the respiratory tract caused by

EPIDEMIOLOGY ● According to FEMA records, in 2015, there were 380, 940 residential fires, resulting in 2565 deaths, and 11, 475 fire-related injuries in the United States. ● The leading cause of death from fire injuries remains a respiratory failure, and smoke inhalation injuries affect one-third of all burn injury victims. ● Incidents increase in extreme of age and in those with physical or cognitive abilities or under influence of drugs or alcohol

CLASSIFICATION 1. Thermal injury : to the mouth, oropharynx, and larynx 1. chemical and particulate constituents of smoke: particulates are micro particles less than 0. 5 micrometer that goes to prank heels and cause bronchospasm and surfactant loss and edema 1. metabolic asphyxiation: carbon monoxide (CO) and cyanide(systemic toxicity).

RISK FACTORS More common in the elderly, immobile, and children Fire in an ENCLOSED space Carbonaceous sputum Raspy or hoarse voice Facial burns (2 nd degree or worse) Singed facial hair Arterial Pa. O 2 < 60 mm. Hg Carboxyhemoglobin >15% Bronchospasm or wheezing

PATHOPHYSIOLOGY/UPPER AIRWAY ● ● ● Injuries to the upper airway may induce massive edema of the tongue and epiglottis and obstruct the supraglottis. Airway edema occurs during the late phases of resuscitation. The initial evaluation is a poor indicator of the severity of airway swelling.

PATHOPHYSIOLOGY/LOWER AIRWAY ● lower airway is damaged by smokerelated toxins, which are generated from the incomplete combustion of certain products. 5 Burning cotton, rubber, and plastic. ● aldehydes, nitrogen dioxide, sulfur dioxide, ammonia, and chlorine, which turn into strong acids or alkalis when combined with water in the lower airway. ● These toxins damage epithelial and capillary cells of the tracheobronchial

CONT. . . ● Pseudomembranes may also form in the trachea or bronchi causing bronchiolitis. ● Damage to airway tissue causes increased mucus production, edema, denudation of epithelium, and mucosal ulceration and hemorrhage. ● Damage to the lung parenchyma causes both epithelial and endothelial damage resulting in pulmonary edema and possibly acute respiratory distress syndrome (ARDS) due to widespread alveolar-capillary leak.

DIAGNOSIS/HISTORY *Suspect inhalation injury in any patient coming from a house/building fire or a car fire. Essentially, any enclosed space. Syncope + a house fire? Higher index of suspicion Does your patient smoke? Do they have existing lung disease? Have a higher index of suspicion. Was extrication from the fire prolonged? Kids are at a high risk because they tend to hide in closets during a fire rather than escape. The elderly or immobile have physical barriers to escape.

CONT. . . 1. important to elucidate whether the exposure was to smoke, flames, and/or possible chemicals (both industrial and household) 2. Duration of exposure 3. burning sensation in nose or throat 4. cough with increased sputum production, stridor, and dyspnea with rhonchi or wheezing. 5. Symptoms of odynophagia 6. systemic symptoms like a headache, delirium, hallucinations,

DIAGNOSIS/PHYSICAL EXAMINATION looking for 1. facial and intranasal burns 2. carbonaceous material or soot in the mouth or sputum 3. accessory muscle usage, tachypnea, cyanosis, stridor, and rhonchi/rales/wheezing.
 2.")
DIAGNOSIS/WORK UP 1. Serial chest radiographs (often negative early in smoke inhalation injury) 2. Complete blood count (CBC) 3. Pulse oximetry (may be falsely elevated with carbon monoxide exposure) 4. Arterial blood gas (ABG) 5. Carboxyhemoglobin level 6. Cyanide level 7. Pulmonary function testing: The flow-volume loop is a very sensitive noninvasive test 8. Fiberoptic Bronchoscopy the standard for the diagnosis

Fiberoptic bronchoscopy of patient on post-burn day 0 Fiberoptic bronchoscopy of patient on postburn day 4

Fiberoptic bronchoscopy of patient on postburn day 10 Abbreviated Injury Score grading scale for inhalation injury on bronchoscop

MANAGEMENT 1. removing the patient from the exposure area 2. Maintain secure airway: Intubation, tracheostomy if necessary 3. aggressive pulmonary hygiene for (edema, hemorrhage, and mucosal sloughing) 4. Bronchodilators (Beta-2 -adrenergic agonists like albuterol and salbutamol) 5. steroids, in either inhaled or intravenous form, have not been proven beneficial in clinical studies. 6. antibiotics should be started promptly when an empiric diagnosis of pneumonia is made. 7. Carbon monoxide treatment includes high oxygen therapy. 8. antidote, hydroxocobalamin, may be given in patients with high suspicious of cyanide poisoning.

INTUBATION The need for airway control must always be assessed and intubation should be considered if any of the following significant injuries to the upper airway is suspected: 1. 2. 3. respiratory distress stridor hypoventilation 4. use of accessory respiratory muscles 5. blistering or edema of the oropharynx 6. deep burns to the face or neck.

PROGNOSIS is noteworthy that mortality rates for inhalation injury have not changed over the past five decades, though improvements in standards of care for severe burn injuries have. [1] Supportive strategies are vital in the management of inhalation injury, yet, more trials are needed to demonstrate sufficient evidence for many of the pharmacological agents. Also, more promising results have been achieved with unconventional modes of ventilation such as HFPV in addressing physiologic derangements from inhalation injury.

COMPLICATIONS Severity generally correlates with exposure time, Complication rates are higher in people with a history of underlying lung disease as well, such as COPD and asthma. Short-term complications(4 -5 days): pneumonia. Acute respiratory distress syndrome and pulmonary edema. Long-term complications(less common): subglottic stenosis, bronchiectasis, and bronchiolitis obliterans Patients who have been exposed to carbon monoxide are also known to have long-term neurological complications (1 -3 wks)
 Asthma Aspiration pneumonitis/pneumonia Chronic obstructive lung disease")
DIFFERENTIAL DIAGNOSIS Acute respiratory distress syndrome (ARDS) Asthma Aspiration pneumonitis/pneumonia Chronic obstructive lung disease Congestive heart failure Interstitial lung diseases Pulmonary embolism Pneumonia: Viral or bacterial Pneumothorax

REFERENCES https: //www. statpearls. com/Article. Library/viewarticle/23532 https: //www. dovepress. com/assessing-inhalation-injury-in-theemergency-room-peer-reviewed-fulltext-article-OAEM https: //present 5. com/thermal-and-inhalation-injury-chapter-39 written-by/

THANK YOU

CYANIDE POISONING Done by : Aseel khriesat Supervised by: Dr. Saleh Abualhaj Done by: Aseel khriesat Supervised by: Dr. Saleh Abualhaj

INTRODUCTION • Cyanide is a mitochondrial toxins that is among the most rapidly lethal poisons known to man. used in both ancient and modern times as a method of execution, cyanide causes death within minutes to hours of exposure. Though significant cyanide poisoning is uncommon it must be recognized rapidly to ensure prompt administration of life saving treatment.

EPIDEMIOLOGY • Fire-in industrialized countries, the most common cause of cyanide poisoning is domestic fires. cyanide can be liberated during the combustion of products containing both carbon and nitrogen. these products include wool, silk, polyurethane(insulation, upholstery), polyacrylonitrile s(plastics), melamine resins(household goods), and synthetic rubber. >>>>>>furniture • Vehicular fires can also expose victims to cyanide.

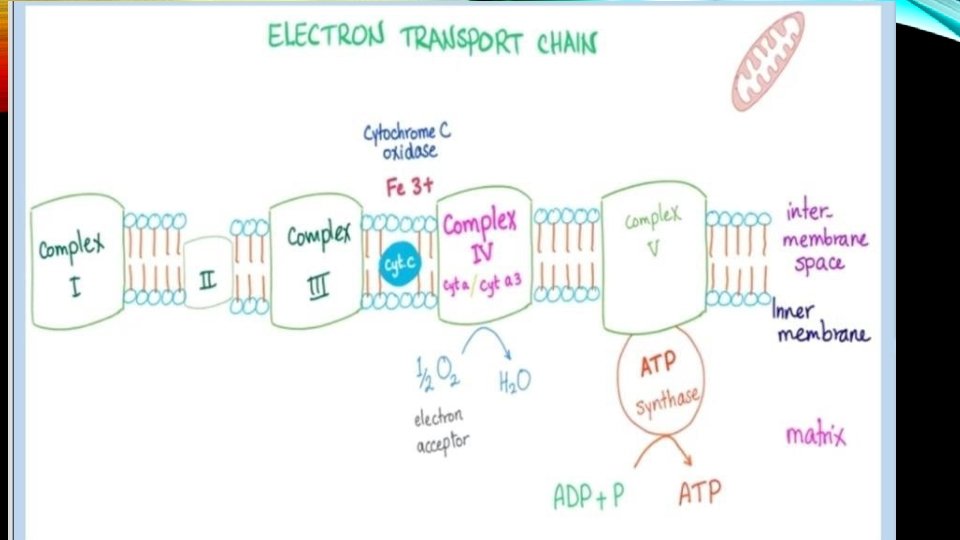
PATHOPHYSIOLOGY • In normal cellular metabolism, most adenosine triphosphate is generated from oxidative phosphorylation. an important part of this process is the shuttling of electrons through the mitochondrial cytochrome complex(also known as the electron transport chain) • Cyanide avidly binds to the ferric ion (fe 3+)of cytochrome oxidase a 3, inhibiting this final enzyme’s in the mitochondrial cytochrome complex. when this enzyme activity is blocked, oxidative phosphorylation ceases. the cell then switch to anaerobic metabolism of glucose to generate ATP. • Anaerobic metabolism leads to the formation of lactic acid and the development of metabolic acidosis. hydrogen ions produced by ATP hydrolysis are no longer consumed in aerobic ATP production , exacerbating this acidosis. serum bicarbonate decrease as it buffers excess acid, leading to an increased inion gap. • Despite an ample oxygen supply, cells cannot utilize oxygen because of their poisoned electron transport chain. this functional(or histotoxic)hypoxia is particularly deleterious to the cardiovascular and central nervous systems(especially the basal ganglia). a number of other mechanisms may exacerbate brain injury. Cyanide’s nonspecific inhibition of antioxidant(such as catalase, glutathione reductase, and superoxide dismutase)results in the accumulation of toxic oxygen free radicals. Cyanide stimulate N-methyl -D-Aspartate receptors, inducing apoptotic cell death. It also inhibits glutamic acid decarboxylase , the enzyme responsible for the formation of the inhibitory neurotransmitter gamma-aminobutyric acid (GABA) from glutamic acid. consequently , increase the risk of seizure as GABA level fall. although cyanide has primary affinity for ferric(fe 3+)iron, a small amount may bind to the ferrous (fe 2+)iron of hemoglobin, forming cyanohemoglobin, which is unable to transport oxygen, thereby furthur exacerbating tissue hypoxia.

CLINICAL PRESENTATION • Clinical features of cyanide poisoning are dependent upon the route , source, and severity of exposure. • Central nervous system and cardiovascular system dysfunction are most prominent. Symptoms and signs can include the following ; • Central nervous system ; headache, anxiety , confusion, vertigo, loss of consciousness, seizures • Cardiovascular-initially tachycardia and hypertension the bradychardia and hypotension, and dysrhythmias • Respiratory-initially tachypnea then bradypnea, pulmonary edema • Skin-flushing (cherry-red color)this sign is present in minority of cyanide toxic patients. normal skin color was more common skin findings • Miscellaneous-rhabdomyolysis, bright red venules see on fundoscopy, bitter almond(approximately 60% of the population) • Renal-renal failure

; sys i e m Central nervous N i a n 1 1 e s 1: a· 11 ons Early (due to hypoxia) Anxiety Headach e Giddiness Dizziness Confusion Mydriasis Bright retinal veins (elevated venous Po 2 Late Decreased consciousness Seizures Paralysis Coma ) Respiratory Early Hy p e rv e n t i la t i o n and t a c h y p n e a ( d u e t o h y p o x i c s t i m u l a t i o n of peripheral a n d central chemoreceptors) Late A b s e n c e of cyanosis (caused b y a n increase 1 n o x y g e n content in v e n o u s blood) Hy p ove nti Ia t i o n Apnea (cells cannot take up oxygen) Cardiovascular Early Tachycardia Late Hy p o t e n s i o n Sup r a v e n t r i c u l a r t a c h y c a r d i a Atrioventricu lar blocks V e n t r i c u l a r fib ri. Ilati o n Asystole

LABORATORY EVALUATION Specific testing-specific testing in cases of potential cyanide poisoning should also include the following; Basic chemistries(eg, na+, cl-, k+, hco 3 -)and arterial blood gas to assess for anion gap metabolic acidosis (high anion gap metabolic acidosis) Serum lactate concentration to confirm hyperlactatemia(lactate concentration of 8 mmol/l or greater have been shown to be both 94% sensitive and 70% specific for cyanide poisoning in smoke inhalational victim) Central venous blood gas , if possible, to assess venous-arterial PO 2 gradient(a narrowing of the venous-arterial po 2 gradient venous hyperoxia may be seen in the cyanide poisoning patient)

DIAGNOSI S • Cyanide poisoning is an uncommon entity. Therefore, making the diagnosis requires that the clinician maintain a high index of suspicion based on history and clinical presentation. cyanide poisoning should be suspected in any person exposed to smoke from a fire in a closed space and those with : • Soot in mouth • Altered mental status • hypotension

TREATMEN DECONTAMINATION-patient poisonined by cyanide T through inhalational must be rapidly removed from the source , and there clothing taken off and appropriately discarded. Secure airway , breathing , circulation. intubation is usually required. administer high flow oxygen 100% by non rebreather face mask regardless of pulse oximetry reading Do not perform mouth to mouth resuscitation in case of suspected cyanide toxicity Treat hypotension with rapid IV boluses of isotonic fluid and vasopressors as needed. treat seizures with benzodiazepine (ef. diazepam 5 mg IV) Obtain assistance from medical toxicologist or poison control centre

ANTIDOTAL TREATMENT • Administer cyanide antidote when cyanide poisoning is clinically suspected. hydroxycobalamine is the preferred antidote and is recommended for immediate therapy. (quickly complexes with cyanide, is excreted by the kidney) • If hydroxycobalamine is available , give the following: • Hydroxycoblamine 70 mg/kg up to 5 g IV(5 g is standard adult dose) • Sodium thiosulfate (25 percent): 1. 65 ml/kg up to 50 ml IV: may repeat once (maximum dose 12. 5 g) • If hydroxycoblamine is not available, cyanide toxicity is known or strongly suspected, and there are no contraindication to nitrites/give the following: • Sodium nitite 10 mg/kg-up to 300 mg- by slow IV infusion : may repeat once • Sodium thiosulfate (25 percent)1. 65 ml/kg up to 50 ml IV: may repeat once • If hydroxycobalamine is not available and cyanide toxicity is possible but not certain, or the patient has contraindications to nitrites, give the following: • Sodium thiosulfate (25 percent)1. 65 ml/kg up to 50 ml IV: may repeat once

DIFFERENTIAL DIAGNOSIS • The number one differential diagnosis is probably carbon monoxide inhalation. patients with only carbon monoxide will improve from the smoke-filled area and placed on 100% oxygen. • Seizure are common in cyanide poisoning but are rare in carbon monoxide poisoning. also of note is that carbon monoxide does not affect the pupils , but cyanide poisoning causes pupillary dilation.

COMPLICATION • Because early treatment is so important in cyanide toxicity, the most obvious pitfall would be not making the diagnosis early in the course. some complications that survivors of sever cyanide poisoning may encounter are Parkinson or other forms of neurological sequelae. the basal ganglia is particularly sensitive to cyanide toxicity

• A 54 year old women was brought to hospital from an a department fire. She had altered mental status , hypotension , and evidence of inhalational injury, but no burns, her carboxyhemoglobin level was 29% and lactate level was 16 mmol/l. she was treated with supplemental oxygen and hyperbaric oxygen for carbon monoxide intoxication • Hydroxycobalamine 5 g was administered IV in the intensive care for presumed cyanide poisoning. subsequently the pt skin and urine became bright red.


CARBON MONOXIDE POISONING Done by : Yasmeen Doumi Supervised by : Dr. Saleh Abualhaj

CLINICAL CASES • consider a mother brings her seven year old girl and five year old son to the emergency room in January with a chief complaint of viral illness the children's Mother explains that they are both complaining abset stomach nausea and headache the mother admits that she also feels unwell and thinks they may have given her a virus • think of a 23 year old man found a sleep in his car with the engine running he's breathing spontaneously and has a pulse but does not respond to commands • 40 year old woman brought to the ER by ambulance into the resuscitation day after sustaining second and third degree burns to 25% of her total body surface area after she was trapped in her burning mobile home approximately 15 minutes before Rescue
 is an odorless, tasteless, colorless, nonirritating gas")
WHAT IS CARBON MONOXIDE? Carbon monoxide (CO) is an odorless, tasteless, colorless, nonirritating gas formed by hydrocarbon combustion. The atmospheric concentration of CO is generally below 0. 001 percent, but it may be higher in urban areas or enclosed environments.
")
EPIDEMIOLOGY • Fire-related smoke inhalation is responsible for most cases of carbon monoxide (CO) poisoning. Non-fire related CO poisoning is responsible for up to 50, 000 emergency department (ED) visits • Potential sources of CO, other than fires, include poorly functioning heating systems, improperly vented fuel-burning devices (eg, charcoal grills, gasolinepowered electrical generators , and motor vehicles operating in poorly ventilated areas • Methylene chloride (dichloromethane) is an industrial solvent and a component of paint remover. Inhaled or ingested methylene chloride is metabolized to CO by the liver, causing CO toxicity in the absence of ambient CO

• Half-life: it is the time required for half the quantity of a drug • or other substance to be metabolized or eliminated. • �CO half-life on 21% room air O 2: 4 -6 hours. • �CO half-life on 100% O 2: 80 minutes. • �CO half-life with hyperbaric O 2: 22 minutes

WHO IS AT RISK? • �EVERYONE, especially: • �People using alternate heat sources during power outages • �Women who are pregnant • �People living in poorly vented crowded houses • Physical conditions that limit the body’s ability to use • oxygen • �Emphysema, asthma • �Heart disease
 diffuses rapidly across the pulmonary capillary membrane and binds")
PATHOPHYSIOLOGY • Carbon monoxide (CO) diffuses rapidly across the pulmonary capillary membrane and binds to the iron moiety of heme with approximately 240 times the affinity of oxygen. • The degree of carboxyhemoglobinemia (COHb) depends on : • 1. amounts of CO and oxygen in the environment • 2. duration of exposure • 3. minute ventilation

↑ COHb causes tissue hypoxia via the following mechanisms: • Decreased oxygen-carrying capacity of hemoglobin • Shift in the O 2 dissociation curve to the left → ↑ affinity for O 2 → ↓ release of O 2 in tissue • Binding of CO to myoglobin → cardiac ischemia → decreased cardiac output • CO inhibits mitochondrial cytochrome c oxidase → defective oxidative phosphorylation → ↑ anaerobic metabolism with ↓ ATP production and hypoxia • CO inhibits cytochrome p 450 in the brain → lipid peroxidation and leukocytemediated inflammatory damage → cerebral edema

• Once CO binds to the heme moiety of hemoglobin, an allosteric change occurs that greatly diminishes the ability of the other three oxygen binding sites to off-load oxygen to peripheral tissues This results in a deformation and leftward shift of the oxyhemoglobin dissociation curve, and compounds the impairment in tissue oxygen delivery • It binds to and inactivates cytochrome C oxidase a critical member of the electron transport chain at the interferes with oxidative phosphorylation in ATP generation

CLINICAL PRESENTATION • Nonspecific symptoms • • Headache Dizziness Fatigue Nausea/vomiting • Neurotoxicity • Altered mental status (e. g. , agitation, confusion, memory loss) • Seizures • Loss of consciousness/coma • Cardiorespiratory toxicity • • • Inhalation injury: associated with fire-related exposures Chest pain Shortness of breath Shock Respiratory failure

• Other classical signs • Cherry-red skin: after exposure to high levels (rare and usually seen postmortem) • Fundoscopic findings: bright red retinal vessels, retinal hemorrhages, papilledema (indicative of cerebral edema) • Symptoms of concurrent cyanide poisoning

CLINICAL PICTURE OF CO POISONING: Acute exposure Chronic exposur e Headache, dizziness, anorexia, apathy, General: Malaise, flu-like symptoms, insomnia, and fatigue. personality disturbance Central: Drowsiness, weakness, Polycythemia agitation, confusion, Visual and disturbance, syncope, seizures, Fecal cardiomegaly, and urinary incontinence, Memory and likely secondary gait disturbances, coma to chronic hypoxia Circulatory: Dyspnea on exertion, Chest (Penney 1988) pain, palpitations. Headache: dull, frontal, and continuous (most common) (Hampson et al 2002) Other: Nausea , vomiting , diarrhea, Abdominal pain Delayed effect DNS or delayed neurological sequalae in the form of impairment of cognitive functions.

CLINICAL SEVERITY Mild < 15 - 20% Headache Nausea, Vomiting Dizziness, Blurred vision Moderate 21 - 40% Confusion, Syncope Chest pain, Dyspnea Weakness Tachycardia, Tachypnea Rhabdomyolysis Palpitations, Dysrhythmias Hypotension Myocardial ischemia, Cardiac arrest Respiratory arrest Noncardiogenic pulmonary edema Seizures, Coma Death Severe 41 - 59% FATAL >60%

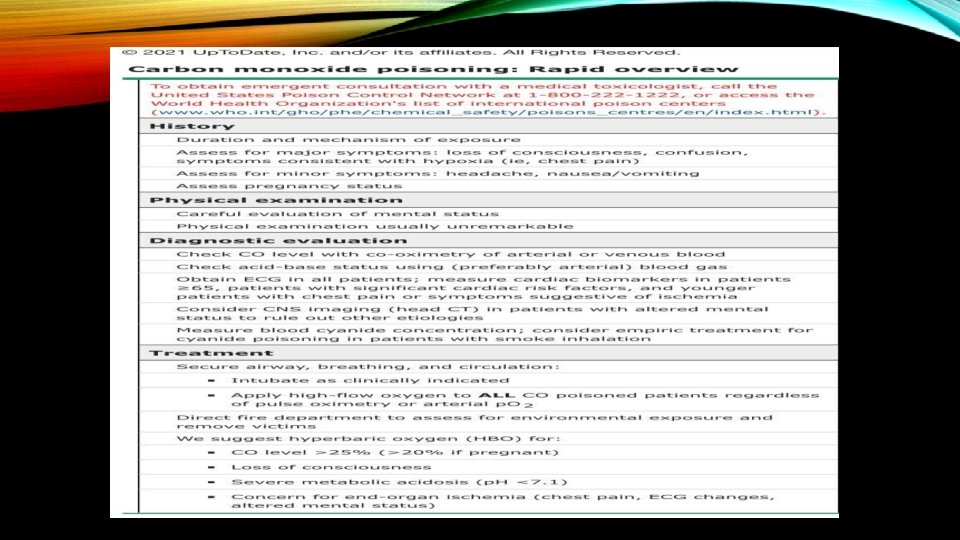
DIAGNOSIS • Ideally, all three criteria should be present to confirm acute poisoning, but symptoms vary widely and the history of exposure is not always evident. • Any symptoms of CO poisoning • Exposure to CO source • Abnormal COHb level on venous/arterial CO oximetry • > 3– 4% in nonsmokers • > 10– 15% in smokers • Start 100% oxygen immediately if clinical suspicion for CO poisoning is high! Diagnostic workup should not delay oxygen administration (see treatment).
 • CO oximetry with spectrophotometry •")
LABORATORY STUDIES • Blood gas (venous or arteria) • CO oximetry with spectrophotometry • Gold standard for diagnosis • The COHb level is used to guide therapeutic decisions. • Pa. O 2: usually appears normal • p. H: Tissue hypoxia may lead to high anion-gap metabolic acidosis.

ADDITIONAL STUDIES • Screen for affected organs and toxic coingestions. • Inhalation injury: airway examination (e. g. , direct laryngoscopy) Cardiac toxicity • All patients: ECG and cardiac monitor for 4– 6 hours • Findings may include signs of myocardial ischemia and/or arrhythmias. • Select patients : • cardiac enzymes and echocardiography • Findings may include increased troponin and/or cardiac hypomotility.

• Neurological toxicity: CT/MRI brain • Indications : • Symptomatic patients (e. g. , altered mental status) • Unconscious patients • Retinal hemorrhage (good indicator of CNS toxicity) • Findings • The globus pallidus is commonly affected (unspecific findings, usually bilateral ). • White matter changes • Cerebral edema

MANGMENT • Patients often arrive in critical condition or comatose, which requires an ABCDE approach. Oxygen therapy is considered first-line treatment. • Oxygen therapy Administer 100% oxygen immediately via nonrebreather facemask. Hyperbaric oxygen (HBOT) : • The following are considered relative indications: COHb > 25% • Pregnant women with a COHb > 20% • CO level >25 percent • Neurological manifestations (e. g. , confusion, loss of consciousness, seizures, focal neurological deficits • Severe acidosis (p. H < 7. 15) • Evidence of end-organ ischemia

MANAGEMENT OF SYSTEMIC INVOLVEMENT AND SUPPORTIVE CARE • Secure airway: Consider early intubation in patients with inhalation injury or severely impaired mental status • Evidence of cardiac toxicity (e. g. , arrhythmias, ischemia): urgent cardiology consult, continuous cardiac rhythm monitoring • Metabolic acidosis: • Improve perfusion (e. g. , fluids, oxygen). • Suspicion of concomitant cyanide poisoning • Suspicion of intentional poisoning • Evaluate for suicidal ideation • Obtain a psychiatric consultation and consider involuntary psychiatric hold.

- Slides: 60