Inflammatory Disorders of the BOWEL Ryan Murphy MD

Inflammatory Disorders of the BOWEL Ryan Murphy, MD May 15 th, 2008

Crohn’s Disease l First described in 1932 by Crohn, Ginzberg, and Oppenheimer l Idiopathic, chronic, transmural inflammatory process of the bowel l Condition is believed to be the result of an imbalance between proinflammatory and anti-inflammatory mediators

Pathophysiology l The exact cause of Crohn’s disease remains unknown l Genetic, microbial, immunologic, environmental, dietary, vascular, and even psychosocial factors as potential causative agents

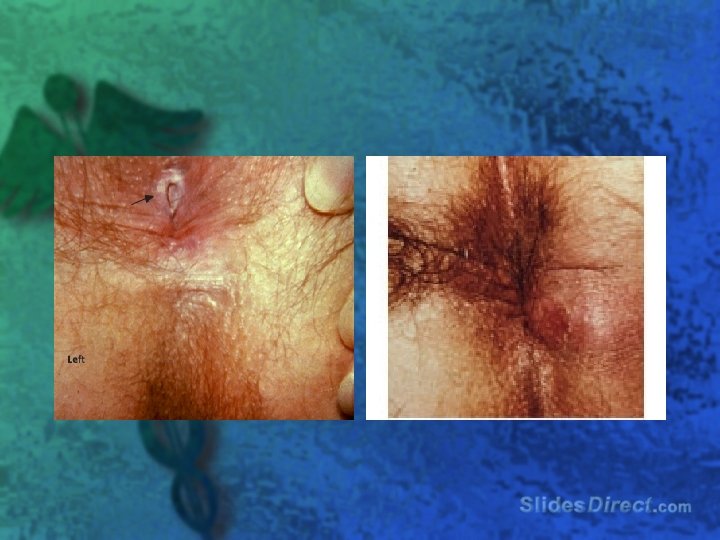
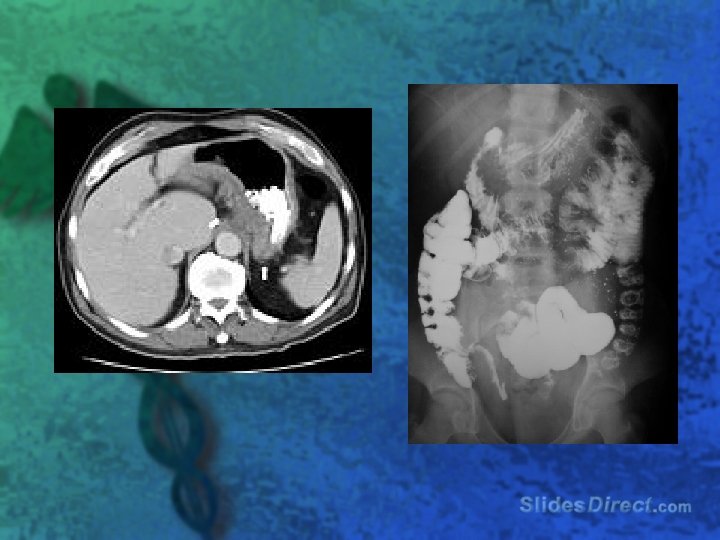
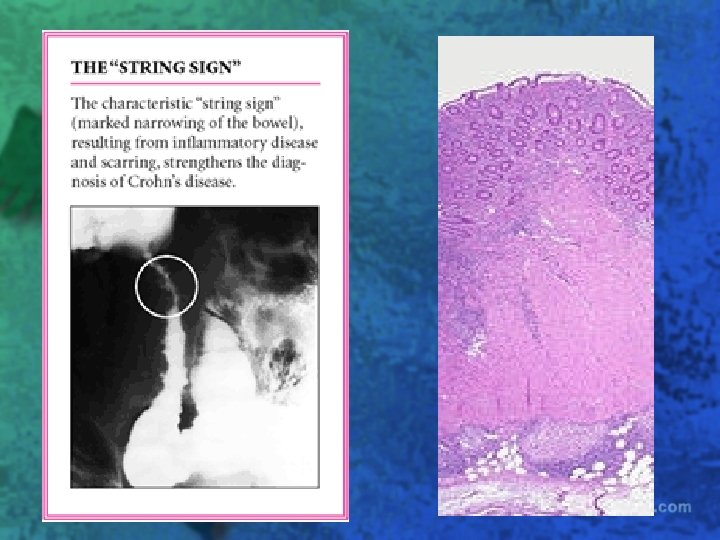
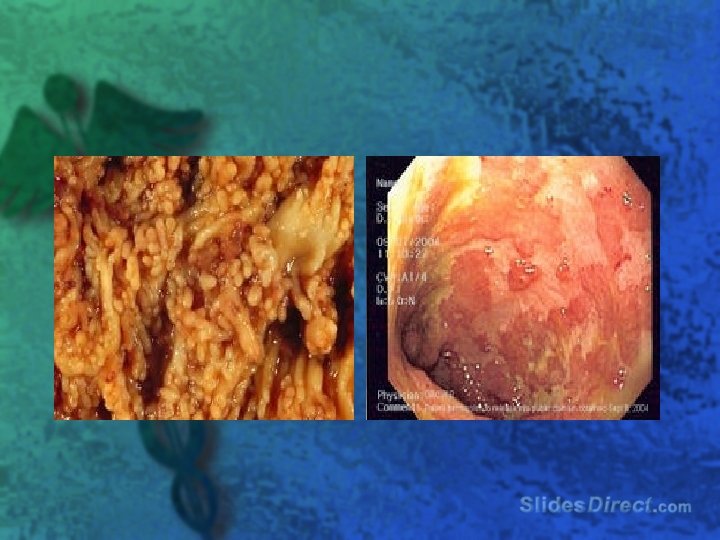
l Transmural inflammation results in thickening of the bowel wall and narrowing of the lumen l Obstruction, fistulization, perforation, abscess formation, adhesions, and malabsorption l Apporximately 30% of patients develop perianal complications

l The most common site of disease: – Ileocecal 40% – Small Bowel 30% – Colon 30% – Other 5%

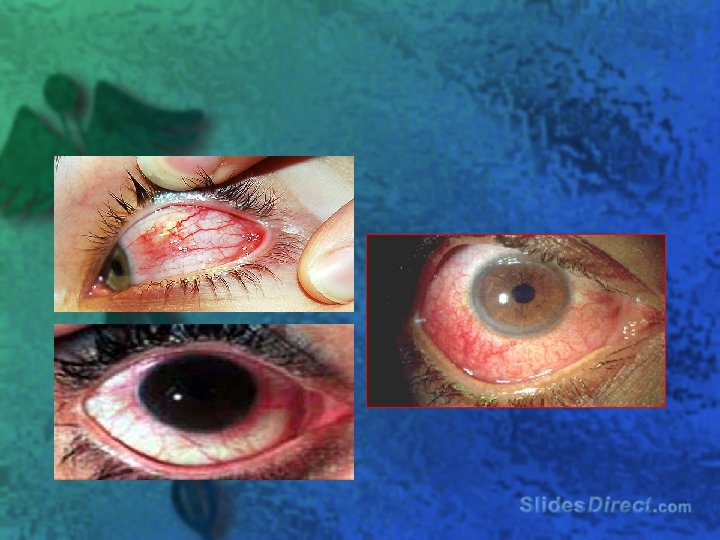
l Extraintestinal manifestations associated with Crohn’s disease : – skin, joints, mouth, eyes, liver, and bile ducts

erythema nodosum, pyoderma gangrenosum

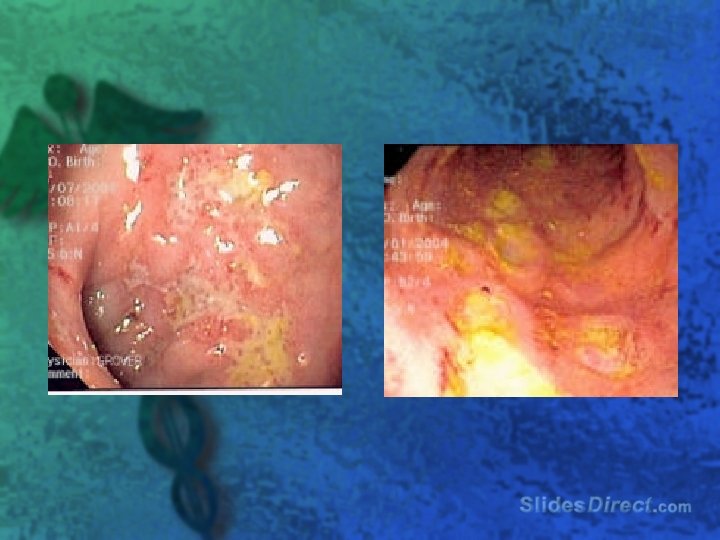
Aphthous ulcers

Who gets Crohn’s l Males are at slightly greater risk l More common among Caucasians l More prevalent among Jewish population l Bimodal Age Distribution: – First Peak – Second Peak 15 -30 60 -80

History l l l Low grade fever, night sweats, weight loss, fatigue Episodic diffuse abdominal pain, Periumbilical or RLQ pain, may be relieved with defecation Intermittent, non-bloody diarrhea Complaints suggestive of obstruction Young people commonly experience growth failure and delayed puberty

video

Physical Exam l Abdominal pain l Perianal skin tags, fistulae, abscesses, and scarring l Erythema nodosum or pyoderma gangrenosum l Uveitis or episcleritis l Peripheral arthritis

Workup l CBC l Electrolytes l Stool exam l ESR l p-ANCA l ASCA

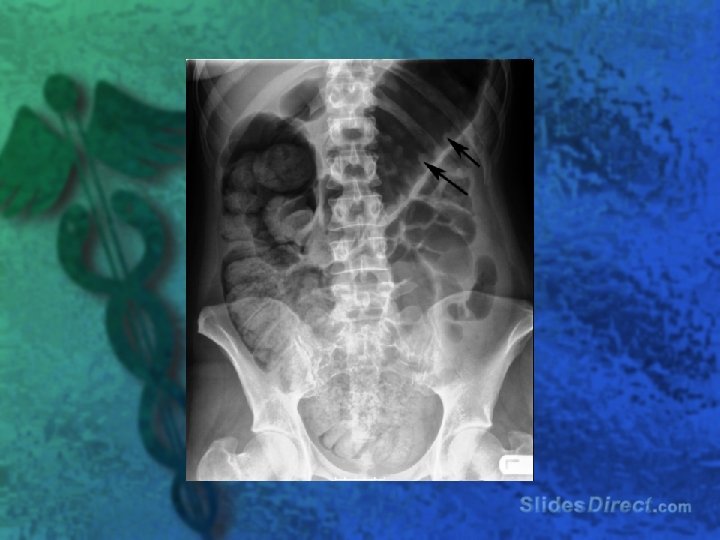
Workup l Upright chest and abdomen radiograph l Barium contrast studies l CT l MRI l Ultrasound l Colonoscopy l Radionucleotide scan

Treatment l NGT if suspected obstruction l Antidiarrheal agents loperamide or diphenoxylate with atropine l Fluid and electrolyte replacement l Sulfasalazine or mesalamine (Asacol) l Prednisone (40 -60 mg/d) l Azathioprine (2 mg/kg/d) or its active metabolite, 6 -mercaptopurine (6 -MP)

Treatment l Cipro and/or Metronidazole l If medical therapy fails, surgical resection of the inflamed bowel l Infliximab, adalimumab, certolizumab l Tacrolimus

Video

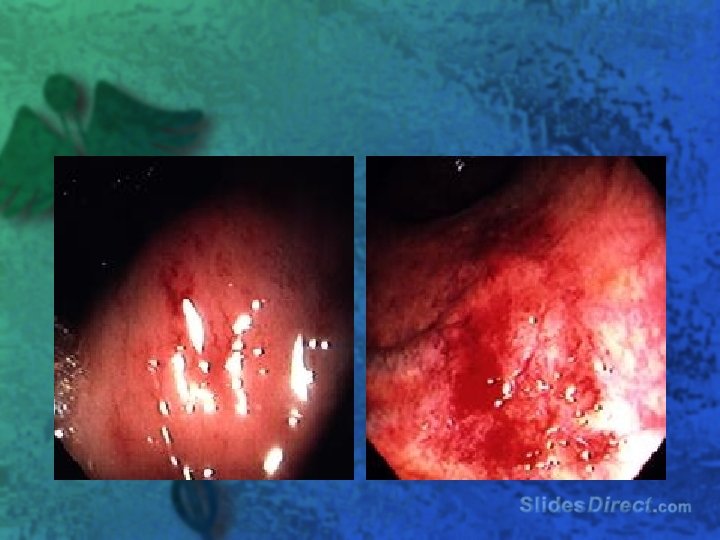
Ulcerative Colitis l chronic, recurrent inflammatory disease of the colon or rectal mucosa l defined as continuous idiopathic inflammation of the colonic or rectal mucosa l Inflammation limited to mucosa and submucosa

Ulcerative Colitis l Mucosal involvement is continuous and uniform l Always begins in rectum and spreads proximal l Chronic inflammation leads the crypt abscess, epithelial necrosis, mucosal ulceration

Ulcerative Colitis l incidence is 10 -12 cases per 100, 000 l peak incidence occurring between the ages of 15 and 25 and again around 60

Clinical Presentation l usually presents with diarrhea mixed with blood and mucus, of gradual onset l Weight loss l Abdominal pain/cramping l Urgency and tenesmus l Depends on extent and severity of disease


Extent of Involvment l Proctitis l Proctosigmoiditis l Left sided colitis l Pancolitis

Severity of Disease l Mild Disease 60% cases – – – l Severe Disease 15% cases – – – l Less than 4 BM’s / day No systemic symptoms Few Extraintestinal manifestations More than 6 BM’s / day Fever, tachycardia, weight loss, anemia Extraintestinal manifestations Fulminant Disease

Extraintestinal l l aphthous ulcers Ankylosing spondylitis Sacroiliitis Primary sclerosing cholangitis Iritis or uveitis l Erythema nodosum l Pyoderma gangrenosum l



Workup l l l l CBC Chemistry ESR / CRP LFT’s Abd x-ray CT Radionuclide scan Sigmoidoscopy / Colonoscopy

Complications l Hemorrhage l Toxic megacolon l Perforation l Obstruction l Perianal fistulas / abscesses l Carcinoma

Treatment l l l l Sulfasalazine or Mesalamine Corticosteroids 5 -ASA and steroid enemas Azathioprine, Cyclosporine, 6 -Mercaptopurine Infliximab Surgery Antibiotics

Feature Perianal Dx Abd mass Growth Failure Colon Ileum Fistulas Cancer Distribution Depth UC Absent Occasional Exclusive Never Absent Common Continuous superficial Crohn’s Common 2/3 pts Common Fairly common Skip lesions transmural
 = 100 rads serious injury usually occurs")
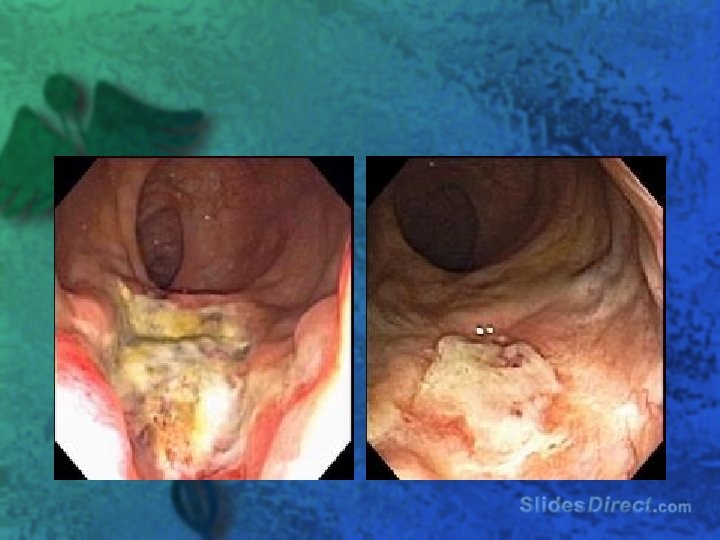
Radiation Colitis l l 1 Gy (gray) = 100 rads serious injury usually occurs at doses greater than 50 Gy 45 -65 Gy for the small intestine, 45 -60 Gy for the colon, and 55 -80 Gy for the rectum window of safety is narrow or perhaps nonexistent because the doses that cause injury are very close to the doses needed for therapy

Acute Injury l Acute injury is a function of fractionation of the dose, field size, type of radiation, and frequency of treatment l Cells are most sensitive to radiation during the G 2 and M stages of mitotic division l Acute injury is caused by injury to the mitotically active intestinal crypt cells

Chronic Injury l Chronic injury is a function of the total dose of radiation used l Chronic radiation injury is caused by injury to the less mitotically active vascular endothelial and connective tissue cells

l Incidence of 2 to 5% of patients receiving abdominal or pelvic radiotherapy

Early Presentation l l l l Patients experience acute symptoms 2 -3 weeks into the treatment. Symptoms usually resolve in 2 -6 months Anorexia Nausea - More frequent with upper abdominal radiation Vomiting - More frequent with upper abdominal radiation Abdominal cramps - Consequence usually of small intestinal involvement Diarrhea - More often observed as a consequence of pelvic irradiation Tenesmus and mucoid rectal discharge - As a result of rectal involvement Rectal bleeding - As a result of rectal involvement

Late Presentation l l l Develop months to years after therapy has ended Colicky abdominal pain - Most common late symptom, due to partial small bowel obstruction Nausea and vomiting - Consequences of small bowel obstruction Chronic watery diarrhea and/or steatorrhea Consequence of multiple factors, including malabsorption, bile acid-mediated diarrhea, bacterial overgrowth, impaired motility, and development of fistulas Feculent vaginal discharge or pneumaturia Consequence of fistula development Tenesmus, mucoid rectal discharge, rectal bleeding, constipation, and decrease in stool caliber Consequences of rectal involvement

Physical Exam l l l l Weight loss and malnutrition Generalized and conjunctival pallor Abdominal tenderness Peritoneal signs Palpable mass on abdominal examination Hyperactive bowel sounds, tinkling, rushes, and audible borborygmi Rectal tenderness and bleeding

Contributing Risk Factors l l l Previous surgery. Patients with hypertension, diabetes mellitus, and generalized atherosclerosis Thin, elderly, and female individuals may have more small intestine lying in the pelvis and may be subject to more radiation exposure. Hypoxic cells are less sensitive to radiation injury. . Certain chemotherapeutic agents (eg, Adriamycin, methotrexate, 5 -fluorouracil, bleomycin) increase sensitivity to radiation. Patients with underlying inflammatory bowel disease may be at a higher risk for severe toxicity.

Workup l CBC, Chemistry, Stool Studies for pathogens l Flat and Upright Abdominal xray l Barium Contrast l CT l Colonoscopy

Treatment l Actue – antidiarrheals, antiemetics, 5 - ASA, topical steroids, sucralfate enemas l Chronic – HBO, laser, surgery

Prevention l Dosing and location l Pretreat with barium contrast l Fill up the bladder l Body position l Antioxidants and other drugs

When you put it on paper, you commit yourself l Which of the following is true regarding inflammatory bowel disease? – A) Toxic megacolon is more common in patients – – with crohn’s than UC B) Perianal complications are most common in pts with Crohn’s C) Crohn’s dx always involves the rectum D)Erythema nodosum is most common in male pts with UC E) Anal fissures in pts with Crohn’s tend to be located in the posterior midline
")
A complaint that may differentiate pts with Crohn’s dx from IBS is: l A) Nocturnal diarrhea l B) Bloating l C) Weight Loss l D) Colicky abdominal pain l E) Bilious vomiting
 Arthralgias")
Pts with IBD may develop which of the following extraintestinal complications? l A) Arthralgias l B) Episcleritis l C) Cholelithiasis l D) Pyoderma Gangrenosum l E) All of the above

Which of the following is true regarding exacerbations and complications of IBS? l l l A) Pts with mild to moderate exacerbations can be sent home with a resumption of therapy or with outpt corticosteroids. B) Bowel rest has not been shown to be useful in pts with flares of IBD C) Fistulae are initially treated medically D) Initial treatment for toxic megacolon is fluids, antibiotics, and corticosteroids E) All of the above
 Has a mortality rate of 75% in its")
Radiation enteritis… l l l A) Has a mortality rate of 75% in its acute form. B) Presents most commonly in its chronic form. C) Occurs more than 2 yrs after completion of therapy in 10% of pts D) Is best diagnosed with abd/pelvis CT with oral and IV contrast. E) All of the above.
- Slides: 61