Inflammatory Bowel Disease IBD The large intestine or


Inflammatory Bowel Disease IBD

The large intestine, or the large bowel, is the last part of the gastrointestinal tract • The colon is much wider than the small intestine, but is also much shorter • The large intestine is about 5 feet (1. 5 m) in length and 2. 5 inches (6 -7 cm) in diameter • Divided into: � the ascending colon (including the cecum and appendix) � Cecum ( first part of large intestine ) � Appendix ( accumulation of lymphatic tissue ) � the transverse colon � the sigmoid colon � the descending colon � Rectum � Anal canal

n Typhoid fever spreads through contaminated food and water or through close contact with someone who's infected Pathogenesis n S typhi and paratyphi enter the host's system primarily through the distal ileum

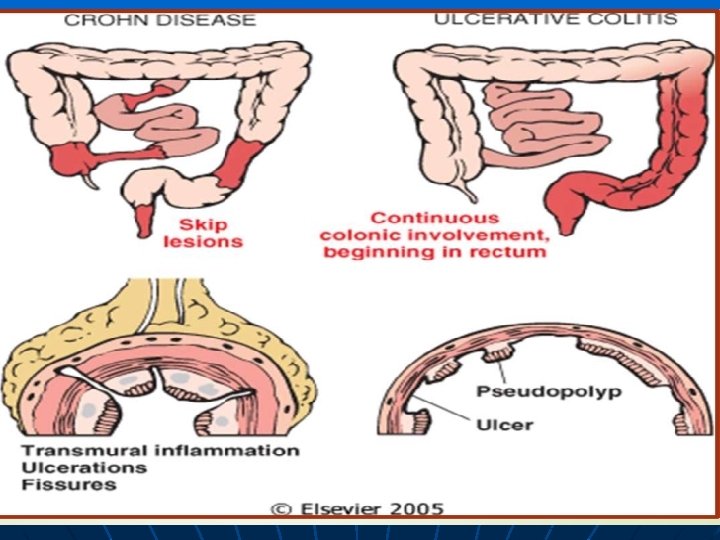
Definition: A group of chronic intestinal diseases characterized by inflammation of the bowel. The most common types are ulcerative colitis and Crohn’s disease. n Ulcerative colitis: is an inflammatory bowel disease that cause long-lasting inflammation and sores (ulcers) in the innermost (superficial) lining of the large intestine (colon) and or rectum. n n Crohn's disease: is an inflammation of the lining of digestive tract. In Crohn's disease, inflammation often spreads deep ( trans mural) into affected tissues. The inflammation can involve different areas of the digestive tract, The large intestine, small intestine or both

Clinical manifestations of IBD the manifestations of IBD depend on the area of the intestinal tract involved. The symptoms, however, are not specific for this disease. They are as follows: n Abdominal cramping n Irregular bowel habits, passage of mucus without blood or pus n Weight loss, Fever, sweats , Malaise, fatigue n Arthralgias n Growth retardation and delayed or failed sexual maturation in children n Extraintestinal manifestations (10%-20%): Arthritis, uveitis, or liver disease

n n Grossly bloody stools, occasionally with tenesmus: Typical of UC, less common in CD Perianal disease (eg, fistulas, abscesses): Fifty percent of patients with CD n So, in UC n IN CD: diarrhea, malabsorption, pain, anaemia, perianal disease mainly: bloody diarrhea, crampy pain, tenesmus , passage of mucus anaemia Symptoms suugesting occurrence of malignancy(rapid deterioration , marked wt loss

n n Ulcerative colitis: It is a ulcero inflammatory disease affecting the colon, which is limited to the mucosa , submucosa It begins in the rectum and extends proximally in a continuous fashion The disease arise at any age, with peak at 20 , specially in young adolescents and may occur in children Ulcerative colitis involves the rectum and sigmoid and may involve the colon. With severe active disease, there is extensive and broad-based ulceration of the mucosa Crohn’s disease This disease may affect any level of the alimentary tract n It most commonly located at the terminal ileum n It occurs at any age but the peak age of detection is the second and third decades of life n There is involvement of the small intestine alone in 30% of cases, of small intestine and colon in 40%, and of the colon alone in 30% n Sharply defined transmural involvement of the bowel by an inflammatory process with mucosa damage n Fissuring with formation of fistula n

n n n TREATMENT: MEDICAL, SURGICAL

Anti-inflammatory drugs n Anti-inflammatory drugs are often the first step in the treatment of inflammatory bowel disease: Aminosalicylates Corticosteroids for short course with rapid tapering n Immune system modulators ( suppressors): These drugs also reduce inflammation, but they target immune system rather than directly treating inflammation. Instead, they suppress the immune response that releases inflammationinducing chemicals the intestinal lining. For some people, a combination of these drugs works better than one drug alone: � Azathioprine and 6 -mercaptopurine �biological therapy: Anti TNF alpha, anti interleukins

Antibiotics n People with ulcerative colitis who run fevers will likely be given antibiotics to help prevent or control infection. Antibiotics can reduce the amount of drainage and sometimes heal fistulas abscesses in people with Crohn's disease: Metronidazole and Ciprofloxacin

Surgical treatment Surgery for Crohn's disease n Surgery can often eliminate ulcerative colitis, During surgery, the doctor removes a damaged portion of the digestive n removing entire colon and tract and then reconnects the rectum healthy sections. n (proctocolectomy). Surgery may also be used to In most cases, this involves a n close fistulae and procedure called ileoanal anastomosis that eliminates the n drain abscesses. need to wear a bag to collect stool. A common procedure for Crohn's Indications: ( severe refractory UC, disease is Malignancy, toxic megacolon) n strictureplasty, n which widens a segment of the intestine that has become too narrow

Infectious Diarrhea

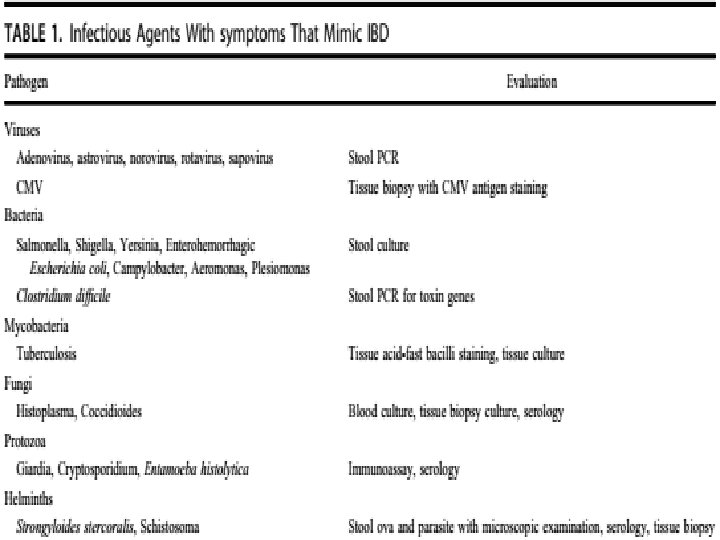
Infectious diarrhea which mimics clinical picture of IBD: 1 - bacterial: salmonella, shigella, E coli, Combylobacter jejuni, Yersinia and C. difficile 2 - Mycobacterial: TB 3 - viral: noro, norwalk, rota viruses and CMV colitis 4 - parasitic: amoebae 5 - sexually induced lymphogranuloma venereum proctocolitis: syphilis,

Clinical picture: 1 - may be similar 2 - Treatment is totally different

Salmonellae : may cause food-borne outbreaks, often in summer and fall. The child experiences abdominal cramps and nausea after an incubation period of 8 -48 hours following ingestion of a contaminated source (food or water). The stools are watery and may contain blood. Fever is noted in most children

Campylobacter enteritis: is characterized by the abrupt onset of fever and abdominal pain, shortly followed by diarrhea. Temperature often remains normal in children younger than 3 month Vomiting is uncommon The stools are watery and occur 2 -20 times daily; they contain blood in 50 -95% of cases. Infection is acquired through ingestion of raw meat, poultry, fish, and water. .

n Yersinia enterocolitica: infection presents with the abrupt onset of watery diarrhea that may contain blood. Most of the patients experience severe abdominal pain, which may be mistaken for appendicitis. Older children have a febrile response, with temperatures ranging from 99° to 104°F. Joint pain secondary to arthritis and rashes occur in 5 -10% of patients with yersiniosis

n Shigellae: may cause asymptomatic infection, mild gastroenteritis, or bacillary dysentery. Bacillary dysentery begins suddenly with fever and abdominal pain, and diarrhea begins shortly thereafter. In severe cases, Shigella infection may lead to megacolon or colonic perforation n Less commonly, extraintestinal manifestations may occur and include hemolytic uremic syndrome, reactive arthritis, neutropenia, sepsis, pneumonia, seizures, and encephalopathy (especially with Shigella dysenteriae type 1 species) n Stools are frequent (10 -12/day, on average) and contain mucus and blood; tenesmus is common. Fever is noted, often in the range of 102104°F (39 -40°C)

Enterohemorrhagic Escherichia coli: n Enterohemorrhagic E. coli infection, which can occur with both O 157 and non-O 157 strains, often leads to bloody diarrhea and abdominal pain and is a significant risk factor for the development of hemolytic uremic syndrome, which occurs in approximately 10% of young children and up to 8% of adults n Other strains: may rise to diarrhea n Enteropatogenic E coli n Enteroaggregative E coli n Enterotoxogenic E coli n Enteroinvasive E coli

Clostridium difficile: pseudo membranous colitis n Spore forming organism produce two orms of toxins( A and B) which induce epithelial necrosis and induction of fluid secretion and severe inflammation forming pseudo membrane n Risk Factors : n Old ages, multiple antibiotic use, immunosuppresed , co morbid disease, long hospital stay

n Tuberculosis n tuberculous infection has been well described in multiple extrapulmonary locations including the GI tract. Gastrointestinal TB is often not associated with pulmonary TB. Both gastrointestinal TB and CD are chronic granulomatous diseases with overlapping symptoms Gastrointestinal TB is associated with fever and weight loss and can lead to mucosal ulcerations in the small bowel, particularly the terminal ileum, with diarrhea and hematochezia. n TB causes caseating granulomas, in contrast to the noncaseating granulomas associated with CD.

n CMV colitis: Risk factors for CMV infection include n age greater than 30 years, refractory IBD, and immunosuppression. attempt at tissue diagnosis via lower endoscopy wit biopsies to evaluate for both viral inclusions( OWL eye inclusion ) and the presenc of CMV antigen with immunohistochemistry or PCR is important. Because almost one-third of patients with IBD may have positive biopsies from only the right colon, full colonoscopy with both right and left colon biopsies is preferable when able to be performed safely.

Thank you
- Slides: 26