Inflammatory Bowel Disease IBD n n n Chronic
 n n n Chronic condition resulting from inappropriate")
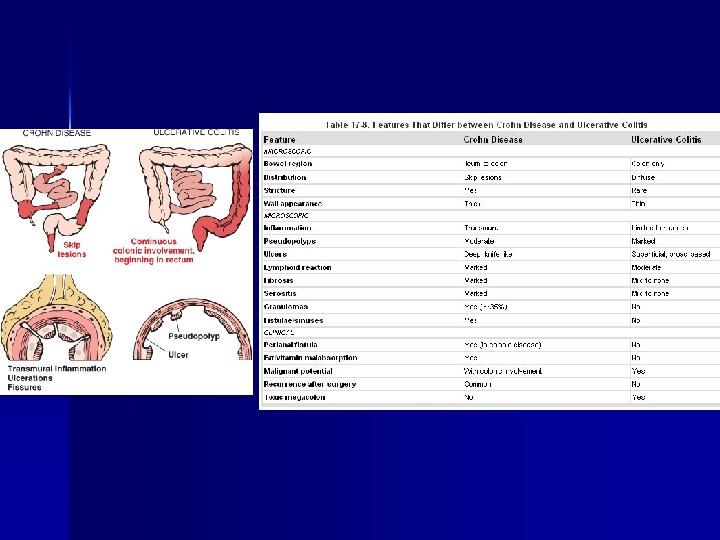
Inflammatory Bowel Disease (IBD, 염증성 장질환) n n n Chronic condition resulting from inappropriate mucosal immune activation Distinction: distribution of affected sites and morphologic expression of disease – Ulcerative colitis (궤양대장염): severe ulcerating inflammatory disease that is limited to the colon and rectum and extends only into the mucosa and submucosa – Crohn disease (크론병): involve any area GI tract (frequent ileal involvement, regional ileitis) and is typically transmural The distinction between UC and CD is important. – Different surgical and medical therapy – Higher risk of cancer in UC Female preponderance, frequently in the teens and early 20 s Hygiene hypothesis
-1. 23 (1990’s) /100. 000 CD 0. 1 (1988)-1. 5")
In Korea UC 0. 2(1980’s)-1. 23 (1990’s) /100. 000 CD 0. 1 (1988)-1. 5 (2001) /100, 000 Inflamm Bowel Dis 2001; 7: 260

Pathogenesis n n n Idiopathic disorder Result from a combination of defects in host interactions with intestinal microbiota, intestinal epithelial dysfunction, and aberrant mucosal immune response The current premise is that defects in the innate immune system allow bacteria to invade the mucosa of the gut, resulting in an exaggerated adaptive immune response, which leads to extensive bowel damage.

Genetics n n n 15% of IBD patients have affected first-degree relatives. Monozygotic twins: 50% concordance rate for CD and 16% of UC NOD 2 (nucleotide-binding oligomerization domain) – NOD 2 polymorphism confer 4 -fold increase in CD – Bind to intracellularbacterial peptidoglycan and subsequently activate NF-κB (nuclear factor) pathway, a transcription factor involved in cellular inflammatory responses and macrophage apoptosis – NOD 2 may regulate immune responses to prevent excessive activation by luminal microbes – Less than 10% of individuals carrying NOD 2 mutation develop CD – Uncommon in African and Asian CD patients ATG 1 L 1 (autophagy-related 16 -like) IRGM (immunity-related GTPase M)

n n n Mucosal immune response – Immunosuppression remains the mainstay of IBD therapy. Epithelial defects – Barrier dysfunction is associated with NOD 2 polymorphism in CD – Mutation of the organic cation transporter SLC 22 A 4 in CD – Polymorphism in ECM 1 with UC Microbiota The role of intestinal microbiota, epithelial function, and mucosal immunity suggests a cycle by which transepithelial flux of luminal bacterial components activates innate and adaptive immune responses. In a genetically susceptible host, the subsequent release of TNF and other immune-mediated signals direct epithelia to increase tight junction permeability, which causes further increases in the flux of luminal materials. These events may establish a self amplifying cycle in which a stimulus at any site may be sufficient to initiate IBD.

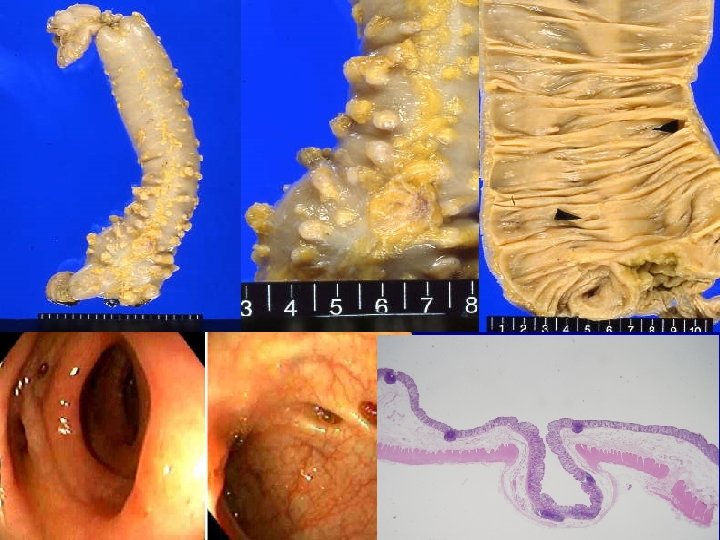
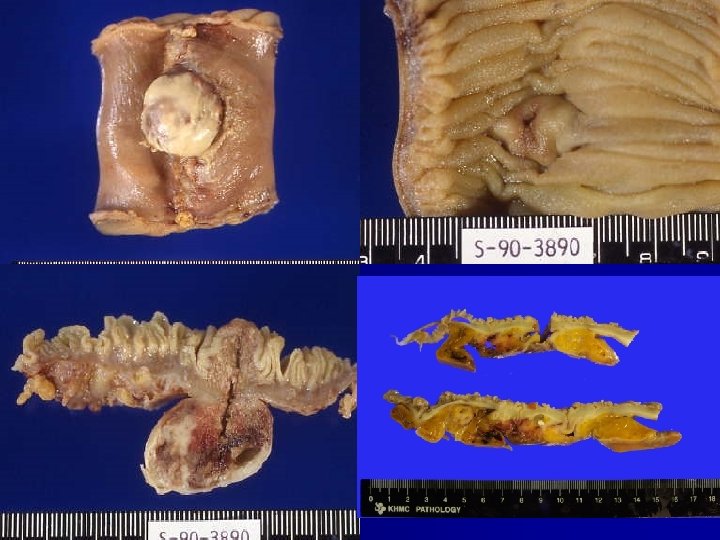
Crohn Disease

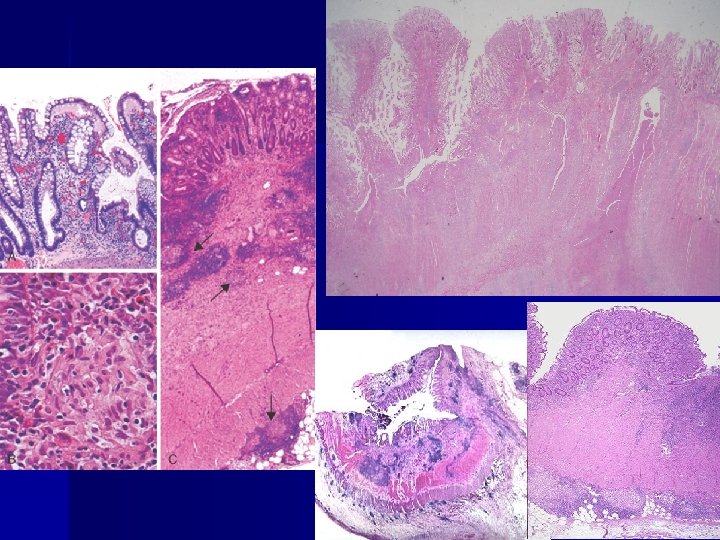
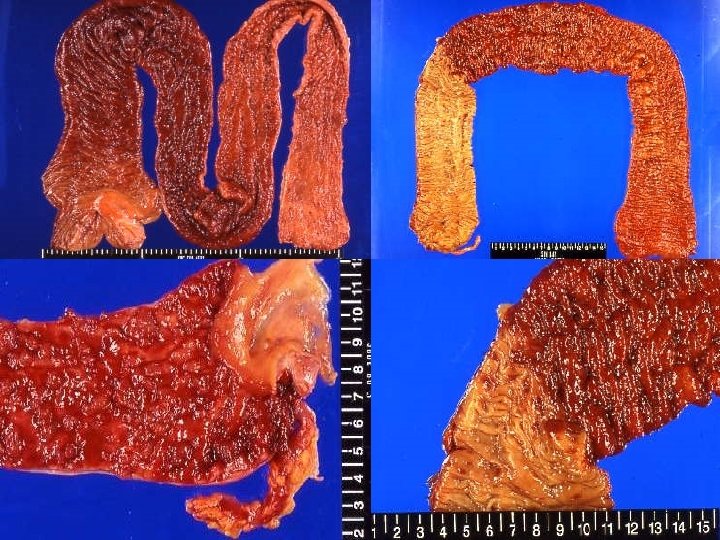
Cobblestone appearance skip lesion Fistula tram-track ulceration

aphthous ulcer Creeping fat

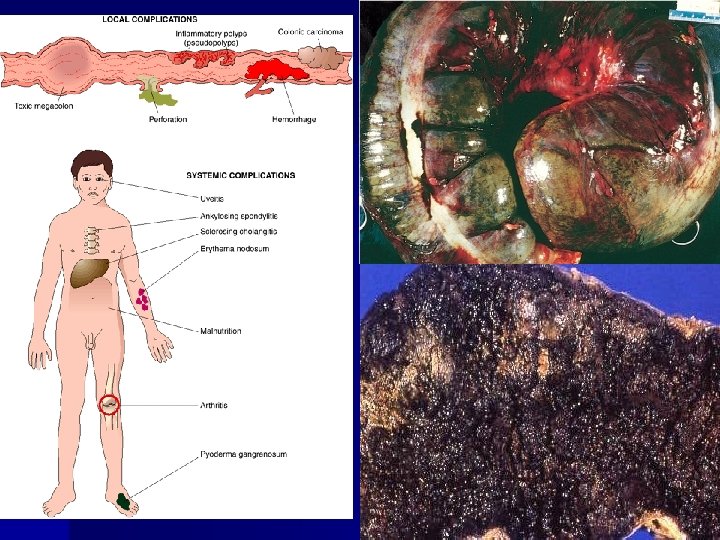
Clinical Features n n n Usually begins with intermittent attacks of relatively mild diarrhea, fever, and abdominal pain, spaced by asymptomatic periods lasting for weeks to many months Bouts of diarrhea with fluid and electrolyte losses, weight loss, and weakness Complications: fibrosing stricture, fistula, protein-losing enteropathy, generalized malabsorption, pernicious anemia, steatorrhea Extraintestinal manifestations: migratory polyarthritis, sacroiliitis, ankylosing spondylitis, erythema nodosum, uveitis Increased incidence of cancer of the GI tract (5 -6 times)

Treatment n n n No cure is available. Conventional immunosuppressive drugs: corticosteroids, sulfasalazine, metronidazole, 6 -mercaptourine, cyclosporine Biologic agents: Infliximab (a chimeric humanized anti. TNF-α antibody), adalimumab, (fully human monoclonal antibody anti-TNF-α), natalizumab (humanized Ig. G 4 monoclonal antibody) Surgery: obstruction or fistula with abscess Preanastomotic or prestomal recurrences after construction of an enterostomy is frequent. The need for repeated resections can lead to short-bowel syndrome.

2005. 05 2006. 03 2009. 06

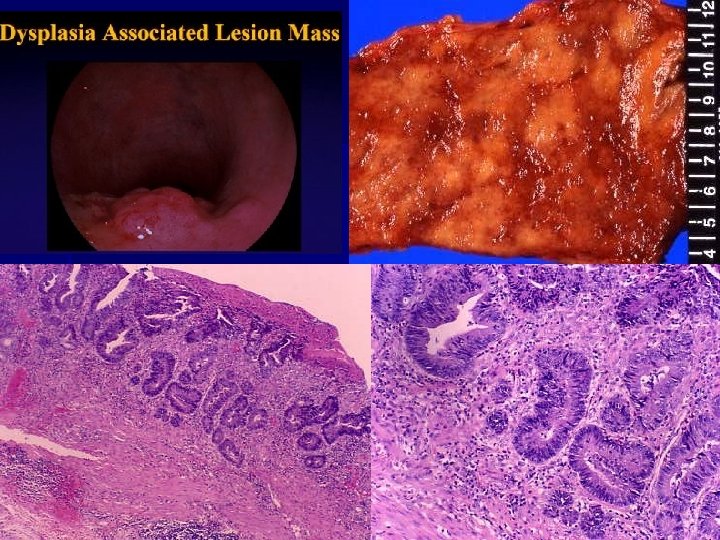
Ulcerative Colitis n n n n Ulceroinflammatory disease limited to the colon and affecting only the mucosa and submucosa Extend in a continuous fashion proximally from the rectum Associated with arthritis (25%), uveitis, erythema nodosum and pyoderma gangranosum (10%), primary sclerosing cholangitis (4%) Whites > Blacks, female>male Peak age: 20 -35 years, 50 -60 years Dysplasia (low to high) and the progression to frank carcinoma High-grade epithelial dysplasia is a strong indication for colectomy. Operation: total proctocolectomy with ileal pouch anal anastomosis

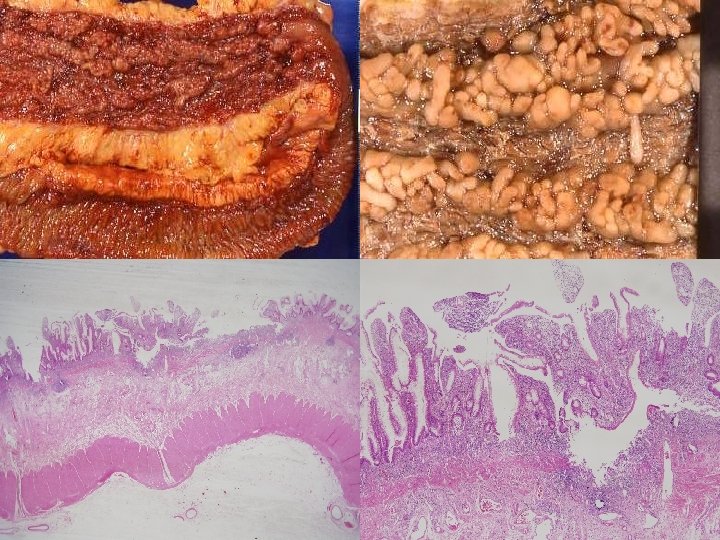
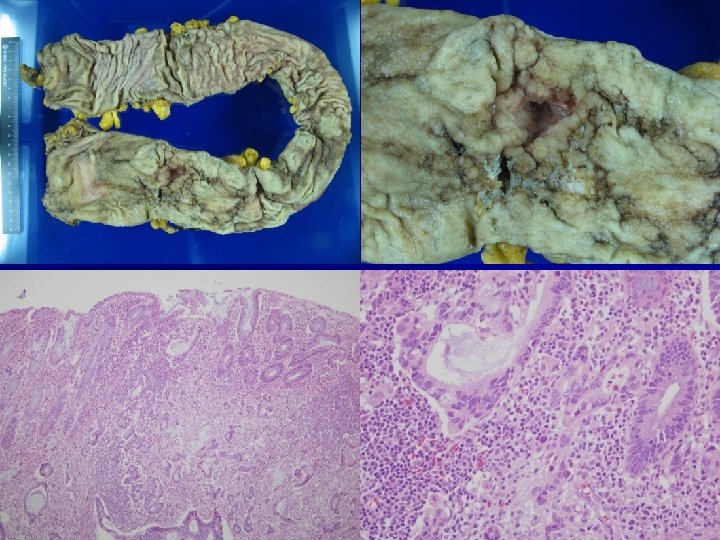
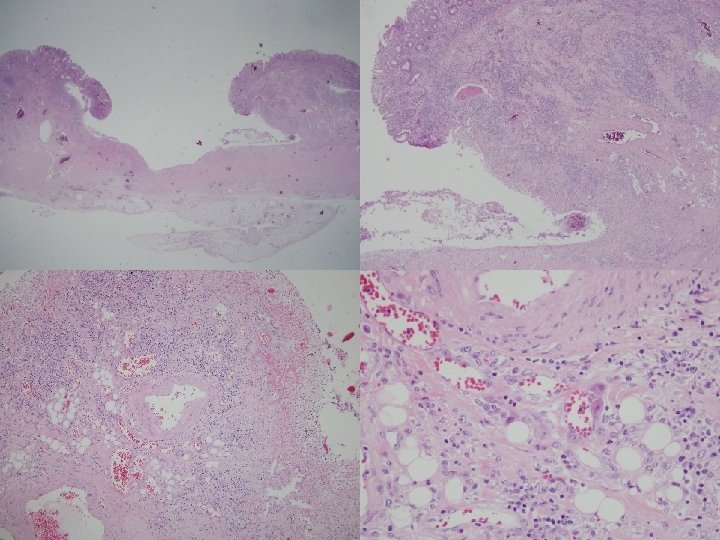
Histology n n n Early colitis – Mucosal congestion, edema, hemorrhage – Diffuse chronic inflammatory cells infiltrate in the lamina propria – Damage and distortion of crypts, crypt abscess Progressive colitis – Atrophic, distorted crypts, inflammatory pseudopolyps Advanced colitis: mucosal atrophy with chronic inflammation Backwash ileitis: distal ileal inflammation (10%) Toxic megacolon: progressive swelling and gangraneous colon

Distorted architecture Cryptcryptal distortion Crypt abscesses Irregular cryptal branching Cryptal herniation and rupture

Clinical Features n n n Typically presents as a relapsing disorder marked by attacks of bloody mucoid diarrhea that may persist for days, weeks, or months and then subside, only to recur after an asymptomatic interval of months to years or even decades Accompanied by lower abdominal pain and cramps usually relieved by defecation Medical treatment: 5 -aminosalicylate-based compounds, corticosteroid, immunosuppressive drug The most feared long-term complication is cancer. The risk of cancer is highest in patients with pancolitis of 10 or more years’ duration, in whom it is 20 -30 -fold higher than in a control group. The associated carcinomas are often infiltrative without obvious exophytic masses.

Indeterminated colitis n n n 10%: extensive pathologic and clinical overlap between UC and CD Do not involve the SI and have colonic disease in a continuous pattern Patchy histologic disease, fissues, a family history of CD, perianal lesions, onset after initiating use of cigarettes Perinuclear anti-neutrophil cytoplasmic antibody: 75% UC, 11% CD Ab to Saccharomyces cerevisae: UC(-), CD(often, +)

Colitis-asscoaited neoplasia n n n Risk increase sharply 8 to 10 years after disease initiation. Patient with pancolitis are at greater risk than those with only left-sided disease. Greater frequency and severity of active inflammation may increase risk. Patient with primary sclerosing cholangitis have an even greater risk of dysplasia. In many cases dysplasia occurs in flat areas of mucosa that are not grossly recognized as abnormal. High grade dysplasia typically prompts colectomy.
 n n n Blind pouch leading off the alimentary tract, lined")
Diverticular Disease (게실질환) n n n Blind pouch leading off the alimentary tract, lined by mucosa that communicates with the lumen of the gut Acquired and lack or have an attenuated of muscle M/C site: left side of colon (sigmoid) Old age, generally multiple (diverticulosis) Pathogenesis: focal weakness in the colonic wall and increased intraluminal pressure – Diets low in fiber reduce stool bulk, which in turn leads to increased peristaltic activity, particularly in the sigmoid colon – Diverticulitis presumably results from irritation caused by retained fecal materials (10 -20%). Mostly asymptomatic, pain and discomfort (20%)
- Slides: 28