Inflammatory bowel disease IBD G SADASIVA RAO M
 G SADASIVA RAO M. Pharm, (Ph. D) Asst. Professor &")
Inflammatory bowel disease (IBD) G SADASIVA RAO M. Pharm, (Ph. D) Asst. Professor & HOD Dept. of Pharmacy Practice, Hindu college of pharmacy, Guntur, AP.
 involves chronic inflammation of all or part of")
Definition • Inflammatory bowel disease (IBD) involves chronic inflammation of all or part of your digestive tract. • IBD primarily includes Ulcerative colitis and Crohn's disease. • Both usually involve severe diarrhea, pain, fatigue and weight loss. • IBD can be debilitating and sometimes leads to lifethreatening complications.

• Ulcerative colitis is an inflammatory bowel disease that causes long-lasting inflammation and sores (ulcers) in the innermost lining of your large intestine (colon) and rectum.

• Ulcerative colitis is classified according to the location of inflammation and severity of symptoms: • Ulcerative proctitis. Inflammation is confined to the area closest to the anus (rectum), and rectal bleeding may be the only sign of the disease. This form of ulcerative colitis tends to be the mildest. • Proctosigmoiditis. Inflammation involves the rectum and sigmoid colon (lower end of the colon). Signs and symptoms include bloody diarrhea, abdominal cramps and pain, and an inability to move the bowels (tenesmus).

• Left-sided colitis. Inflammation extends from the rectum up through the sigmoid and descending colon. Signs and symptoms include bloody diarrhea, abdominal cramping and pain on the left side, and unintended weight loss. • Pancolitis often affects the entire colon and causes abouts of bloody diarrhea that may be severe, abdominal cramps and pain, fatigue, and significant weight loss. • Acute severe ulcerative colitis. Previously called fulminant colitis, this rare form of colitis affects the entire colon and causes severe pain, profuse diarrhea, bleeding, fever and inability to eat.

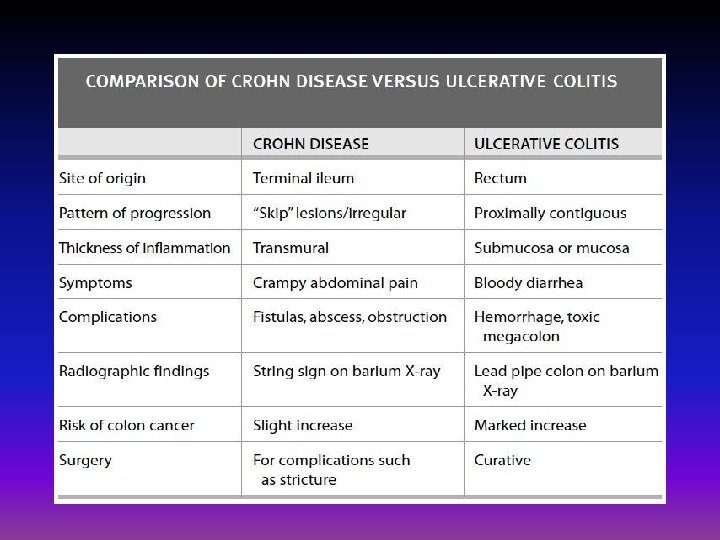
• Crohn's disease is a condition of chronic inflammation potentially involving any location of the GIT from mouth to anus. • In Crohn's disease, inflammation often spreads deep into affected tissues

• Crohn's disease may involve inflammation in different parts of the digestive tract in different people. • The most common areas affected are the last part of the small intestine (ileum) and the colon. • Inflammation may be confined to the bowel wall, which can lead to narrowing from inflammation or scarring or both (fibrostenosis), or may tunnel through the bowel wall (fistula). Narrowing may lead to a blockage (obstruction). Obstructions, stenosis and fistulas are not associated with ulcerative colitis
 • Others")
Less common entities of IBD are: • Microscopic colitis (collagenous and lynphocytic) • Others – Diversion colitis – Radiation colitis – Drug induced colitis – Infectious colitis – Ischemic colitis

Symptoms Signs and symptoms that are common to both Crohn's disease and ulcerative colitis include: • Diarrhea: Diarrhea is a common problem for people with IBD. • Fever and fatigue: Many people with IBD experience a low-grade fever. You may also feel tired or have low energy. • Abdominal pain and cramping: Inflammation and ulceration can affect the normal movement of contents through your digestive tract and may lead to pain and cramping. You may also experience nausea and vomiting.

• Blood in your stool: You might notice bright red blood in the toilet bowl or darker blood mixed with your stool. You can also have bleeding you don't see (occult blood). • Reduced appetite: Abdominal pain and cramping, as well as inflammation, can affect your appetite. • Unintended weight loss: You may lose weight and even become malnourished because you cannot properly digest and absorb food.

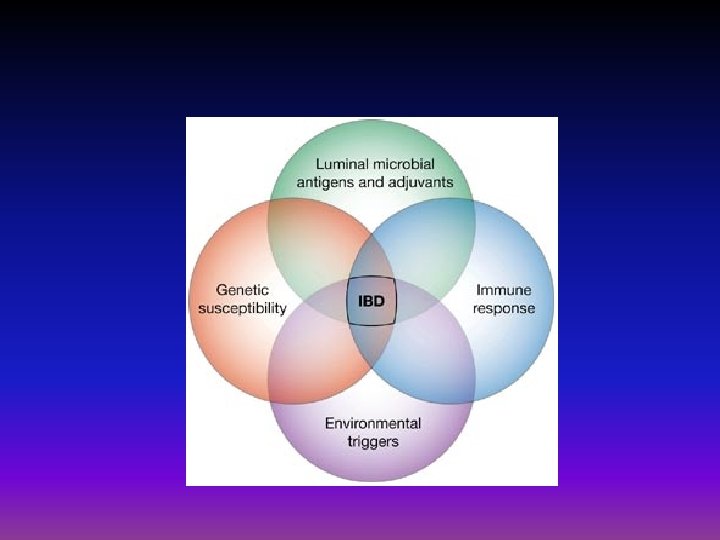
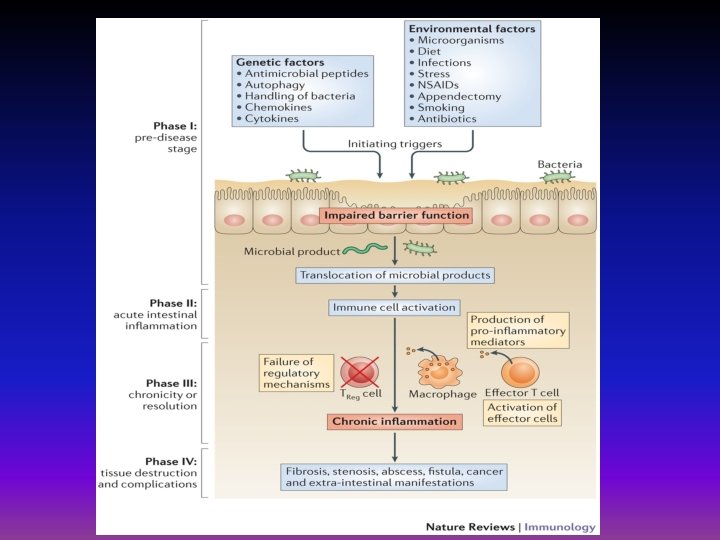
Causes • The exact cause of inflammatory bowel disease remains unknown. • Previously, diet and stress were suspected, but now doctors know that these factors may aggravate but don't cause IBD. • One possible cause is an immune system malfunction. an abnormal immune response causes the immune system to attack the cells in the digestive tract, too. • Heredity also seems to play a role in that IBD is more common in people who have family members with the disease.

Risk factors • Age: Most people who develop IBD are diagnosed before they're 30 years old. But some people don't develop the disease until their 50 s or 60 s. • Race or ethnicity: Although whites have the highest risk of the disease, it can occur in any race. If you're of Ashkenazi Jewish descent, your risk is even higher. • Family history: You're at higher risk if you have a close relative — such as a parent, sibling or child — with the disease. • Cigarette smoking: It is the most important controllable risk factor for developing Crohn's disease. However, smoking may provide some protection against ulcerative colitis.
 is a medication sometimes")
• Isotretinoin use: Isotretinoin (Amnesteem, Claravis, Sotret; formerly Accutane) is a medication sometimes used to treat scarring cystic acne or acne. Some studies suggest it may be a risk factor for IBD, but a clear association between IBD and isotretinoin has not been established. • Nonsteroidal anti-inflammatory medications: These include ibuprofen, naproxen sodium, diclofenac sodium and others. These medications may increase the risk of developing IBD or worsen disease in people who have IBD. • Where you live: If you live in an urban area or in an industrialized country, you're more likely to develop IBD. Therefore, it may be that environmental factors, including a diet high in fat or refined foods, play a role. People living in northern climates also seem to be at greater risk.

Complications • Crohn's disease may lead to one or more of the following complications: • Inflammation: Inflammation may be confined to the bowel wall, which can lead to diarrhea and bleeding. Inflammation can also lead to scarring and narrowing (stenosis) or may spread through the bowel wall (fistula). • Bowel obstruction: Crohn's disease affects the full thickness of the intestinal wall. Over time, parts of the bowel can thicken and narrow, which may block the flow of digestive contents. You may require surgery to remove the diseased portion of your bowel. • Ulcers: Chronic inflammation can lead to open sores (ulcers) anywhere in your digestive tract, including your mouth and anus, and in the genital area (perineum).

• Fistulas: Sometimes ulcers can extend completely through the intestinal wall, creating a fistula — an abnormal connection between different body parts. Fistulas can develop between your intestine and skin or between your intestine and another organ. Fistulas near or around the anal area (perianal) are the most common kind. • Anal fissure: This is a small tear in the tissue that lines the anus or in the skin around the anus where infections can occur. It's often associated with painful bowel movements and may lead to a perianal fistula.

• Malnutrition: Diarrhea, abdominal pain and cramping may make it difficult for you to eat or for your intestine to absorb enough nutrients to keep you nourished. It's also common to develop anemia due to low iron or vitamin B 12 caused by the disease. • Colon cancer: Having Crohn's disease that affects your colon increases your risk of colon cancer. General colon cancer screening guidelines for people without Crohn's disease call for a colonoscopy every 10 years beginning at age 50. However, depending on how long you have had Crohn's disease and how much of your colon is involved, you may need a colonoscopy as often as every one to two years. Ask your doctor how often you should have a colonoscopy.

• Other health problems: Crohn's disease can cause problems in other parts of the body, such as inflammation of the eyes, skin or joints; anemia; osteoporosis; inflammation of the liver or bile ducts; and delayed growth or sexual development in children. • Medications: Certain medications for Crohn's disease that act by blocking functions of the immune system are associated with a small risk of developing cancers such as lymphoma and skin cancers. They also increase risk of infection. • Corticosteroids can be associated with a risk of osteoporosis, bone fractures, cataracts, glaucoma, diabetes and high blood pressure. Work with your doctor to determine risks and benefits of medications

• • • Possible complications of ulcerative colitis include: Severe bleeding A hole in the colon (perforated colon) Severe dehydration Liver disease (rare) Bone loss (osteoporosis) Inflammation of your skin, joints and eyes Sores in the lining of your mouth An increased risk of colon cancer A rapidly swelling colon (toxic megacolon) Increased risk of blood clots in veins and arteries

Tests and diagnosis Diagnosis of IBD, you may have one or more of the following tests and procedures: • Blood tests • Tests for anemia or infection. Your doctor may suggest blood tests to check for anemia — a condition in which there aren't enough red blood cells to carry adequate oxygen to your tissues — or to check for signs of infection from bacteria or viruses. • Fecal occult blood test. You may need to provide a stool sample so that your doctor can test for hidden blood in your stool.

Endoscopic procedures • Colonoscopy: This test allows your doctor to view your entire colon using a thin, flexible, lighted tube with an attached camera. During the procedure, your doctor can also take small samples of tissue (biopsy) for laboratory analysis, which may help confirm a diagnosis. Clusters of inflammatory cells called granulomas, if present, help confirm a diagnosis of Crohn's disease. • Flexible sigmoidoscopy: In this procedure, your doctor uses a slender, flexible, lighted tube to examine the last section of your colon (sigmoid).

• Upper endoscopy: In this procedure, your doctor uses a slender, flexible, lighted tube to examine the esophagus, stomach and first part of the small intestine (duodenum). While it is rare for these areas to be involved with Crohn's disease, this test may be recommended if you are having nausea and vomiting, difficulty eating or upper abdominal pain. • Capsule endoscopy: This test is used to help diagnose Crohn's disease. You swallow a capsule that has a camera in it. The images are transmitted to a computer you wear on your belt, after which the camera exits your body painlessly in your stool. You may still need endoscopy with biopsy to confirm a diagnosis of Crohn's disease.

• Double-balloon endoscopy: For this test, a longer scope is used to look further into the small bowel where standard endoscopes don't reach. This technique is useful when capsule endoscopy shows abnormalities, but the exact diagnosis is still in question.

Imaging procedures • X-ray: If you have severe symptoms, your doctor may use a standard X-ray of your abdominal area to rule out serious complications, such as a perforated colon. • Computerized tomography (CT) scan: You may have a CT scan — a special X-ray technique that provides more detail than a standard X-ray does. This test looks at the entire bowel as well as at tissues outside the bowel. • CT enterography is a special CT scan that provides better images of the small bowel. This test has replaced barium X-rays in many medical centers
: An MRI scanner uses a magnetic field and")
• Magnetic resonance imaging (MRI): An MRI scanner uses a magnetic field and radio waves to create detailed images of organs and tissues. MRI is particularly useful for evaluating a fistula around the anal area (pelvic MRI) or the small intestine (MR enterography). Unlike CT, there is no radiation exposure with MRI. • Small bowel imaging: This test looks at the part of the small bowel that can't be seen by colonoscopy. After you drink a liquid containing barium, doctors take an X-ray of your small intestine. While this technique may still be used, it has largely been replaced by CT or MRI

Treatments and drugs

• The goal of inflammatory bowel disease treatment is to reduce the inflammation that triggers your signs and symptoms. In the best cases, this may lead not only to symptom relief but also to long-term remission and reduced risks of complications. • IBD treatment usually involves either drug therapy or surgery. • Doctors use one of two approaches to treatment: "step-up, " which starts with milder drugs first, versus "topdown, " which gives people stronger drugs earlier in the treatment process

Anti-inflammatory drugs • Anti-inflammatory drugs are often the first step in the treatment of inflammatory bowel disease. They include: Aminosalicylates: • Sulfasalazine can be effective in reducing symptoms of ulcerative colitis and for some people with Crohn's disease confined to the colon, but it has a number of side effects, including digestive distress and headache. • Certain 5 -aminosalicylates — including mesalamine , balsalazide and olsalazine — are available in both oral and enema or suppository forms. • Which form you take depends on the area of your colon that's affected. Rarely, these medications have been associated with kidney and pancreas problems.

Drug Sulfasalazine Mesalamine Indication UC: mild-tomoderate maintenance CD: limited role Adverse Reactions Comment N/V, diarrhea, HA, High ADR rate has rash, caused use to myelosuppression decline UC: mild-to. N/V, diarrhea, HA, Topical forms moderate abdominal pain effective for proctitis induction/maintena and distal UC nce CD: limited role Olsalazine As above, diarrhea common Balsalazide As above
 Delivery System Release Frequency Mesalamine (Asacol)")
Intestinal Site of Usual Dose and Generic (Trade) Delivery System Release Frequency Mesalamine (Asacol) p. H-dependent Ileum (distal), colon 800 mg PO TID coating (Eudragit S) dissolves at p. H ≥ 7 Mesalamine (Lialda) Multi-matrix (p. H- Ileum (distal), colon 2. 4– 4. 8 g PO QD sensitive coating and delayed-release) Mesalamine Controlled-release Duodenum, 1 g PO QID (Pentasa) microspheres jejunum, ileum, colon Mesalamine Direct topical Rectum (supp) 500 mg PR QD-BID (Rowasa) therapy Descending 4 g/60 m. L enema PR colon/rectum QHS (enema) Olsalazine Bacterial cleavage of Colon 500 mg PO BID (Dipentum) azo bond Sulfasalazine Bacterial cleavage of Colon Initially 500 mg PO (Azulfidine) azo bond BID; increase to 1 g PO TID-QID Balsalazide (Colazal) Bacterial cleavage of azo bond Colon 750 mg PO TID

Corticosteroids: These drugs, which include prednisone and hydrocortisone, are generally reserved for moderate to severe ulcerative colitis or Crohn's disease that doesn't respond to other treatments. • They are given orally, intravenously, or by enema or suppository, depending on the part of the digestive tract affected. • Corticosteroids have numerous side effects, including a puffy face, excessive facial hair, night sweats, insomnia and hyperactivity. • More-serious side effects include high blood pressure, diabetes, osteoporosis, bone fractures, cataracts, glaucoma and increased chance of infection. They are not usually given long term.

Drug Indication UC: mild-to. Cortico Steroids: severe induction prednisone and CD: mild-tohydrocortisone severe induction Budesonide UC: limited role CD: mild-tomoderate induction/maint enance Dose Various 9 mg daily Adverse Reactions Comment Hyperglycemia, Goal should be CNS excitation, avoiding chronic immunosuppres use in UC and sion, CD osteoporosis, cataracts As above for Long-term use corticosteroids, may still cause probably less chronic short-term corticosteroid effects ADRs

Immune system suppressors • These drugs also reduce inflammation, but they target your immune system rather than directly treating inflammation. • They suppress the immune response that releases inflammation-inducing chemicals in the intestinal lining. • For some people, a combination of these drugs works better than one drug alone.

• Immunosuppressant drugs include: • Azathioprine and mercaptopurine. • These are the most widely used immuno suppressants for the treatment of IBD. • Taking them requires that you follow up closely with your doctor and have your blood checked regularly to look for side effects, including effects on the liver and pancreas. • Additional side effects include lowered resistance to infection and a rare chance of developing cancers such as lymphoma and skin cancers.

• Cyclosporine. • This drug is normally reserved for people who haven't responded well to other medications. Its use is generally confined to ulcerative colitis. • Cyclosporine has the potential for serious side effects — such as kidney and liver damage, seizures and fatal infections — and is not for long-term use. • There's also a small risk of cancer, so let your doctor know if you've previously had cancer. It is now used much less often because safer alternatives are available.

• Methotrexate. • This drug — which is used mainly to treat cancer, psoriasis and rheumatoid arthritis — is sometimes used for people with Crohn's disease who don't respond well to other medications. It is given by injection. • Short-term side effects include nausea, fatigue and diarrhea, and rarely, it can cause potentially lifethreatening pneumonia. • Long-term use can lead to bone marrow suppression, scarring of the liver and sometimes cancer. You will need to be followed closely for side effects.

UC: mild-to 6 severe MP/azathiopri maintenance ne CD: mild-tosevere maintenance 6 -MP: 0. 75– 1. 5 N/V, diarrhea, mg/kg/day HA, rash, Azathioprine: myelosuppresi 1. 5– 2. 5 on mg/kg/day ( neutropenia), pancreatitis UC: limited role 25 mg IM/SQ N/V, stomatitis, Usually reserved Methotrexate CD: mild-to- weekly induction hepatoxicity, for patients who moderate dose, then 15 mg pulmonary have failed 6 induction/maint weekly for fibrosis MP/azathioprine enance maintenance
-alpha inhibitors, or \"biologics, \" • Infliximab, Adalimumab and Golimumab. •")
Tumor necrosis factor (TNF)-alpha inhibitors, or "biologics, " • Infliximab, Adalimumab and Golimumab. • work by neutralizing a protein produced by your immune system. • They are for people with moderate to severe Crohn's disease or ulcerative colitis who don't respond to or can't tolerate other treatments. • Infliximab is given by intravenous injection and the others by subcutaneous injection. They may be combined with other immunosuppressant medications such as azathioprine or mercaptopurine.

• People with certain conditions can't take TNF-alpha inhibitors. If you have a history of tuberculosis, fungal infections or hepatitis B, you may experience a reactivation of your disease while on therapy. Your doctor will test you for previous exposure to tuberculosis and hepatitis B and may test you for possible fungal infection as well. • These drugs also are associated with a rare risk of developing certain cancers such as lymphoma and skin cancers.

• • • Natalizumab and vedolizumab. These drugs work by stopping certain immune cell molecules — integrins — from binding to other cells in your intestinal lining. These drugs are approved for people with moderate to severe Crohn's disease and ulcerative colitis with evidence of inflammation who aren't responding well to any other medications. Because natalizumab is associated with a rare but serious risk of progressive multifocal leukoencephalopathy — a brain infection that usually leads to death or severe disability — you must be enrolled in a special restricted distribution program to use it. Vedolizumab recently was approved for Crohn's disease. It works like natalizumab but appears not to have a risk of brain infection.

Antibiotics • People with ulcerative colitis who run fevers will likely be given antibiotics to prevent or control infection. • Antibiotics can reduce the amount of drainage and sometimes heal fistulas and abscesses in people with Crohn's disease. • Researchers also believe antibiotics help reduce harmful intestinal bacteria and suppress the intestine's immune system. • They may be used in addition to other medications or when infection is a concern — in cases of perianal Crohn's disease, . However, there's no strong evidence that antibiotics are effective for Crohn's disease.

• Frequently prescribed antibiotics include: • Metronidazole. • At one time, metronidazole was the most commonly used antibiotic for Crohn's disease. • It can cause serious side effects, including numbness and tingling in your hands and feet and, occasionally, muscle pain or weakness. • If these effects occur, stop the medication and call your doctor. • You should also not drink alcohol while taking this medication because of severe side effects — including nausea, vomiting and tremor — due to the interaction of the drug with alcohol.

• Ciprofloxacin. • This drug, which improves symptoms in some people with Crohn's disease, is now generally preferred to metronidazole. A rare side effect is tendon rupture, which is an increased risk if you're also taking corticosteroids.

Other medications • In addition to controlling inflammation, some medications may help relieve your signs and symptoms, but always talk to your doctor before taking any over-thecounter medications. Depending on the severity of your Crohn's disease, your doctor may recommend one or more of the following

• Anti-diarrheal medications. A fiber supplement — such as psyllium powder or methylcellulose — can help relieve mild to moderate diarrhea by adding bulk to your stool. For more severe diarrhea, loperamide may be effective. Anti-diarrheal medications should only be used after discussion with your doctor. • Pain relievers. For mild pain, your doctor may recommend acetaminophen. However, ibuprofen, naproxen sodium and diclofenac sodium likely will make your symptoms worse and can make your disease worse as well.

• Iron supplements. If you have chronic intestinal bleeding, you may develop iron deficiency anemia and need to take iron supplements. • Vitamin B-12 shots. Crohn's disease can cause vitamin B-12 deficiency. Vitamin B-12 helps prevent anemia, promotes normal growth and development, and is essential for proper nerve function. • Calcium and vitamin D supplements. Crohn's disease and steroids used to treat it can increase your risk of osteoporosis, so you may need to take a calcium supplement with added vitamin D.

• Nutrition. • Your doctor may recommend a special diet given via a feeding tube (enteral nutrition) or nutrients injected into a vein (parenteral nutrition) to treat your Crohn's disease. • This can improve your overall nutrition and allow the bowel to rest. • Bowel rest can reduce inflammation in the short term. • If you have a stenosis or stricture in the bowel, your doctor may recommend a low-residue diet. This will help to minimize the chance that undigested food will get stuck in the narrowed part of the bowel and lead to a blockage.

Surgery • If diet and lifestyle changes, drug therapy, or other treatments don't relieve your IBD signs and symptoms, your doctor may recommend surgery. Surgery for ulcerative colitis. • Surgery can often eliminate ulcerative colitis, but that usually means removing your entire colon and rectum (proctocolectomy). • In most cases, this involves a procedure called ileoanal anastomosis that eliminates the need to wear a bag to collect stool. Your surgeon constructs a pouch from the end of your small intestine. The pouch is then attached directly to your anus, allowing you to expel waste relatively normally. • In some cases, a pouch is not possible. Instead, surgeons create a permanent opening in your abdomen (ileal stoma) through which stool is passed for collection in an attached bag.

Surgery for Crohn's disease. • Up to one-half of people with Crohn's disease will require at least one surgery. • During surgery, the doctor removes a damaged portion of your digestive tract and then reconnects the healthy sections. • Surgery may also be used to close fistulas and drain abscesses. • A common procedure for Crohn's disease is strictureplasty, which widens a segment of the intestine that has become too narrow. • The benefits of surgery for Crohn's disease are usually temporary. The disease often recurs, frequently near the reconnected tissue. • The best approach is to follow surgery with medication to minimize the risk of recurrence. • If you have had surgery on your colon or where your small intestine and colon meet, your doctor may recommend a repeat colonoscopy in six to 12 months to look for signs of disease and help with correct treatment

Diet • There's no firm evidence that what you eat actually causes inflammatory bowel disease. • But certain foods and beverages can aggravate your signs and symptoms, especially during a flare-up. • It can be helpful to keep a food diary to keep track of what you're eating, as well as how you feel. • If you discover some foods are causing your symptoms to flare, you can try eliminating those foods. Here are some suggestions that may help

• Limit dairy products Many people with inflammatory bowel disease find that problems such as diarrhea, abdominal pain and gas improve. You may be lactose intolerant — that is, your body can't digest the milk sugar (lactose) in dairy foods. • Try low-fat foods. If you have Crohn's disease of the small intestine, you may not be able to digest or absorb fat normally. Instead, fat passes through your intestine, making your diarrhea worse. Try avoiding butter, margarine, cream sauces and fried foods. • Take care with fiber. If you have inflammatory bowel disease, high-fiber foods, such as fresh fruits and vegetables and whole grains, may make your symptoms worse, especially if you have narrowing in the bowel. If raw fruits and vegetables bother you, try steaming, baking or stewing them • Avoid other problem foods. Spicy foods, alcohol and caffeine may make your signs and symptoms worse.

Other dietary measures • Eat small meals. You may find you feel better eating five or six small meals a day rather than two or three larger ones. • Drink plenty of liquids. Try to drink plenty of fluids daily. Water is best. Alcohol and beverages that contain caffeine stimulate your intestines and can make diarrhea worse, while carbonated drinks frequently produce gas. • Consider multivitamins. Because Crohn's disease can interfere with your ability to absorb nutrients and because your diet may be limited, multivitamin and mineral supplements are often helpful. Check with your doctor before taking any vitamins or supplements. • Talk to a dietitian. If you begin to lose weight or your diet has become very limited, talk to a registered dietitian.
")
Alternative medicine • Probiotics. Researchers suspect that adding more of the beneficial bacteria (probiotics) that are normally found in the digestive tract might help combat IBD. there is some evidence that adding probiotics along with other medications may be helpful. • Fish oil acts as an anti-inflammatory, and there is some evidence that adding fish oil to aminosalicylates may be helpful, but this has not been proved. Fish oil can cause diarrhea. • Aloe vera gel may have an anti-inflammatory effect for people with ulcerative colitis, but it also can cause diarrhea. • Turmeric. Curcumin, a compound found in the spice turmeric, has been combined with standard ulcerative colitis therapies in clinical trials. There is some evidence of benefit, but more research is needed.

• Acupuncture. This procedure involves the insertion of fine needles into the skin, which may stimulate the release of the body's natural painkillers. Only one clinical trial has been conducted regarding its benefit for ulcerative colitis. • Prebiotics. Unlike probiotics — which are beneficial live bacteria that you consume — prebiotics are natural compounds found in plants, such as artichokes, that help fuel beneficial intestinal bacteria. Studies have not shown positive results of prebiotics for people with Crohn's disease.

THANK YOU
- Slides: 57