Inflammatory Bowel Disease Dr Omar S Mansour Consultant

Inflammatory Bowel Disease Dr Omar S. Mansour Consultant Colorectal Surgeon BAU`
 is an idiopathic disease")
Inflammatory Bowel Disease • Definition • Inflammatory bowel disease (IBD) is an idiopathic disease caused by a dysregulated immune response to host intestinal microflora. • The two major types of inflammatory bowel disease are ulcerative colitis (UC) and Crohn’s Disease.
, which is limited to the colonic mucosa •")
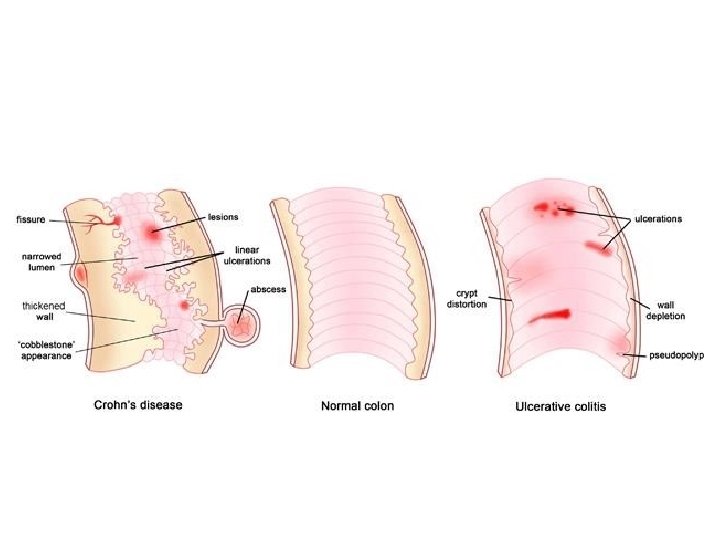
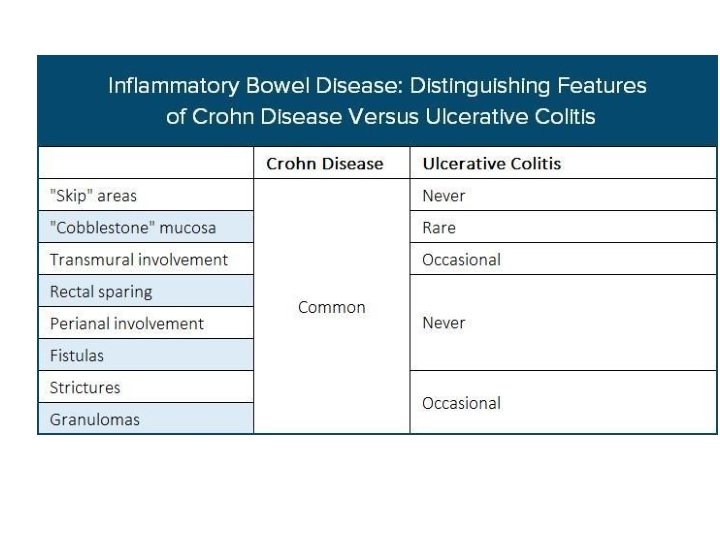
Main types • Ulcerative colitis (UC), which is limited to the colonic mucosa • Crohn disease (CD) which can affect any segment of the gastrointestinal tract from the mouth to the anus, involves "skip lesions, " and is transmural • Indeterminate Colitis

Epidemiology of the IBD • In the United States, it is currently estimated that about 1 – 1. 3 million people suffer from IBD. 1, 2 • Sex: • Ulcerative colitis is slightly more common in males, while Crohn’s disease is more frequent in women. • .

Epidemiology • Ethnicity: • IBD occurs more in people of Caucasian and Ashkenazic Jewish origin than in other racial and ethnic subgroups. • Previously noted racial and ethnic differences seem to be narrowing though. •

Incidence Rate (number of newly diagnosed cases per 100, 000 person-years Crohn’s disease Ulcerative colitis 3. 1 to 14. 6 cases per 100, 000 person 2 years 2. 2 to 14. 3 cases per 100, 000 person 2 years
 Crohn’s disease 26 to")
Prevelance Prevalence (number of existing cases per 100, 000 population) Crohn’s disease 26 to 199 cases per 100, 000 persons 201 per 100, 000 adults 1 2 Ulcerative colitis 37 to 246 cases per 100, 000 persons 238 per 100, 000 adults 1 2

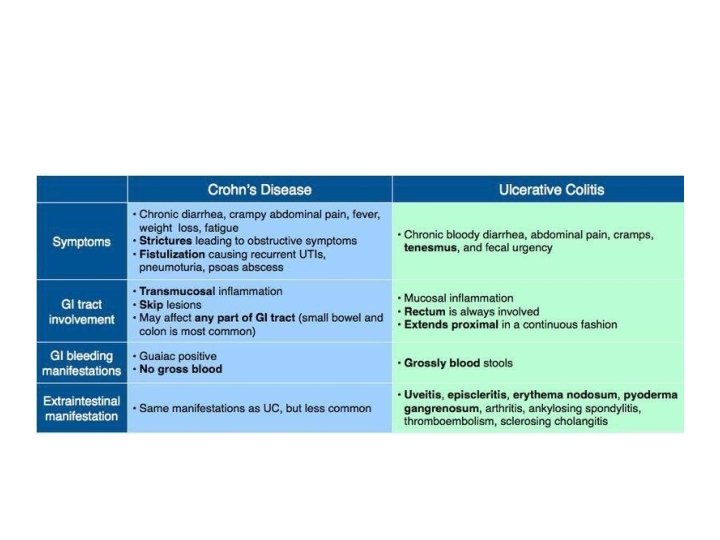
Signs and symptoms • Generally, the manifestations of IBD depend on the area of the intestinal tract involved. The symptoms, however, are not specific for this disease. They are as follows: • Abdominal cramping • Irregular bowel habits, passage of mucus without blood or pus • Weight loss • Fever, sweats

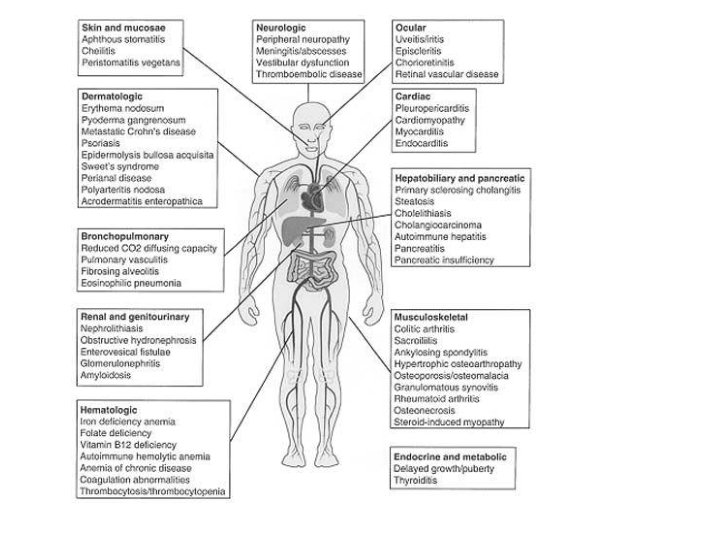
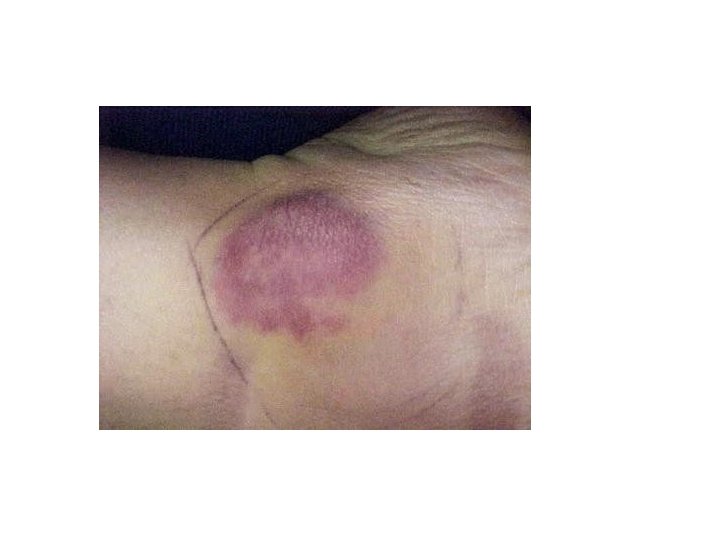
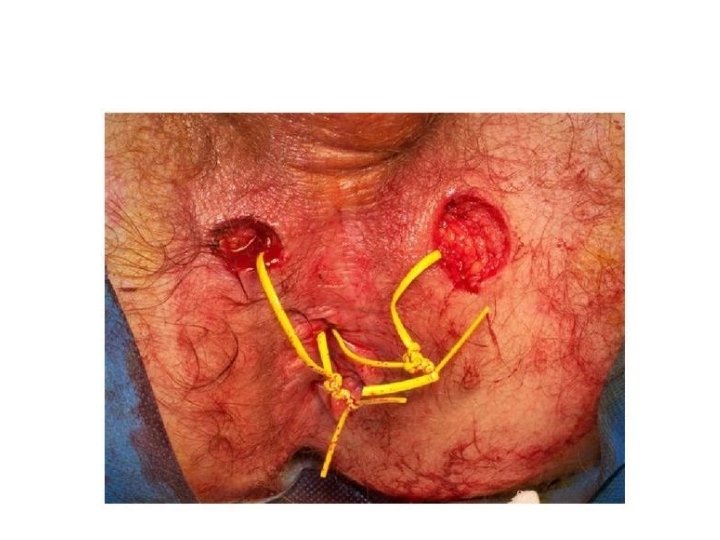
Signs and Symtoms • Malaise, fatigue • Arthralgias • Growth retardation and delayed or failed sexual maturation in children • Extraintestinal manifestations (10 -20%): Arthritis, uveitis, or liver disease • Grossly bloody stools, occasionally with tenesmus: Typical of UC, less common in CD • Perianal disease (eg, fistulas, abscesses): Fifty percent of patients with CD

Diagnosis • Examination in patients with IBD may include the following findings, which are directly related to the severity of the attack: • Fever • Tachycardia • Dehydration • Toxicity • Pallor, anemia

Diagnosis • Toxic megacolon: Medical emergency; patients appear septic, have high fever, lethargy, chills, and tachycardia, as well as have increasing abdominal pain, tenderness, distention • Mass in the right lower abdominal quadrant: May be present in CD • Perianal complications: May be observed in up to 90% of cases of CD [2]

Investigations • Although several laboratory studies may aid in the management of IBD and provide supporting information, no laboratory test is specific enough to adequately and definitively establish the diagnosis, including the following: • Complete blood count CBC

Ix • Nutritional evaluation: Vitamin B 12 evaluation, iron studies, red blood cell folate, nutritional markers • Erythrocyte sedimentation rate ESR and C-reactive protein levels CRP • Faecal calprotectin level • Serologic studies: Perinuclear antineutrophil cytoplasmic antibodies (ANCA), anti-Saccharomyces cerevisiae antibodies (ASCA) • Stool studies: Stool culture, ova and parasite studies, bacterial pathogens culture, and evaluation for Clostridium difficile infection [3]

Imaging studies • • • Upright chest and abdominal radiography Barium double-contrast enema radiographic studies Abdominal ultrasonography Abdominal/pelvic computed tomography scanning/magnetic resonance imaging Computed tomography enterography Colonoscopy, with biopsies of tissue/lesions Flexible sigmoidoscopy Upper gastrointestinal endoscopy Capsule enteroscopy/double balloon enteroscopy

Management Approach • The medical approach for patients with IBD is symptomatic care (ie, relief of symptoms) and mucosal healing following a stepwise approach to medication, with escalation of the medical regimen until a response is achieved (“step-up” or “stepwise” approach), such as the following:
: For treating flares and")
MX • Step I – Aminosalicylates (oral, enema, suppository formulations): For treating flares and maintaining remission; more effective in UC than in CD • Step IA – Antibiotics: Used sparingly in UC (limited efficacy, increased risk for antibioticassociated pseudomembranous colitis); in CD, most commonly used for perianal disease, fistulas, intra-abdominal inflammatory masses
: For acute disease flares")
Mx • Step II – Corticosteroids (intravenous, oral, topical, rectal): For acute disease flares only • Step III – Immunomodulators: Effective for steroid-sparing action in refractory disease; primary treatment for fistulas and maintenance of remission in patients intolerant of or not responsive to aminosalicylates • Step IV – Clinical trial agents: Tend to be diseasespecific (ie, an agent works for CD but not for UC, or vice versa)

Pharmacotherapy • The following medications may be used in patients with IBD: • 5 -Aminosalicylic acid derivatives (eg, sulfasalazine, mesalamine, balsalazide, olsalazine) • Antibiotics (eg, metronidazole, ciprofloxacin, rifaximin) • Corticosteroid agents (eg, hydrocortisone, prednisone, methylprednisolone, budesonide, dexamethasone)
 • Tumor necrosis factor")
Mx • Immunosuppressant agents (eg, azathioprine, 6 -mercaptopurine, methotrexate, cyclosporine) • Tumor necrosis factor inhibitors (eg, infliximab, adalimumab, certolizumab pegol) • Monoclonal antibodies (eg, natalizumab) • H 2 -receptor antagonists (eg, cimetidine, ranitidine, famotidine, nizatidine) • Proton pump inhibitors (eg, omeprazole, lansoprazole, esomeprazole magnesium, rabeprazole sodium, pantoprazole) • Antidiarrheal agents (eg, diphenoxylate and atropine, loperamide, cholestyramine) • Anticholinergic antispasmodic agents (eg, dicyclomine, hyoscyamine)

Surgery • UC is surgically curable. However, surgical resection is not curative in CD, with recurrence being the norm. Consider early consultation with a surgeon in the setting of severe colitis or bowel obstruction and in cases of suspected toxic megacolon. • Surgical intervention in IBD includes the following: • UC: Proctocolectomy with ileostomy, total proctocolectomy with ileoanal anastomosis

Sx • Fulminant colitis: Surgical procedure of choice is subtotal colectomy with end ileostomy and creation of a Hartmann pouch • CD: Surgery (not curative) most commonly performed in patients with complications of the disease; generally consists of conservative resection (eg, potential stricturoplasty vs resective surgery) to preserve bowel length in case future additional surgery is needed [4]

Sx • Selected patients with distal ileal or proximal colonic disease: Option for ileorectal or ileocolonic anastomosis • Severe perianal fistulas: Option for diverting ileostomy; generally, resection for symptomatic enteroenteric fistulas






- Slides: 35