Inflammatory Bowel Disease Digestive Specialists Inc 999 Brubaker

Inflammatory Bowel Disease Digestive Specialists, Inc. 999 Brubaker Drive • Kettering, OH 45429 Anjali Morey, M. D. , Ph. D.

Which would be considered a high risk Crohns Disease patient? A. Highly Symptomatic B. Advanced age of disease onset C. Prior Surgical resection D. Disease limited to one section of the colon 25% 25% A. B. C. D. 10

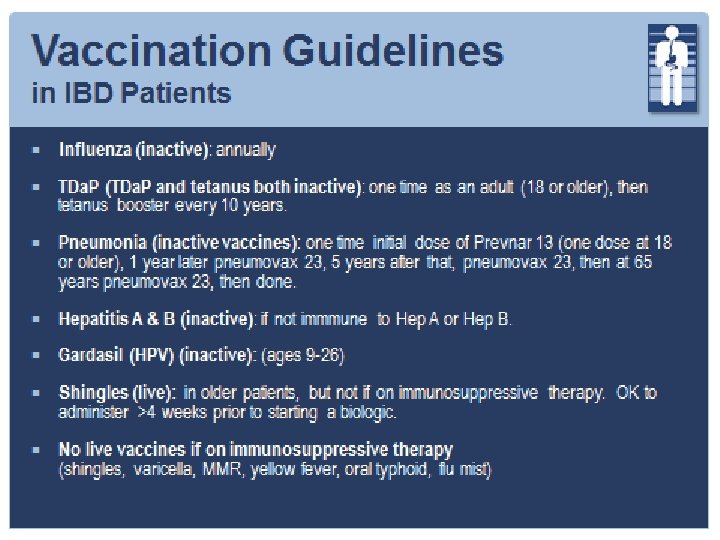
Which vaccine should not be given to an IBD patient on immunosuppressive therapy? A. Influenza B. Pneumonia C. Hep B Vaccine D. Gardasil E. Shingles 20% 20% 20% A. B. C. D. E.

Objectives 1. Review primary care workup for chronic diarrhea when IBD is suspected 2. Report on current treatment recommendations for Ulcerative Colitis and Crohn’s Disease 3. Discuss clinical follow-up of patients on immunosuppressive therapy 4. Discuss lifestyle changes that can help maintain remission

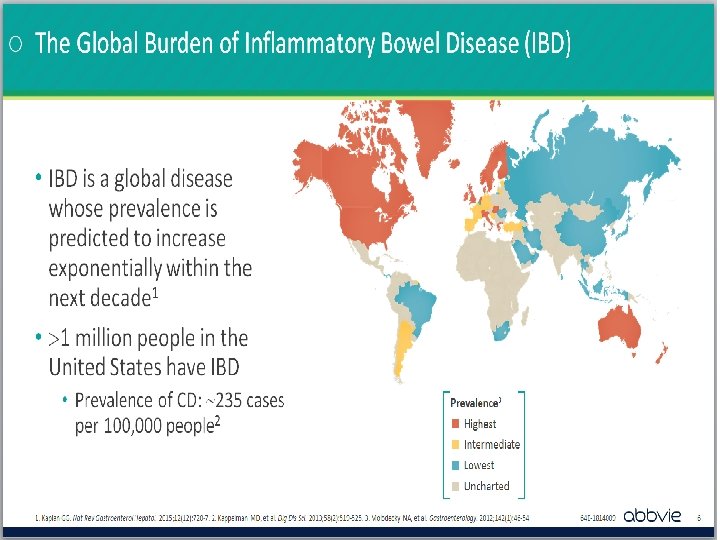
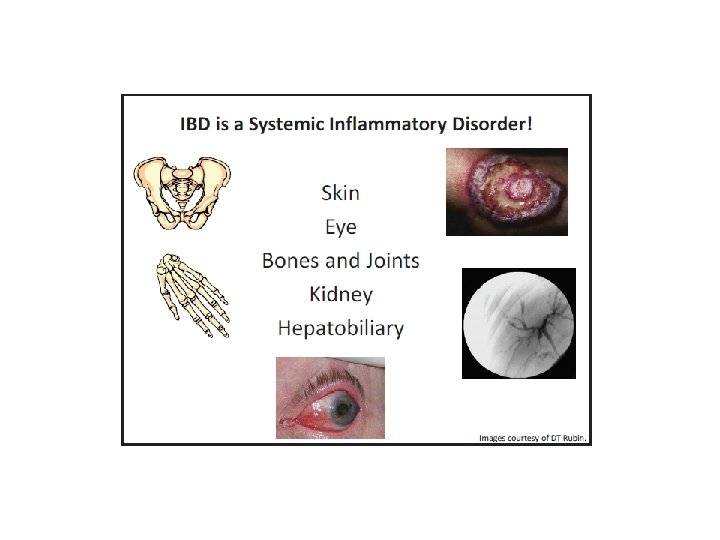
IBD Overview
 Any segment of GI tract (mouth-anus) Rectal Sparing Discontinuous")
Overview of Crohn’s Disease (CD) Any segment of GI tract (mouth-anus) Rectal Sparing Discontinuous “skip lesions” Perianal Disease Transmural inflammation − stricture − fistula − perforation − abscess − skin tags − fissures − fistulae Normal Crohn’s Disease
 Pathologic Changes − Epithelioid non-caseating granulomas − Chronic inflammatory")
Overview of Crohn’s Disease (CD) Pathologic Changes − Epithelioid non-caseating granulomas − Chronic inflammatory infiltrate − Crypt architectural distortion
 Confined to colon Begins in rectum and extends proximally")
Overview of Ulcerative Colitis (UC) Confined to colon Begins in rectum and extends proximally in a continuous fashion Confined to mucosa and submucosa Normal Ulcerative Colitis
 Pathologic changes − Cryptitis / crypt abscesses − Crypt")
Overview of Ulcerative Colitis (UC) Pathologic changes − Cryptitis / crypt abscesses − Crypt architectural distortion − Lamina propria expansion with acute and chronic inflammatory cells

Primary Care Patients often present with diarrhea > 2 weeks

CD: Signs & Symptoms Abdominal Pain Fatigue GI Bleeding Fever Diarrhea Joint Pain Weight Loss Skin Rashes

CD: Staging Workup Initial Steps • Labs • Colonoscopy • TI exam & biopsy If iron deficiency anemia exists and colonoscopy negative • EGD If EGD negative in the setting of iron deficiency anemia • Small Bowel Capsule Endoscopy • Consider imaging prior if any suspicion of narrowing / stricture If abdominal symptoms present • CTE / MRE to assess small bowel

CD: Initial Labs CBC CRP / ESR CMP TSH Strongyloides Antibody Consider Prometheus Testing Consider Absorption Labs

CD: Absorption Labs Iron Studies / Ferritin B-12 / Folic Acid Vitamin D − Vitamin D Target Range (for IBD Patients): 40 - 60 ng/m. L Vitamin A Zinc

CD: Stool Studies to Rule Out Infection / Inflammation Stool Ova and Parasites Stool for C. difficile toxin Stool giardia antigen Stool for Cryptosporidium Stool culture and sensitivity Fecal Calprotectin

CD: Imaging CT Enterography / MR Enterography − Cross-sectional imaging technology − Assess for small intestine disease activity − Assess for complications • Abscess • Fistula • obstruction < 30 y/o, MRE preferred to avoid radiation exposure

CD: High Risk Patients Surgical Resection Deep ulceration Fistula / Stricture Perianal involvement Abscess Early onset of disease and / or severe rectal disease Extensive anatomic involvement

UC: Signs & Symptoms Bloody Diarrhea Weight Loss Tenesmus Joint Pain Urgency Skin Rash Abdominal Pain Fatigue Fever

UC: Labs CBC CMP CRP / ESR Fecal Calprotectin Stool studies to rule out infection

UC: Imaging Case-by-case based on clinical presentation and evaluation Can be used to assess disease extent and severity in severe flare

Mayo Scoring System for Assessment of UC Activity Used for initial evaluation and monitoring treatment response Scores range from 0 to 12 Higher scores indicate more severe disease − ≤ 2 = Clinical remission − 3 -4 = Mild activity − 6 -10 = Moderate activity − 11 -12 = Severe activity

Mayo Scoring System for Assessment of UC Activity Variable 0 Points 1 Points 2 Points 3 Points Bowel Normal movement (BM) frequency 1 -2 BM > normal 3 -4 BM > normal Rectal bleeding None Streaks on stool < 50% BM’s Obvious fresh BM’s with fresh blood with most blood BM’s Endoscopy Normal Mild Erythema, Marked � vascularity, erythema, Mild friability Lack vascular pattern, Friability, Erosions Severe spontaneous bleeding, Ulceration Physician Global Assessment Normal Mild Severe Moderate >5 BM > normal

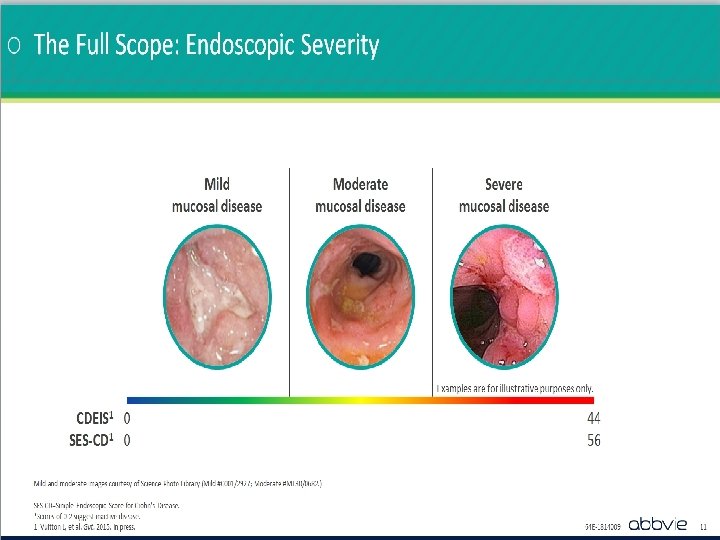
UC: Colonoscopy Used to Assess Disease Severity Mayo Score = 0 Normal / Inactive Disease • No friability or granularity • Intact vascular pattern Mayo Score = 1 Mayo Score = 2 Mayo Score = 3 Mild Disease Moderate Disease Severe Disease • Erythema • Decreased vascular pattern • Mild Friability • • • Moderate signs plus: • Spontaneous bleeding • Ulceration Marked erythema Absent vascular pattern Friability Erosions Mayo Endoscopic Subscore

IBD Therapies

Goals of IBD Therapy Achieve mucosal healing and induce remission Maintain steroid-free remission Prevent / treat complications of disease Avoid short and long term toxicity of therapy Enhance quality of life
 Corticosteroids Immunomodulators (6 MP / AZA / MTX) Biologics")
IBD Therapies Aminosalicylates (5 -ASA) Corticosteroids Immunomodulators (6 MP / AZA / MTX) Biologics − Anti-TNF − Anti-Integrin − Anti IL-12 / IL-23
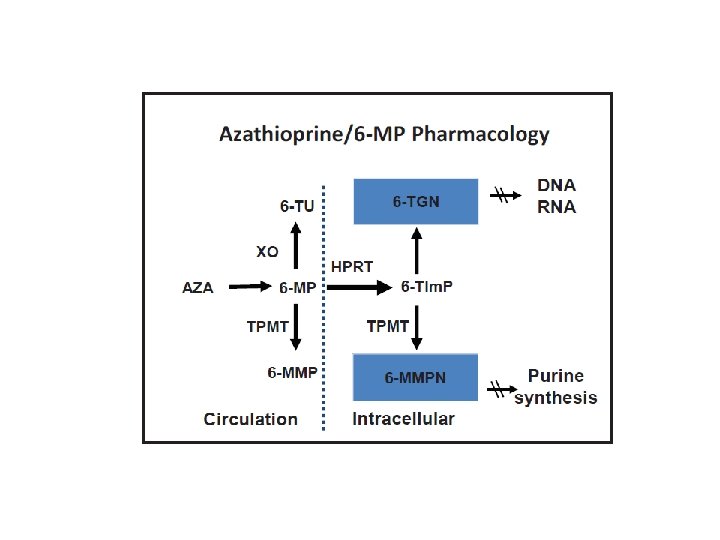
 235 -400 Therapeutic range > 400 Higher")
Azathioprine/6 MP Pharmacology 6 TG (active metabolite) 235 -400 Therapeutic range > 400 Higher risk for bone marrow suppression 6 MMP > 5700 Higher risk for hepatotoxicity
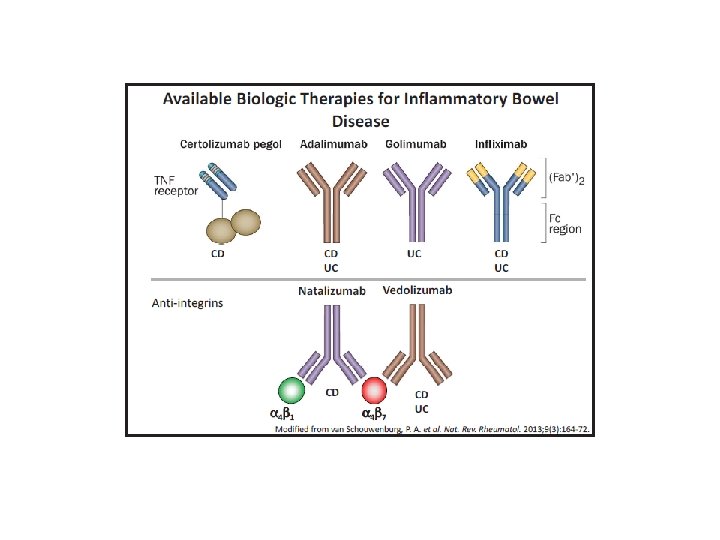

Biologic therapy for IBD Certolizumab - Cimzia Adalimumab - Humira Golimumab -Simponi Infliximab - Remicade Anti-Integrin antibody: Natalizumab -Tysabri (PML –Progressive Multifocal Leucoencephalopathy) Anti-Integrin antibody: Vedolizumab - Entyvio Anti IL-12 / IL-23 antibody: Ustekinumab – Stelara - moderate to severe CD.

Crohn’s Disease Therapies Disease Severity at Presentation Biologics + Thiopurine + Corticosteroid Severe Biologics or Thiopurine + Corticosteroid Moderate Pentasa Mild Pentasa Biologics or Thiopurine Induction Maintenance Therapy is modified according to severity at presentation or failure at prior step

Sequential Therapies for UC Disease Severity at Presentation Severe Moderate Colectomy Biologics + Thiopurine + Corticosteroid Biologics Aminosalicylate or Thiopurine + Aminosalicylate Corticosteroid or Thiopurine Aminosalicylate Mild Induction Maintenance Therapy is stepped up according to severity at presentation or failure at prior step

Guidelines for Initiating and Follow-up of Immunosuppressive Therapy
")
Labs Prior to Start of Immunosuppressive Therapy Quanti. FERON / Chest X-ray (TB Testing) Acute Hepatitis Panel

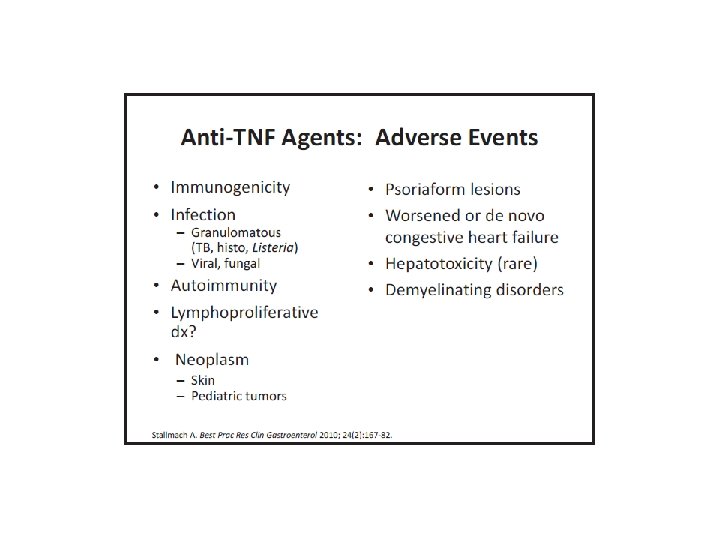
For Patients on Immunosuppressive Therapy Annual head to toe dermatology skin exam Sun precautions Annual Pap smear Annual TB Testing (Quantiferon / chest x-ray) Serial labs (CBC with Diff and Hepatic Function Panel) if on Imuran, 6 MP or MTX

Lifestyle Modifications
 Replace")
Mediterranean Diet Primarily plant-based foods (fruits and vegetables, whole grains, legumes and nuts) Replace butter with healthier fats (olive oil) Herbs and spices instead of salt Limit red meat (beef and pork) to no more than a few times a month Fish, chicken, and turkey at least twice a week Red wine in moderation (optional)

Other Dietary Considerations Eat smaller, more frequent meals Drink plenty of fluids Consider multivitamin once daily Talk to a dietitian Probiotics – Kefir once daily Dairy, gluten, excessive caffeine / carbonation can exacerbate symptoms
 − Relaxation and breathing")
Lifestyle Changes Stress Management − Exercise (20 minutes / day) − Relaxation and breathing exercises (yoga and meditation) Smoking Cessation / avoid second hand smoke exposure Avoid unnecessary antibiotic exposure Utilize Patient Education Resources (CCFA)

Final Thoughts Early diagnosis / avoid treatment delays Treating IBD patients is a collaborative approach between primary care and GI and other specialists Increase patient satisfaction
- Slides: 48