INFECTIOUS MONONUCLEOSIS Dr R Bindhusaran Associate professor DEPT

INFECTIOUS MONONUCLEOSIS Dr. R. Bindhusaran, Associate professor DEPT OF PATHOLOGY, SKHMC, Kulasekharam
 or glandular fever is a benign, self-limiting lymphoproliferative")
INFECTIOUS MONONUCLEOSIS • Infectious mononucleosis (IM) or glandular fever is a benign, self-limiting lymphoproliferative disease caused by Epstein-Barr virus (EBV), one of the herpes viruses. • Infection may occur from childhood to old age but the classical acute infection is more common in teenagers and young adults. • The infection is transmitted by person-to-person contact such as by kissing with transfer of virallycontaminated saliva.

• Primary infection in childhood is generally asymptomatic, while 50% of adults develop clinical manifestations. • EBV is oncogenic as well and is strongly implicated in the African (endemic) Burkitt’s lymphoma and nasopharyngeal carcinoma

Transmission • Mononucleosis is typically transmitted from asymptomatic individuals • Through saliva, earning it the name "the kissing disease", • By sharing a drink • Sharing eating utensils. • In most individuals, these antibodies remain in their system, creating lifelong immunity to further infections

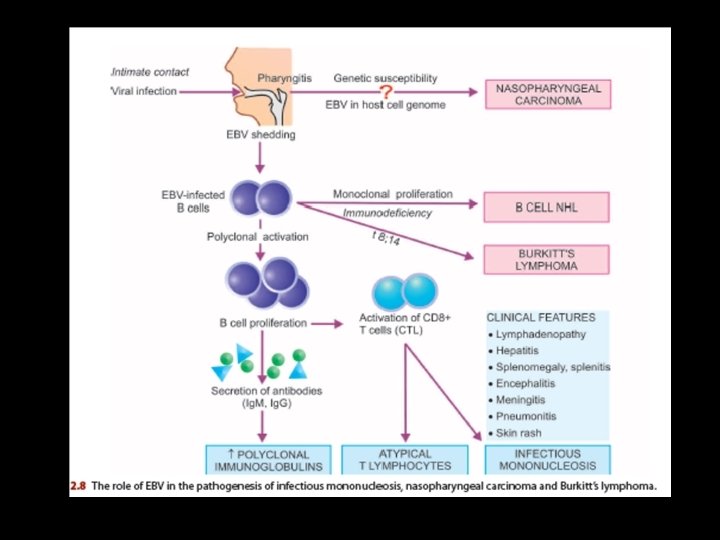
PATHOGENESIS • EBV, the etiologic agent for IM, is a B lymphotropic herpesvirus. • The disease is characterised by fever, generalised lymphadenopathy, hepatosplenomegaly, sore throat, and appearance in blood of atypical ‘mononucleosis cells’

Pathogensis • 1. In a susceptible host the virus in the contaminated saliva invades and replicates within epithelial cells of the salivary gland • Then enters B cells in the lymphoid tissues which possess receptors for EBV. • The infection spreads throughout the body via bloodstream or by infected B cells.

• Viraemia and death of infected B cells cause an acute febrile illness and appearance of specific humoral antibodies which peak about 2 weeks after the infection and persist throughout life. • The appearance of antibodies marks the disappearance of virus from the blood. • 3. Though the viral agent has disappeared from the blood, the EBV-infected B cells continue to be present in the circulation as latent infection. • EBV-infected B cells undergo polyclonal activation and proliferation.

• They secrete antibodies—initially Ig. M but later Ig. G class antibodies appear • They activate CD 8+ T lymphocytes—also called cytotoxic T cells (or CTL) or suppressor T cells. • CD 8+ T cells bring about killing of B cells and are pathognomonic atypical lymphocytes seen in blood in IM. • The proliferation of these cells is responsible for generalized lymphadenopathy and hepatosplenomegaly.

CLINICAL FEATURES • The incubation period of IM is 30 -50 days in young adults, while children have shorter incubation period. • The usual clinical features are as under: • 1. During prodromal period (first 3 -5 days), the symptoms • are mild such as malaise, myalgia, headache and fatigue. • 2. Frank clinical features (next 7 -21 days) seen commonly are fever (90%), sore throat (80%) and bilateral cervical lymphadenopathy (95%). • Other features are splenomegaly (50% patients), hepatomegaly (10% cases), transient erythematous maculopapular rash on the trunk and extremities (10%), periorbital oedema (10%) and jaundice (5%).

 Neurologic manifestations in children. • ii) Splenic rupture due to splenitis.")
Complications: • i) Neurologic manifestations in children. • ii) Splenic rupture due to splenitis. • iii) Upper airway obstruction due to hypertrophied adenotonsillitis. • iv) Autoimmune haemolytic anaemia • v) Bacterial superinfection. • vi) Rarely, myocarditis, hepatitis, pneumonia.
 TLC There is a moderate rise")
LABORATORY FINDINGS • 1. HAEMATOLOGIC FINDINGS • i) TLC There is a moderate rise in total white cell count • (10, 000 -20, 000/μl) during 2 nd to 3 rd week after infection. • ii) DLC There is an absolute lymphocytosis. The lymphocytosis is due to rise in normal as well as atypical T lymphocytes. There is relative neutropenia. • iii) Atypical T cells Essential to the diagnosis of IM is the presence of at least 10 -12% atypical T cells (or mononucleosis cells) lying in peripheral blood lymphocytosis

atypical lymphocytes
 CD 4+ and CD 8+ T cell counts • There is")
• iv) CD 4+ and CD 8+ T cell counts • There is reversal of CD 4+/CD 8+ T cell ratio. There is marked decrease in CD 4+T cells while there is substantial rise in CD 8+ T cells. • v) Platelets • There is generally thrombocytopenia in the first 4 weeks of illness.
 Test for heterophile antibodies • Heterophile antibody test (Paul-Bunnell test):")
SEROLOGIC DIAGNOSIS • i) Test for heterophile antibodies • Heterophile antibody test (Paul-Bunnell test): • A high serum titer of 40 or more times is diagnostic of acute IM infection in symptomatic case in the first week. • Heterophile antibodies peak during the 3 rd week in 80 -90% cases. • The test remains positive for about 3 months after the illness started.

• EBV-specific antibody tests • Specific antibodies against the viral capsid and nucleus of EBV can be demonstrated in patients who are negative for heterophile antibody test: • Specific antibody against EBV capsid antigen show elevated titers in over 90% cases during acute infection. Ig. M class antibody appears early and is thus most useful for diagnosis of acute infection. Ig. G class antibody appears later
 EBV antigen detection • Detection of EBV DNA or proteins can")
• iii) EBV antigen detection • Detection of EBV DNA or proteins can be done in blood or CSF by PCR method. • 3. LIVER FUNCTION TESTS • In addition, abnormalities o the liver function test are found in about 90% of cases. • These include elevated serum levels of transaminase(SGOT and SGPT), rise in serum alkaline phosphatase and mild elevation of serum bilirubin.

Reference • Harsh Mohan Text Book of Pathology • Robbins & Cotran Pathologic Basis of Disease,
- Slides: 20