Infections Paediatrics Public Health Notifiable Diseases Acute encephalitis
")
Infections (Paediatrics)

Public Health: Notifiable Diseases ● Acute encephalitis ● Acute infectious hepatitis ● Acute meningitis ● Acute poliomyelitis ● Anthrax ● Botulism ● Brucellosis ● Cholera ● Diphtheria ● Enteric fever (typhoid or paratyphoid fever) ● Food poisoning ● Haemolytic uraemic syndrome (HUS) ● Infectious bloody diarrhoea ● Invasive group A streptococcal disease ● Legionnaires’ disease ● Leprosy ● Malaria ● Measles ● Meningococcal septicaemia ● Mumps ● Plague ● Rabies ● Rubella

Pathogens

Pathogens

Prokaryote vs Eukaryote ● Prokaryote ○ ● No membrane bound organelles Eukaryote ○ ○ Membrane bound organelles (e. g. Nucleus)

Viruses ● ● ● Need a host cell to reproduce in No cell wall Smaller than bacteria REplicate faster than bacteria E. g Rotavirus, HIV

Bacteria ● ● ● Prokaryotes Self-reproducing Organelles More complex Spheres, rods and spirals

Parasites ● Organism lives on / in a host ● Disease causing
")
Fungi ● Overgrowth can lead to symptoms ● E. g Thrush (Candida)

Protazoa ● Unicellular eukaryotic organisms ● Sub Kingdom of protista ● Get food from surrounding environment ● E. g. Malaria

Prion ● ● ● Type of protein Triggers normal proteins to fold abnormally Can spread through infected meat products Prion diseases are a group of neurodegenerative conditions E. g. CJD (Creutzfeldt-Jakob Disease)

UK Immunisation Schedule
 6")
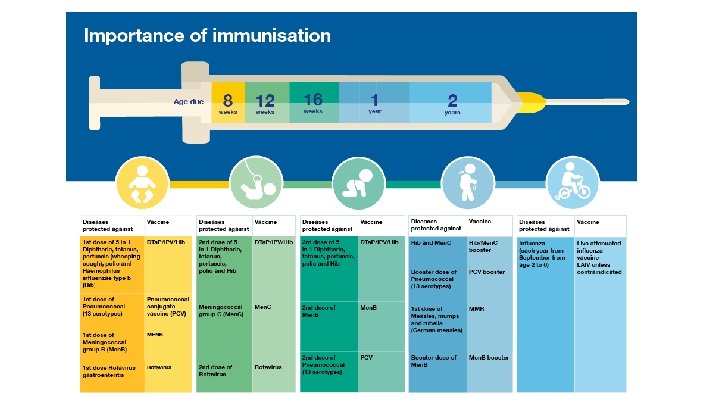
UK Immunisation Schedule *Changed from 5 -in-1 to 6 -in-1 (+ Hep B) 6 -in-1 1. 2. 3. 4. 5. 6. Diphtheria Tetanus Pertussis (Whooping cough) Polio Hib (Haemophilus influenzae type b) Hepatitis B Give at 8 w, 12 w, 16 w
 6 - in - 1 Pneumococcal (PCV) Rotavirus (D&V common")
2 months (8 w) 6 - in - 1 Pneumococcal (PCV) Rotavirus (D&V common cause) 3 months (12 w) 6 - in - 1 Meningitis C Rotavirus (D&V common cause) 4 months (16 w) 6 - in - 1 Meningitis C 12 months (1 year) Hib Meningitis C 13 months MMR (Measles, mumps, rubella) Pneumococcal (PCV) 3 -5 years Diphtheria, Tetanus, Whooping Cough, Polio (4 -in-1 pre-school booster) MMR 13 -18 years Tetanus, Diphtheria, Polio (Booster) HPV (girls only - cervical cancer) Annual / lifetime Flu BCG (against TB) / chicken-pox ACWY - 14 years / University students aged 19 -25

Physiology
 Born")
Fetus / Childhood ● ● Infective agent → mounts an immune response (normally) Born with immature immune complexes Circulating immunoglobulins from mother (transplacental) Decrease during first few months of life ○ Susceptible to infections ● (risk of congenital / acquired immunodeficiency) ○ ○ ○ HIV Chromosomal syndromes Maternal infection ■ Bloodborne ■ Infection during pregnancy

Paediatric Infections

Viral Infections

NOTIFY PUBLIC HEALTH ENGLAND! Measles
")
Measles ● UK Vaccine programme ○ ● ● ● ● MMR (measles, mumps, rubella) ■ Autism / IBD scares surrounding vaccine - Andrew Wakefield Cause: measles virus Droplet spread Incubation period 10 -14 days Fever Rash Koplik’s spots Conjunctivitis / coryza Cough

Measles - Clinical Features ● Rash ○ ○ ○ Spreads downwards from behind the ears Whole body Maculopapular rash ● Fever ● Koplik’s spots ○ White spots on buccal mucosa ● Conjunctivitis ● Coryza ● Cough

Measles - Treatment ● ● No curative treatment Symptomatic Isolation (especially if admitted to hospital) Immunocompromised patients: ○ Ribavirin ● Vitamin A given in developing countries to modulate immune response

Complications ● ● ● Respiratory ○ Pneumonia ○ Secondary bacterial infection and otitis media ○ Tracheitis Neurological ○ Febrile convulsions ○ EEG abnormalities ○ Encephalitis ■ 1/5000 - 8 days post onset of symptoms, 15% mortality ○ Subacute sclerosing panencephalitis ■ 1/18, 000 - loss of neurological function → dementia → death ■ Measles antibody in blood, CSF and EEG abnromalities Other ○ Diarrhoea ○ Hepatitis ○ Appendicitis ○ Corneal Ulceration ○ Myocarditis

Mumps

Mumps ● ● ● ● Part of MMR vaccine Cause: Mumps Virus (family: paramyxovirdae (same as measles) Respiratory droplet spread Single stranded RNA Most common in winter and spring First gland affected - Parotid glands Incubation period 15 -24 days

Mumps - Clinical Features ● Initially ○ ○ ○ ● ● Fever Malaise Parotitis Children may complain of earache, pain on eating and drinking Usually mild, self-limiting illness Hearing loss may result - usually unilateral and transient Complications: ○ ○ ○ Viral meningitis Viral encephalitis Orchitis

Rubella
 ● ● ● ● ● Generally mild Winter / spring Can")
Rubella (German Measles) ● ● ● ● ● Generally mild Winter / spring Can severely damage a fetus Incubation period: 15 -20 days Cause: Rubella Virus Rash starts of face and spreads to body ○ May be itchy in children, less likely Lymphadenopathy ○ Suboccipital ○ Postauricular Complications (rare): ○ Arthritis ○ Encephalitis ○ Thrombocytopenia ○ Myocarditis Serological diagnosis No effective treatment - prevention is key
")
Human Herpesviruses (VZV, CMV, EBV, HSV)
")
Chicken Pox (Varicella Virus - Herpesvirus)
 Vesicular rash,")
Chicken Pox ● ● ● Cause: Varicella Zoster Virus (A human herpesvirus) Vesicular rash, itchy Mode of spread: respiratory (highly contagious) Progresses through blood and lymphatics - cause vesicular lesions in skin Complications: ○ ○ Secondary bacterial infection with staph/strep leading to TSS / necrotising fasciitis (consider if new fever after first few days) Encephalitis Purpura fulminans ■ Consequence of vasculitis Strokes ■ Very rare - incidence increased due to vasculitis / protein S deficiency

VZV - Prevention ● ZIG - Human varicella zoster immunoglobulin ○ Recommended for high risk immunocompromised individuals with T-lymphocytes function ■ Neonates ■ Bone marrow transplant recipients ■ Congenital / acquired immune deficiency

NOTE - Shingles ● ● ● Same virus Reactivation of VZV Dermatomal distribution Most commonly occurs in Immunocompromised people Most commonly thoracic

Epstein-Barr Virus
 ● Syndrome ● Causes")
Epstein-Barr Virus ● Major cause of Glandular fever (infectious mononucleosis) ● Syndrome ● Causes → Burkitt’s lymphoma, lymphoproliferative disease, nasopharyngeal carcinoma ● B-lymphocyte and epithelial cells of pharynx

Glandular Fever ● ● Symptoms 1 -3 months Fever Malaise Tonsillopharyngitis ○ (reducing intake of food and fluids) ● Lymphadenopathy ● Splenomegaly (50%) ● Hepatomegaly (10%) ○ Jaundice ● Rash / petechiae on soft palate

Glandular Fever ● Diangosis: ○ ○ ○ Atypical lymphocytes on blood film Positive monospot test - presence of heterophil antibodies Seroconversion with production of Ig. M and Ig. G antigens to EBV ● Treatment: ○ ○ ○ Symptomatic Corticosteroids if airway compromised If Group A Strep grown from tonsils - give Penicillin ● Note: Ampicillin / Amoxicillin may lead to florid maculopapular rash in children with EBV - avoid!

CMV - Cytomegalovirus ● Usually transmitted via saliva, genital secretions, breast milk (rarely blood / placental) ● May result in mononuclear syndrome ● If immunocompromised can cause range of infections ● Treatment: ○ Ganciclovir or Foscarnet - both have bad SE

Slapped Cheek

Slapped Cheek ● Parvovirus B 19 ● Red rash on cheeks (may spread to top of arms) ○ Pallor surrounding mouth / eyes ● Fever - low grade ● Lethargy ● Headache

Bacterial Infections

Scalded Skin Syndrome

Scalded Skin Syndrome ● Cause: Staph Aureus ● Toxin causes syndrome ● Treatment: ○ ○ Admission IV antibiotics ■ Flucloxacillin ● AKA Ritter’s Disease ● Widespread blisters ● Epidermolytic exotoxins cause detachement of epidermal layer

Tropical Infections

NOTIFY PUBLIC HEALTH ENGLAND! Diphtheria

Diphtheria ● ● ● Potentially fatal bacterial infection Severe damage to kidneys, nervous system, heart Cause: Corynebacterium Diphtheriae May be mild or severe Incubation period: 2 -5 days Symptoms: ○ ○ Sore throat Fever (Grey / white patch may develop in throat if severe - can block airway) Lymphadenopathy

Diphtheria ● Complications ○ ○ Myocarditis ■ Abnormal heart rate Inflammation of nerves ■ Paralysis Reduced platelets Renal problems ● Diagnosis ○ Swab throat - culture ● Treatment ○ ○ Diphtheria antitoxin - prevent damage Antibiotics: penicillin / erythromycin ● Fatal in 10% of cases (even with treatment)

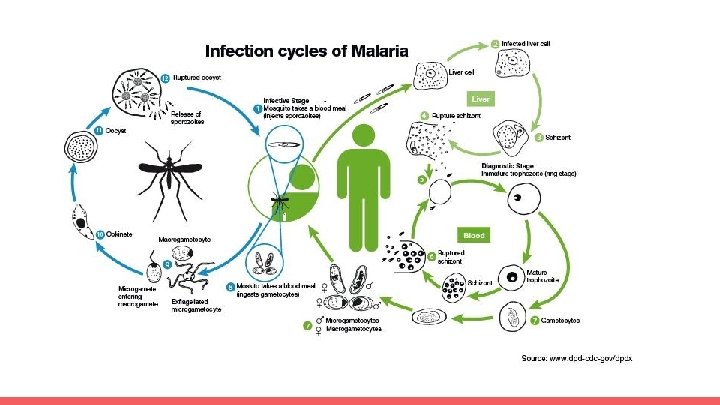
Malaria

Malaria ● Tropical disease ● Spread by female anopheles mosquitoes ○ Parasites come from saliva into human blood → liver → reproduce ● Cause: Plasmodium (falciparum); ovale, malariae, vivax (milder) ● Incubation period: 10 -15 days ● Symptoms: ○ ○ ○ Fever Fatigue Coma Death Seizures ● Treatment: Hydroxychloroquine

TB

Tuberculosis ● Cause: Mycobacterium Tuberculosis ● Droplet spread ● Symptoms: ○ ○ ○ ● ● Cough Night sweats Fever Weight loss Haemoptysis Can be latent or active (10%) Increased relationship between TB and HIV Testing - Mantoux test Vaccine: BCG

TB ● Diagnosis: ○ ○ ○ CXR Culture Mantoux test ● Treatment: ○ ○ ○ Rifampicin (6) Isoniazid (6) Ppyrazinamide (4) Ethambutol (4) (If CNS sparring TB) ● https: //www. nice. org. uk/guidance/ng 33/chapter/Recommendations#latent-tb

Uncommon manifestations

Kawasaki’s Disease

Kawasaki’s Disease ● Pathophysiology ○ Vasulitis ● Cause ○ Unknown - Autoimmune repsonse ● Symptoms: ○ ○ ○ Fever >5 days Genital rash Strawberry tongue Maculopapular rash Lymphadenopathy Rash on hands and feet ■ May begin to peel
 IVIG (IV Immunoglobulin) 2) Aspirin ■ Coronary")
Kawasaki’s Disease ● Treatment ○ ○ 1) IVIG (IV Immunoglobulin) 2) Aspirin ■ Coronary aneurysm risk ● Management ○ ECHOCardiogram

Cardiac Aneurysms ● ECHOs should be performed ● Aspirin given to reduce risk of Coronary aneurysms ● Abnormal dilatations of Coronary Arteries ● Can lead to ischaemic heart disease/ Angina ● Pathophysiology: micro embolisms (clot → occlusion) ● Medicine: anti-platelets ● Surgery: ligation
 A -")
Mnemonics: CRASH ● ● ● C - conjunctivitis R - rash (polymorphous) A - adenopathy (lymph, at least 1) S - strawberry tongue H - hands and feet (swollen and rash)
 Small and medium vessel")
Mnemonics: Warm CREAM (WARM - fever, autoimmune, rash, mucous membranes) Small and medium vessel vasculitis (autoimmune) ● Warm - fever >5 days + 4 of 5 ● Conjunctivitis ● Rash - erythematous, maculopapular ● Erythema (palms and soles) - with swelling ● Adenopathy, cervical - 1 unilateral node ● Mucous membrane - dry, red strawberry tongue Treatment: 1) High dose Aspirin; 2) IVIG Complications: 1) Coronary Artery Aneurysms; 2) Myocarditis → DO AN ECHO

Toxic Shock Syndrome

Toxic Shock Syndrome ● ● ● Toxin producing staph and strp Toxin acts as superantigen Systemic illness High fever, diffuse maculopapular rash, hypotension and shock May include: ○ ○ Redness of mucous membranes Vomiting or diarrhoea Altered consciousness Thrombocytopenia ● 1 -2 weeks after onset, desquamation of palms, soles, fingers ● Areas of infection should be surgically debrided ● IVIG given to neutralise circulating toxin

Rare But Important

NOTIFY PUBLIC HEALTH ENGLAND! Whooping Cough

Pertussis ● ● ● Vaccinated against “ 100 -day cough” Fever, coryza - followed by coughing fits, whoop sound on inspiration May last 10+ weeks May have associated vomiting, broken ribs, fatigue from effort ○ ● ● Babies may not cough but have periods where they do not breath Cause: Bacterium - Bordetella pertussis Airborne disease - droplet spread Infectious from start of symptoms - 3 weeks after coughing fits start Treatment - antibiotics ○ ○ ○ Erythromycin, Azithromycin, Clarithromycin Trimethoprim Sulfamethoxazole

Polio
 ○ ○ Arms, leg")
Polio ● Poliomyelitis ● Cause: Poliovirus ● Muscle weakness (any) ○ ○ Arms, leg Diaphragm ● Feco-oral spread ● Vaccinated against ● Diagnosis: ○ Poliovirus cultured from stool sample / pharynx swab ● Treatment: ○ ○ No cure Relief of symptoms - analgesia, rehabilitation, portable ventilators

HIV

HIV ● Human Immunodeficiency Virus → AIDS ● HIV Virus ● Treated with Antiretrovirals ○ No fully licensed cure ● Passed to child from mother ○ ○ (Unsure if breast milk, intrauterine or delivery) Or Sexually transmitted / through blood products ● Symptoms: ○ ○ Infections Immunosuppression Kaposi's Sarcoma Fatal if left untreated - from other infections

NOTIFY PUBLIC HEALTH ENGLAND! Meningitis

Meningitis ● ● ● ● Acute inflammation of meninges ○ Covering brain and spinal cord Symptoms ○ Fever ○ Neck stiffness ○ Phonophobia / photophobia Viral / bacterial causes Diagnosis ○ Lumbar puncture Treatment ○ Broad spec Abx until causative organism known Brudzinski’s Sign ○ Flexing knees and hips when flexing neck Kernig’s Sign ○ Ben leg, knee at 90 degrees, pain on straightening of knee ■ Meninges or SAH)

Causes Neonates - 3 months Group B Strep E. coli Listeria monocytogenes 1 month - 6 years Neisseria meningitidis Streptococcus pneumoniae Haemophilus influenzae > 6 years Neisseria meningitidis Streptococcus pneumoniae

MENINGOCOCCAL SEPTICAEMIA ● ● ● Meningitis + septicaemia Fatal if untreated Neisseria meningitis most common Bacterial infection (viral causes rarely cause septicaemia) Groups A, B, C, W, X, Y (ACWY vaccine for university students) Management: ○ ○ ABCDE Broad spec antibiotics until culture indicates sensitivity Ben-Pen in community Cyclosporine (e. g. Ceftriaxone / Cefotaxime/ Cefuroxime)

1. 4 Management in secondary care Antibiotics for suspected bacterial meningitis or meningococcal disease 1. 4. 1 Treat children and young people aged 3 months or older with suspected bacterial meningitis without delay using intravenous ceftriaxone. 1. 4. 2 Treat children younger than 3 months with suspected bacterial meningitis without delay using intravenous cefotaxime plus either amoxicillin or ampicillin. 1. 4. 3 Treat suspected meningococcal disease without delay using intravenous ceftriaxone. 1. 4. 4 Treat children and young people with suspected bacterial meningitis who have recently travelled outside the UK or have had prolonged or multiple exposure to antibiotics (within the past 3 months) with vancomycin in addition to the above antibiotics. 1. 4. 5 Where ceftriaxone is used, do not administer it at the same time as calcium-containing infusions. Instead, use cefotaxime[9]. 1. 4. 6 In children younger than 3 months, ceftriaxone may be used as an alternative to cefotaxime (with or without ampicillin or amoxicillin), but be aware that ceftriaxone should not be used in premature babies or in babies with jaundice, hypoalbuminaemia or acidosis as it may exacerbate hyperbilirubinaemia. 1. 4. 7 If tuberculous meningitis is part of the differential diagnosis use antibiotic treatment appropriate for tuberculous meningitis in line with Tuberculosis (NICE clinical guideline 33) (replaced by Tuberculosis [NICE clinical guideline 117]). 1. 4. 8 If herpes simplex meningoencephalitis is part of the differential diagnosis give appropriate antiviral treatment.

Treatment for specific infections in confirmed bacterial meningitis Children and young people aged 3 months or older 1. 4. 9 Treat H influenzae type b meningitis with intravenous ceftriaxone for 10 days in total unless directed otherwise by the results of antibiotic sensitivities. 1. 4. 10 Treat S pneumoniae meningitis with intravenous ceftriaxone for 14 days in total unless directed otherwise by the results of antibiotic sensitivities. Children younger than 3 months 1. 4. 11 Treat Group B streptococcal meningitis with intravenous cefotaxime for at least 14 days. If the clinical course is complicated[10] consider extending the duration of treatment and consulting an expert in paediatric infectious diseases. 1. 4. 12 Treat bacterial meningitis due to L monocytogenes with intravenous amoxicillin or ampicillin for 21 days in total, plus gentamicin for at least the first 7 days. 1. 4. 13 Treat bacterial meningitis due to Gram-negative bacilli with intravenous cefotaxime for at least 21 days unless directed otherwise by the results of antibiotic sensitivities. If the clinical course is complicated[ 10] consider extending the duration of treatment and consulting an expert in paediatric infectious diseases.

Treatment of unconfirmed bacterial meningitis 1. 4. 14 In children and young people aged 3 months or older with unconfirmed, uncomplicated but clinically suspected bacterial meningitis, treat with intravenous ceftriaxone for at least 10 days depending on symptoms and signs and course of the illness. 1. 4. 15 In children younger than 3 months with unconfirmed but clinically suspected bacterial meningitis, treat with cefotaxime plus either ampicillin or amoxicillin for at least 14 days. If the clinical course is complicated[ 10], consider extending the duration of treatment and consulting an expert in paediatric infectious diseases.

NOTIFY PUBLIC HEALTH ENGLAND! Encephalitis
 ● Cuses: ○ ○")
Encephalitis ● Inflammation of the brain (meninges often also affected) ● Cuses: ○ ○ ○ Neurotoxic virus Neuroimmunological response Slow virus infection ● May occur from metabolic abnormality ● Clinical features: ○ ○ ○ Flu like symptoms Behavioural changes Headache, fever ● Causes: ○ Commonly: enteroviruses, respiratory viruses and herpesviruses

Candida

Candida ● ● ● Thrush Itching / soreness Commonly mouth or genitalia White discharge / red inflamed area Fungal infection - treat with antifungals ○ ○ Fluconazole Clotrimazole ■ Topical / pessary / tablet

NOTIFY PUBLIC HEALTH ENGLAND! Scarlet Fever

Scarlet Fever ● ● ● Cause: Group A Strep Incubation period - 1 -4 days Commonly affects 5 -15 yrs age Complications: ○ Glomerulonephritis ○ Rheumatic heart disease ○ Arthritis Diagnosis: ○ Throat culture Treatment: ○ Oral Penicillin VK (10 days) ○ Erythromycin

Scarlet Fever ● Symptoms ○ ○ ○ Rash Strawberry tongue Lymphadenopathy Headache Fever Forschheimer spots ■ Small red transient spots on soft palate ● Rash: ○ ○ Rough Red
")
Coxsackie Disease (Hand, Foot and Mouth)
 Feco-oral transmission Viral infection → hand,")
Coxsackie Disease ● ● Coxsackie Virus (Genus: enterovirus) Feco-oral transmission Viral infection → hand, foot and mouth

Hand, Foot and Mouth ● Coxsackie A 16 ● Symptoms last 1 week ○ ○ ○ Fever Flat, discoloured spots (may blister) ■ Palms, soles of feet, buttocks, lips Fatigue, vomiting, anorexia, irritability ● Incubation 3 -6 days ● Treatment: ○ ○ Supportive Analgesia ● Compilations (rare) ○ ○ Loss of nails Meningitis Encephalitis Flaccid paralysis

Immunodeficiency

Immunosuppression ● Inappropriate immune response ● Many causes ○ ○ ○ Infection: ■ HIV Chronic disease: ■ CF Chromosomal abnormalities: ■ Down's syndrome Medication ■ Steroids Intentional ■ Organ donation
- Slides: 89