Infections of Nervous System Encephalitis Meningitis Encephalitis Severe






 • Headache")

























- Slides: 34
Infections of Nervous System Encephalitis Meningitis
Encephalitis • Severe inflammation of the brain • Usually caused by a mosquito-borne or a tic -borne virus • Can also be caused by: – Ingestion of infected goat’s milk – Accidental injection or inhalation of the virus
Rural Areas • Arboviruses – any virus that is transmitted by arthropod vectors
Urban Areas • Usually caused by enteroviruses – named by their transmission-route through the intestine – often found in the respiratory secretions and stool of an infected person – Types • Coxsackievirus • Echovirus • Poliovirus – Historically, poliomyelitis was the most significant disease caused by an enterovirus
Other viruses implicated • • • Herpesvirus Mumps HIV Adenoviruses Demyelinating diseases following: – Measles – Varicella – Rubella – Vaccination
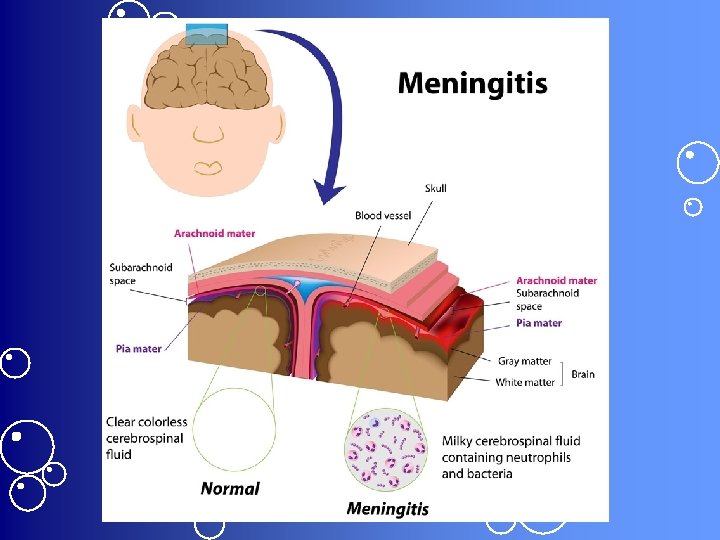
Pathophysiology • Intense lymphocytic infiltration of brain tissues and leptomeninges – arachnoid and pia mater – the two innermost layers of tissue that cover the brain and spinal cord • Leads to: – Cerebral edema, degeneration of the brain’s ganglion cells, & diffuse nerve cell destruction
Signs & Symptoms • Fever of 102 -105 (38. 8 -40. 6) • Headache • Vomiting
Signs of meningeal irritation • Stiff neck • Stiff back
Signs of neuron damage • • • Drowsiness Coma Paralysis Seizures Ataxia Organic psychoses
Diagnostics • CSF or blood analysis to identify the causative virus • Technetium-99 scan may show localized abnormalities • CT scan may disclose localized abnormalities
Treatment • Antiviral agents such as acyclovir • Anticonvulsants to prevent or control seizures • Furosemide or Mannitol to reduce cerebral swelling • Sedative to alleviate restlessness • ASA or Tylenol to relieve headache and reduce fever • Fluids & lytes to prevent dehydration and electrolyte imbalance • Antibiotics for secondary infections
Nursing Actions • • Frequent neuro assessments Monitor I & O Position changes to avoid joint stiffness & neck pain ROM to prevent contractures Darkened room & decreased stimulation Maintain adequate nutrition Reassure patient & family that behavior changes caused by the condition usually disappear Frequent reorientation
Meningitis • Brain & spinal cord become inflamed – Usually d/t bacterial infection • May involve all 3 layers of meninges – Dura mater – Arachnid mater – Pia mater
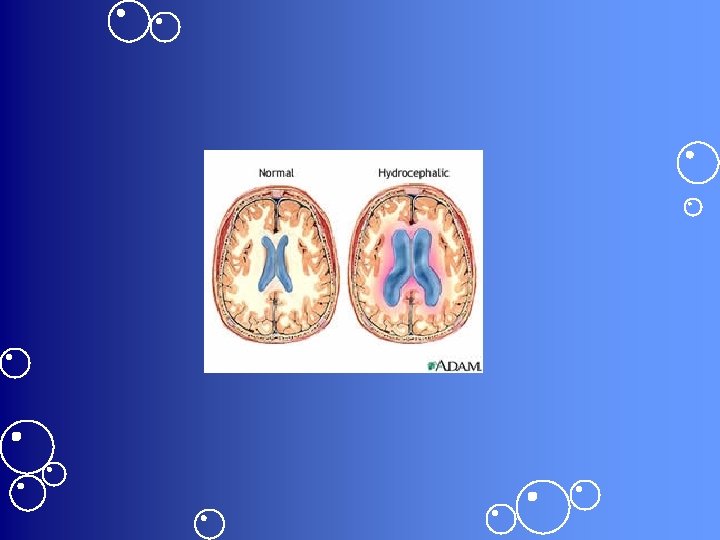
Promptness improves prognosis • If treated early, decreased risk of complications: – Increased ICP – Hydrocephalus – Cerebral infarction – Cranial nerve deficits • Optic neuritis • Deafness – Brain abscess – Seizures or coma
Etiology • Bacteremia – Pneumonia – Empyema – Osteomyelitis – Endocarditis • Aseptic – Virus or other organism • Sometimes no causative organism can be found
Other Infections Associated with Meningitis • • • Sinusitis Otitis media Encephalitis Myelitis Brain abscess – H flu – Strep Pneumonia – E Coli
Any Opening • May follow trauma or invasive procedures – Skull fx – Penetrating head wound – Lumbar puncture – Ventricular shunting
Routes of Entry 1. The blood • Most common 2. A direct opening between the CSF & the environment as a result of trauma 3. Along the cranial and peripheral nerves 4. Through the mouth or nose
Pathophysiology • Invading organism triggers an inflammatory response in the meninges • Neutrophils gather in the area & produce an exudate in the subarachnoid space – Causes the CSF to thicken • CSF flows less readily around the brain & spinal cord – Can block the arachnoid villi & further obstruct CSF flow leading to hydrocephalus
Exudate can also • Exacerbate the inflammatory response – Increases the pressure in the brain • Extend to the cranial and peripheral nerves – Triggering additional inflammation • Irritate the meninges – Disrupting their cell membranes – Causing edema
Consequences of Meningitis • • • Elevated ICP Engorged blood vessels Disrupted cerebral blood supply Possible thrombosis or rupture Cerebral infarction if ICP can’t be reduced Possible encephalitis – Secondary infection of the brain tissue
Aseptic Meningitis • Lymphocytes infiltrate the pia-arachnoid layers but usually not as severely as in bacterial meningitis – No exudate is formed • Makes this type of meningitis, self-limiting
Signs & Symptoms • Fever, chills, & malaise – d/t infection & inflammation • Headache & vomiting • Sometimes papilledema – Inflammation & edema of the optic nerve – Results from increased ICP
Meningococcal • Bacterial meningitis – Characteristic rash
Signs of neuron irritation • Nuchal rigidity • Positive Brudzinski’s & Kernig’s signs • Exaggerated and symmetrical deep tendon reflexes • Opisthotonos – In infants and children
You may also see these • Sinus arrhythmias d/t irritation of autonomic nerves • Irritability d/t increasing ICP • Photophobia, diplopia, and other visual problems d/t cranial nerve irritation • Delirium, deep stupor, & coma d/t increased ICP and cerebral edema
Diagnostics • LP-elevated CSF pressure from obstructed CSF outflow at the arachnoid villi • Cloudy or milky-white CSF • CSF – High protein levels – Positive Gram stain & culture • Cultures of blood, urine, and nose and throat secretions reveal the offending organism
Diagnostics, cont’d • CXR may reveal pneumonitis or lung abscess • Sinus and skull X-rays may identify paranasal sinusitis as the underlying infection or a skull fx as the mechanism for entrance of microorganisms • WBC count reveals leukocytosis
Treatment • • • Antibiotic therapy, usually for 2 weeks Digoxin to control arrhythmia Mannitol to decrease cerebral edema Anticonvulsant to prevent seizures Sedative to reduce restlessness Acetaminophen to relieve headache and fever
Supportive Measures • Bed rest • Fever reduction – Cooling blanket • Isolation if indicated – Family education
Nursing Actions • Frequent neuro assessments • Monitor for deterioration – Temperature increase, decreasing LOC, onset of seizures, altered respirations • Monitor fluid balance • Positioning • Maintain adequate nutrition & elimination • Maintain a quiet environment • Sterile technique for any dressing changes • Administer meds as indicated
Think of appropriate nursing diagnoses for patients with these infections