Infections in Urooncology Patients Dr Bill WONG Queen

Infections in Uro-oncology Patients Dr Bill WONG Queen Elizabeth Hospital Hong Kong


Queen Elizabeth Hospital

Bladder & Prostate Cancer Incidence in Hong Kong Cancer Registry

Bladder Cancer Critical Limits Determining Surgery Ca in-situ Tis Non-invasive papillary Ta Invasion of lamina propria T 1 Invasion of muscle - - - - - T 2 Invades perivesical tissue microscopically T 3 a Invades perivesical tissue macroscopically (w/ mass) T 3 b Invades prostate, uterus or vagina T 4 a Invades pelvic wall or abdominal wall T 4 b LOCAL RESECTION --------- RADICAL RESECTION PALLIATIVE RESECTION
 Lerner, et al")
Bladder Cancer Incidence of Lymph Node Metastases Smith & Whitmore (1981) Lerner, et al (1993) Vieweg, et al (1999) Organ confined p. Tis 0% 1% 10 % p. T 1 5% 13 % 2% p. T 2 13 % 20 % 10 % p. T 3 a 18 % * 24 % 23 % * 42 % 43 % 44 % 45 % 47 % Non organ confined p. T 3 b p. T 4 a+b

Bladder Cancer Radical Cystectomy • • N = 1, 026 Postop mortality = 4 % Overall 5 -yr survival rate = 48 % Significant factors on survival: • Tumour stage • Tumour grade • LN status Histology – squamous, TCC, or adenocarcinoma Ghoneim, et al J Urol 158: 393, 1997 *

Post Cystectomy Urinary Diversion • Cutaneous ureterostomy • Uretero-sigmoidostomy / Rectal bladder • Ileal conduit / Colonic conduit
 Surg Clin N Am 30: 1511,")
Post Cystectomy Urinary Diversion Ileal Conduit (Bricker 1950) Surg Clin N Am 30: 1511, 1950

Urostomy

Ileal Conduit: Long-term Cx Parastomal Hernia

Ileal Conduit Cx: Hydronephrosis Urostomy Clinic, Q E H

Ileal Conduit: Long-term Cx Upper Tract Complications • Obstructive • Ischaemia ureteral stricture • Retroperitoneal fibrosis • Non-obstructive / Reflux • Bacterial colonization of intestinal segment • Ureteral reflux • Chronic pyelonephritis

Pressure Waves in Ileal Conduits

A 5764206 Lo. KC M / 67 19 -6 -87 Ileal conduit 7 -4 -97 Ur = 19. 0; Cr = 195 11 -10 -96 IVU

Post Cystectomy Urinary Diversion • • • Cutaneous ureterostomy Uretero-sigmoidostomy / Rectal bladder Ileal conduit / Colonic conduit Substitution cystoplasty / Orthotopic neobladder Continent cutaneous diversion

Pelvic Cancer Surgery • Ca bladder • Radical total cysto-prostatectomy Radical total cystectomy • Radical total cysto-prostato-urethrectomy Radical total cysto-urethrectomy • Ca cervix - Post radiation recurrence • Salvage pelvic exenteration

Post Cystectomy Continent Diversion Queen Elizabeth Hospital Jan 1991 - Dec 2005 • Orthotopic neobladder • Ca bladder 74 • Leiomyosarcoma of bladder 75 1 • Continent cutaneous diversion • Ca bladder 17 2 had post-RT salvage cystectomy • Ca cervix (post radiation) 6 • Ca urethra 7 30

Post Cystectomy Continent Diversion Queen Elizabeth Hospital Jan 1991 - Dec 2005 • Orthotopic neobladder 75 • 1991 Tubular colonic 2 • 1992 - 1997 Le Bag ileocolonic • 1998 - 2005 T pouch ileal 54 19 • Continent cutaneous diversion • • Kock pouch 2 Le Bag ileocolonic pouch + Mitrofanoff Mansson colonic pouch + Mitrofanoff 12 Native bladder 9 30 7

The Ideal Neobladder • Urine storage & voiding • Adequate capacity, low pressure • Elasticity for voiding / emptying • Protection of upper tract • Absence of reflux • Absence of infected urine

The Ideal Neobladder • Urine storage & voiding • Adequate capacity, low pressure • Elasticity for voiding / emptying • Protection of upper tract • Absence of reflux • Absence of infected urine

The Ideal Neobladder Absence of Reflux
 Uretero-enteric Reimplantation • Florida colonic pouch (n = 190) Technique Tunneled (Anti-reflux)")
Direct (Non-tunneled) Uretero-enteric Reimplantation • Florida colonic pouch (n = 190) Technique Tunneled (Anti-reflux) Direct non-tunneled (Refluxing) No. of ureters Obstruction 30 326 4 13. 3 % 16 4. 9 % Reflux 1 3. 3 % 23 7. 0 % Helal, et al J Urol 150: 835, 1993
 • Submucosal tunnel (Goodwin, Leadbetter)")
Antireflux Ureteral Implantation • Afferent isoperistaltic ileal segment (Studer) • Submucosal tunnel (Goodwin, Leadbetter) Mucosal sulcus (Le Duc) • Split-cuff ureteric nipple (Turner-Warwick) • Afferent ileal nipple valve (Kock) • Serosal-lined extramural tunnel (Abol-Enein)
 BJU 63: 43 -52, 1989")
Ileal Low Pressure Bladder Substitute Studer, et al (1989) BJU 63: 43 -52, 1989
 • Prospectively randomised Antireflux")
Antireflux Nipple or Afferent Tubular Segment Studer, et al (1991) • Prospectively randomised Antireflux nipple Tubular segment n = 20 • Median follow-up 36 months 30 months • Pyelonephtritis 4 2 • With afferent ileal tubular segments, contrast medium could be forced upwards into renal pelvis when bladder substitutes were overfilled. Peristalsis in isoperistaltic segment gradually returned contrast medium back to reservoir. Eur Urol 20: 315, 1991
 Mucosal Sulcus (Le Duc) • Cumbersome technique • Angulation and")
Submucosal Tunnel (Leadbetter, Goodwin) Mucosal Sulcus (Le Duc) • Cumbersome technique • Angulation and kinking

Ileal Nipple Valve • • • * High complexity Nipple ischaemia Nipple stenosis Stone formation Valve prolapse

Refluxing vs Anti-reflux Anastomosis An Experimental Study Refluxing anastomosis Control Anti-reflux anastomosis +ve culture from renal pelvis 7/8 3/9 1/5 Pyelonephritis 6/9 0/9 2/6 (less severe) Kristjansson, et al BJU 78: 840, 1996

The Ideal Technique • Effective • Low complication rate • Easy and reproducible
")
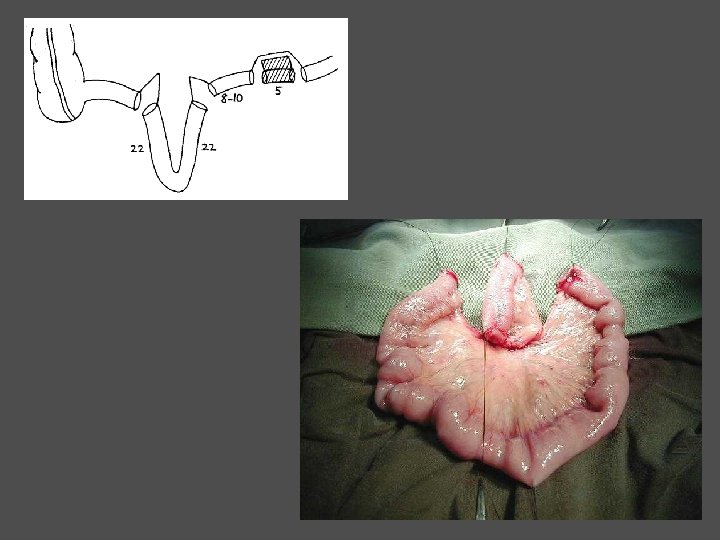
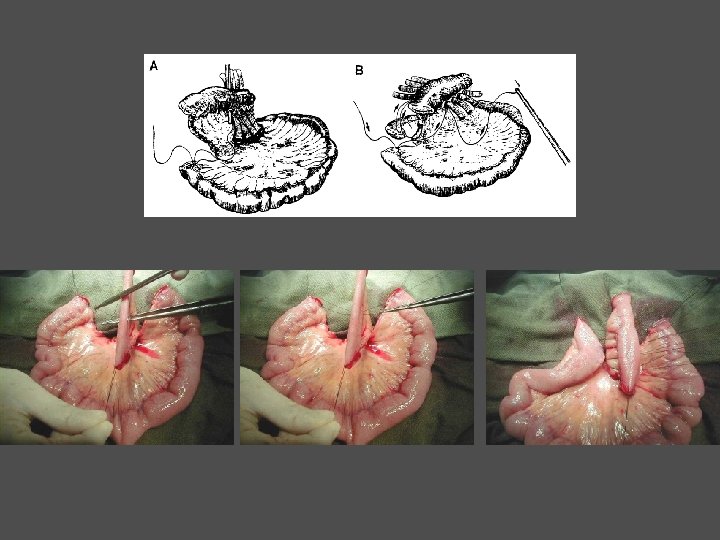
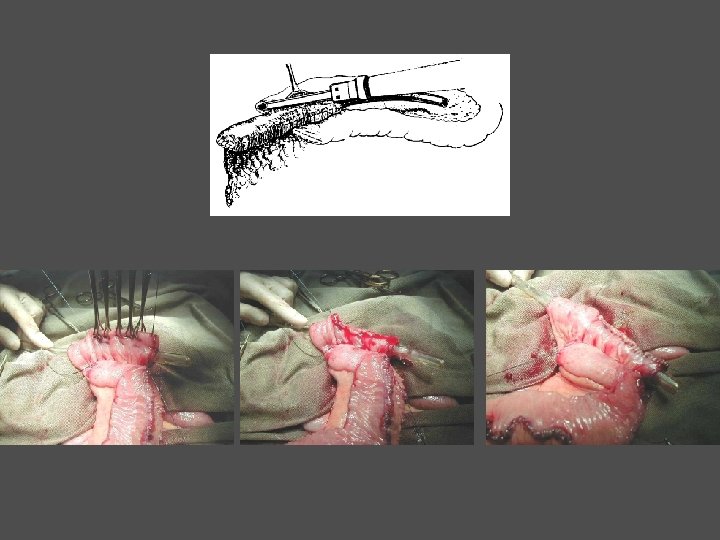
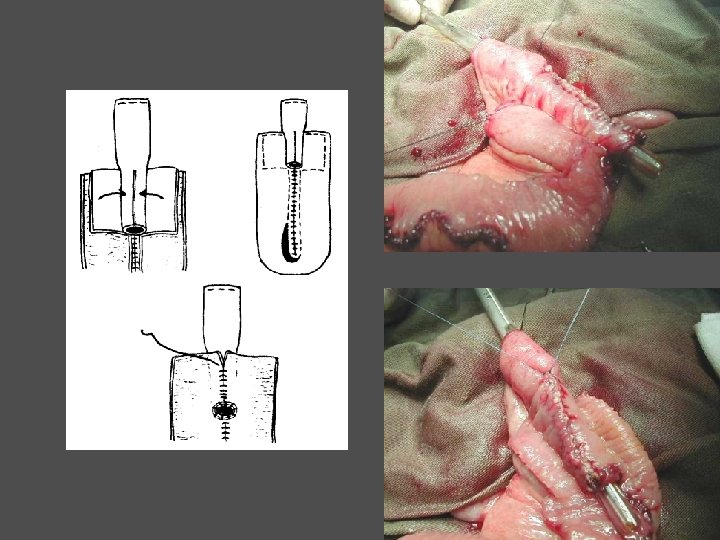
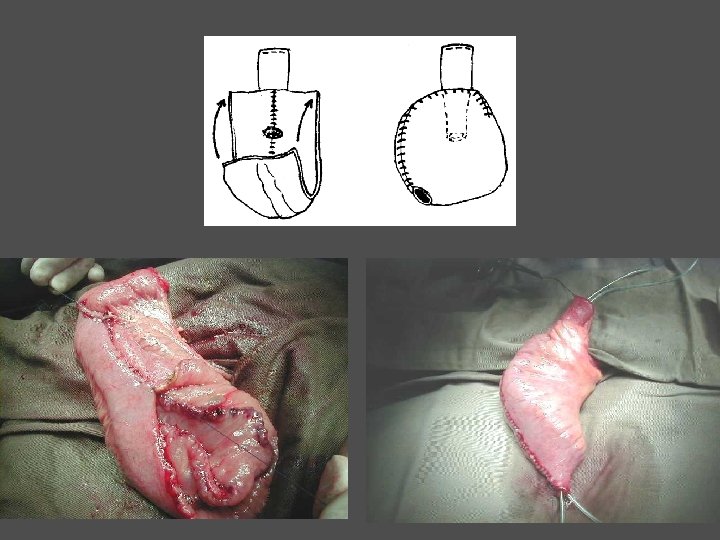
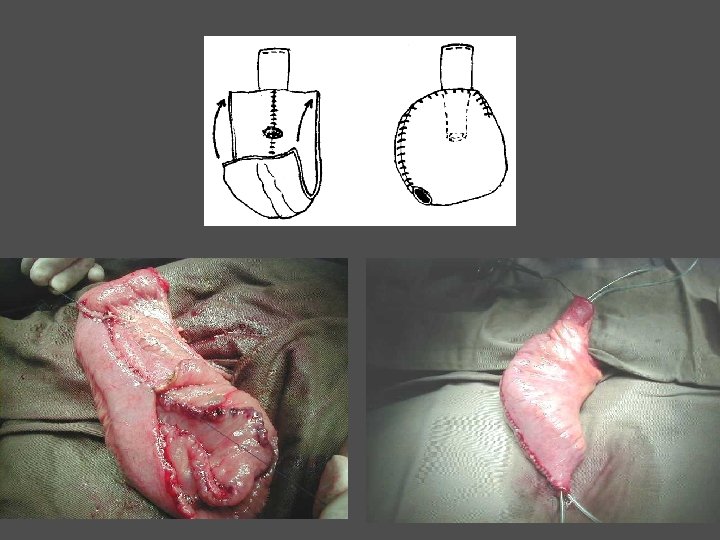
Ileal Neobladder with Serosal Lined Extramural Ileal Tunnel • T pouch DG Skinner (1998) • Serous lined extramural tunnel Abol-Enein (1994)

B 7796701 Wong. K M / 73 T pouch ileal neobladder 10 -12 -98 (post-op 3 weeks) Cystogram

Orthotopic T Pouch Ileal Neobladder Stein, Skinner, et al J Urol 172: 584, 2004 • 209 patients • Median follow-up = 33 (range 0 – 69) months • Reflux (15 / 158) 10 % • Renal function worsened (7 / 181) • 5 had normal upper tract 4%

Orthotopic Ileal T Pouch Reflux n = 31 / 46 • Reflux (demonstrable by VUDS) in 11 / 31 (35 %) • Filling pressure at first reflux mean = 18 cm. H 2 O (range 10 - 39) • Filling volume at first reflux mean = 366 ml (range 250 - 530)

Orthotopic Ileal T Pouch Late Complications N = 46 • • • Diarrhoea Lower urinary tract infection Pyelonephritis Metabolic acidosis Deterioration in renal function 1 4 2 -

The Ideal Neobladder Absence of Infected Urine

Vesico-Ureteric Reflux Cystitis + VUR Pyelonephritis Renal scar / Reflux nephropathy

CIC Clean Intermittent Catheterisation CISC Clean Intermittent Self Catheterisation The insertion of a catheter into the bladder four times or more daily to provide regular and complete bladder evacuation, helps to prevent urinary tract infection and deleterious effects of high intravesical pressure damaging the upper urinary tract. Lapides 1972

Qo. L after Total Cystectomy Voiding Routines Urostomy n = 19 • 5 (26. 3 %) required assistance to - prepare stomahesives - empty urostomy bags Orthotopic Neobladder n = 20 • 18/20 (90 %) resumed urethral voiding 6/18 (33. 3 %) urethral voiders needed supplementary CISC • Only 2 (10 %) totally relied on regular CISC • Only 1 (5 %) required assistance for CIC

Reduce Infected Urine • Clean intermittent self catheterisation • Regular bladder washout

The Ideal Neobladder • Urine storage & voiding • Adequate capacity, low pressure • Elasticity for voiding / emptying • Protection of upper tract • Absence of reflux • Absence of infected urine

The Ideal Neobladder Adequate Capacity

Orthotopic Bladder Substitution Tubular Colonic Neobladder

Colding-Jorgensen et al BJU 72: 586, 1993 Studer et al World J Urol 10: 11, 1992

Orthotopic Bladder Substitution Le Bag Ileocolonic Neobladder

B 2937986 Cheung. AW M / 71 Le Bag ileocolonic neobladder 25 -6 -92 Postop 2 wk cystogram 22 -4 -96 Postop 4 yr VCUG
")
Orthotopic Bladder Substitution Le Bag Ileocolonic Neobladder • ‘Floppy bag’ (capacity > 1000 ml) • Voiding / emptying problem • Infected residual urine • Stone formation

The Ideal Neobladder Effective Voiding / Emptying

Orthotopic Ileal T Pouch Early vs Late Voiding Function N = 46 Early. Late No. reviewed 45 41 • Void by Valsalva 29 29 • Valsalva + CISC for PVR 16 • Mandatory CISC 3 9
 N = 46 Male Female")
Orthotopic Ileal T Pouch Late Voiding Function (>6 mth) N = 46 Male Female No. reviewed 31 10 • Void by Valsalva 24 (77 %) 5 (50%) • Valsalva + CISC for PVR 5 • Mandatory CISC 2 1 4

Orthotopic T Pouch Ileal Neobladder Stein, Skinner, et al J Urol 172: 584, 2004 • 209 patients • Median follow-up = 33 (range 0 – 69) months • Voiding • Complete void 75 % • Intermittent catheterisation • 20 % of men • 43 % of women • Continence • Daytime • Nighttime 87 % 72 % 25 %

K 4334671 Po. WH F / 23 Leiomyosarcoma of bladder 21 -10 -98 T pouch 24 -5 -99 Video-UDS 26 -2 -01 Video-UDS

H 4449683 Yu. CT 19 -7 -00 T pouch ileal neobladder 8 -01 Post cystoplasty - 1 yr

The Ideal Neobladder Reducing Infective / Upper Tract Cx • Urine storage & voiding • Adequate capacity, low pressure • Elasticity for voiding / emptying • Protection of upper tract • Absence of reflux • Absence of infected urine

Urinary Diversion: Outcome Quality of Life 0 1 2 3 4 5 6 Delighted Pleased Mostly satisfied Mixed Mostly dissatisfied Unhappy Terrible Orthotopic neobladder (n = 19) 5 10 2 1 0 0 1 Urostomy (n = 19) 0 7 3 5 0 2 2 QOL Score

Urinary Diversion: Ileal Conduit to Neobladder All patients undergoing cystectomy are candidates for a neobladder and we should identify those in whom orthotopic reconstruction may be less ideal. Hautmann RE J Urol 169: 834 -842, 2003 *

Bladder Cancer Critical Limits Determining Surgery Ca in-situ Tis Non-invasive papillary Ta Invasion of lamina propria T 1 Invasion of muscle - - - - - T 2 Invades perivesical tissue microscopically T 3 a Invades perivesical tissue macroscopically (w/ mass) T 3 b Invades prostate, uterus or vagina T 4 a Invades pelvic wall or abdominal wall T 4 b LOCAL RESECTION --------- RADICAL RESECTION PALLIATIVE RESECTION
 No. of patients")
Superficial Bladder Cancer: TUR & BCG 10 -year Follow-up (MSKCC Study) No. of patients (%) 0– 5 years 5 – 10 years Dead of disease No recurrence 20 (9%) – – – Superficial recurrence 108 ( 49 % ) 84 % 16 % 0. 02 % Tumour progression 93 ( 42 % ) 80 % 20 % 33 % Totals 221 82 % 18 % 15 % Herr et al (1995)
 Tumour stage No.")
Superficial Bladder Cancer: Treated by TUR 20 -year Follow-up (Swedish Study) Tumour stage No. of patients No recurrence Superficial Tumour recurrence progression Ta. G 1 22 27 % 59 % 14 % Ta. G 2, 3 55 31 % 55 % 11 % T 1 G 2 41 19 % 49 % 32 % 22 % T 1 G 3 58 7% 48 % 45 % 36 % Totals 176 20 % 52 % 28 % 22 % Holmang et al J Urol 153: 1823, 1995 Dead of disease

Radical Cystectomy for TCC Kaplan-Meier Cancer-Free Survival Rates 1. 0. 9. 8 T 1 . 7 Cum CFS (%) T 2 . 6. 5. 4 T 3 a . 3. 2. 1 0 T 3 b T 4 Months following surgery –– –– –– T 1 T 2 T 3 a T 3 b T 4 (n = 11) (n = 21) (n = 15) (n = 3)

Bladder Cancer Critical Limits Determining Surgery Ca in-situ Tis Non-invasive papillary Ta Invasion of lamina propria T 1 Invasion of muscle - - - - - T 2 Invades perivesical tissue microscopically T 3 a Invades perivesical tissue macroscopically (w/ mass) T 3 b Invades prostate, uterus or vagina T 4 a Invades pelvic wall or abdominal wall T 4 b LOCAL RESECTION --------- RADICAL RESECTION PALLIATIVE RESECTION

Bladder Cancer Critical Limits Determining Surgery Ca in-situ Tis Non-invasive papillary Ta Invasion of lamina propria - - - T 1 --------- Invasion of muscle - - - - - T 2 --------- Invades perivesical tissue microscopically T 3 a Invades perivesical tissue macroscopically (w/ mass) T 3 b Invades prostate, uterus or vagina T 4 a Invades pelvic wall or abdominal wall T 4 b LOCAL RESECTION RADICAL RESECTION PALLIATIVE RESECTION

Radical Cystectomy • Prognostic implications of the pathology are well appreciated • Bladders can be safely removed • Local control rates are excellent • Orthotopic bladder replacement is the option for most men and women
- Slides: 69