Infection Prevention Control Drs Induction Infection Prevention Control

















 score ‘epic 3: National Evidenced-Based Guidelines for Preventing Healthcare. Associated")




- Slides: 27
Infection Prevention & Control Dr’s Induction Infection Prevention & Control Team
To protect staff and patients from Hospital Acquired Infections, follow these general principles Waste disposal Blood/body fluids spillage Sharps safety Standard Infection Control Precautions Linen handling Do not share creams, lotions, gels etc. Personal Protective Equipment (PPE) Keep cuts covered Hand hygiene Decontamination of equipment & environment
Hand Hygiene • Routine hand hygiene – 2 methods available • Hand washing – Hands are visibly soiled – Any diarrhoeal case – ‘When you feel the need to wash your hands’ • Foaming alcohol hand rub – Visibly clean hands – Bare Below The Elbows Policy B
Standard Precautions & PPE • ASSESS THE RISK of exposure to body substances or contaminated surfaces BEFORE any health-care activity. Make this a routine! • ITS NOT ONLY GLOVES & APRON – THINK & assess the activity you’re undertaking • Ask yourself – Could my hands become contaminated? – Could my uniform become contaminated? – Is there a risk of splashing/spraying to my face or eyes?
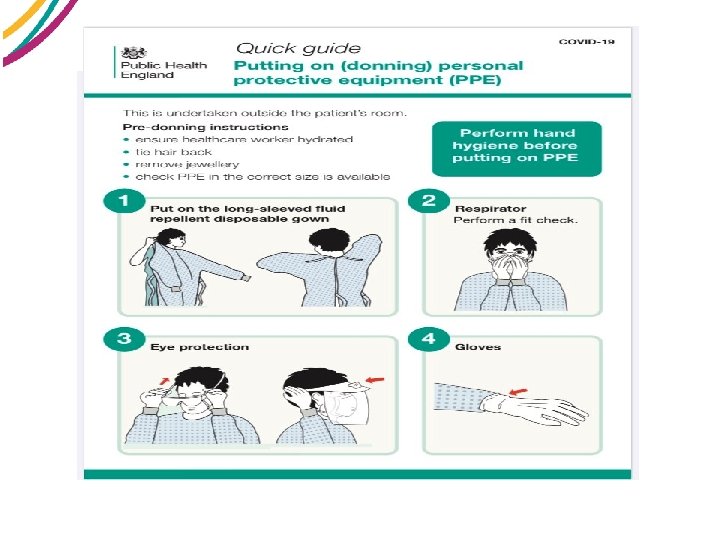
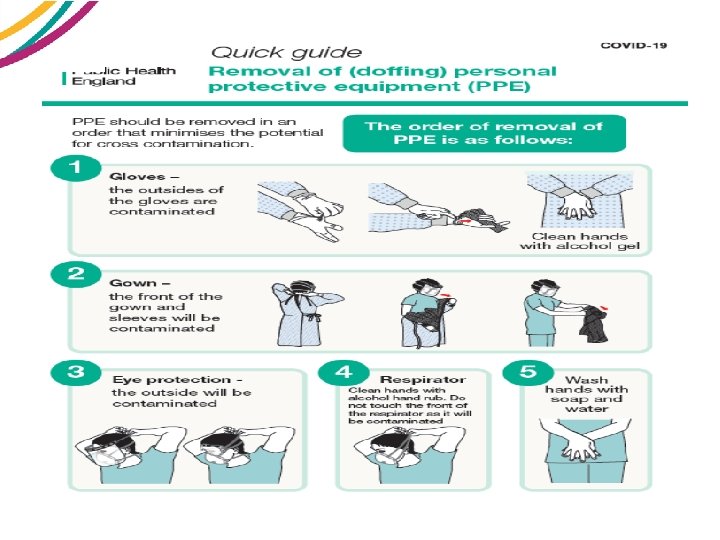
PPE
Further guidance
Decontamination of Equipment / Environment Contaminated with: VRE 85%!!! Contaminated with? ? • Coag-neg Staph • Staph aureus • Pseudomonas Contaminated with: faecal organisms and MRSA 1 in 6 of mobiles Contaminated with: faecal organisms • VRE • C. difficile
Sharps safety Dispose of sharps at the point of use! You use it … You bin it! What to do in case of sharps injuries………… Bleed it Wash it Cover it Report it Attend Occupational Health (A&E out of hours)
Disposal of Waste Black Domestic Waste, may be landfilled / recycled • • Orange Infectious waste, heated treated to render safe prior to disposal Yellow Infectious waste, must be incinerated Purple Cytotoxic waste, must be incinerated by licensed facility Blue Confidential waste Legal requirement to dispose of waste correctly Clinical (Infectious) waste 3 ½ times more expensive than domestic waste
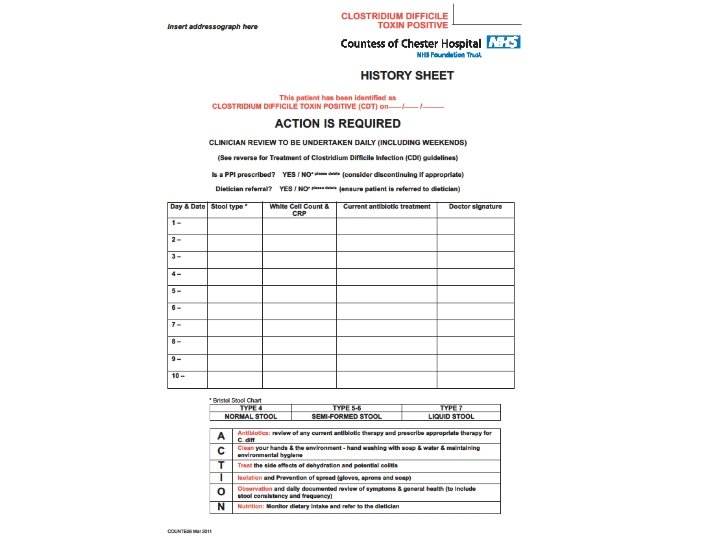
FIGURE 1. CDI TREATMENT ALGORITHM
Key learning from C. difficile RCAs 2018 -19 • • • Fewer MFFD developing CDI Ages more in line with expected age range Range of clinical areas & Consultant teams Fewer patients with LOS over 3 weeks Fewer total antibiotic exposures than 2017/18
Key areas to consider 2018 -19 • 50% isolated at onset of diarrhoea • 63% on PPI prior to onset • Main indication for antibiotic prescription: - 30% respiratory - 30% sepsis - 23% urinary tract • 30% of patients MFFD prior to onset • 11% of antibiotics unnecessary
MRSA BACTERAEMIA
Easy as 1…. . 2…. . 3…. ? • SCREEN……… • IDENTIFY – Early identification of MRSA carriage results in improved patient management ERADICATE – Commence appropriate therapy (topical +/- systemic) PREVENT SPREAD – Routine & consistent adherence to all infection prevention & control practice • •
MRSA Bacteraemia 2019 -20 CASE 1 - June 2019 • In hospital for 106 days – then MRSA positive blood culture • 5 opportunities missed to collect an MRSA screen • Subsequently screened MRSA positive nose, groin and catheter • Patient already deceased • Cause of death – – 1 a) Sepsis with Methicillin Resistant Staphylococcus Aureus b) Discitis at L 2/L 3 level – 2) Congestive Cardiac Failure o v A e l b a d i
MRSA Bacteraemia 2019 -20 CASE 2 - October 2019 • Nursing admission assessment not undertaken – Admitted via GPU • MRSA admission screen not collected • VIP score recording inconsistent e l b a d i o v A CASE 3 - December 2019 • Known MRSA colonised • Developed phlebitis post cannula removal • Antibiotic treatment did not cover for MRSA • Nursing admission assessment, screening (nose & throat) • Decolonisation (variance from 1 st line treatment) • Cannula insertion documentation / VIP monitoring o v A e l b ida
What we’ve learnt from previous MRSA bacteraemia cases
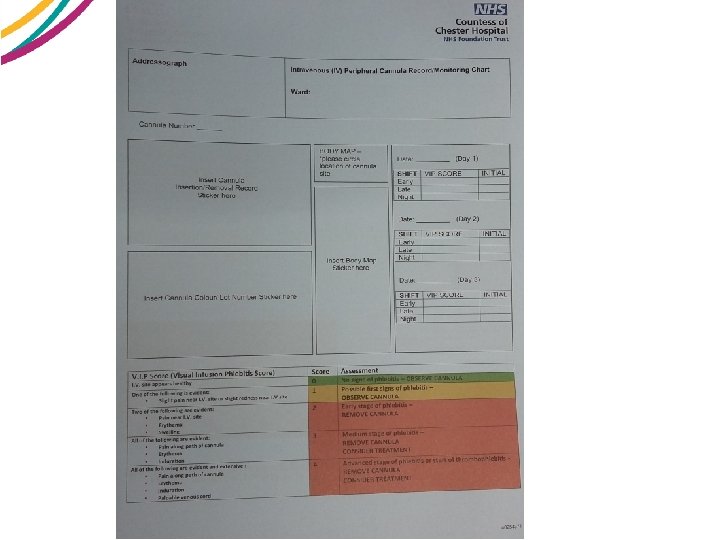
Visual Infusion Phlebitis (VIP) score ‘epic 3: National Evidenced-Based Guidelines for Preventing Healthcare. Associated infections in NHS Hospitals in England (2014)’ ‘NICE: Pathway – Preventing infection to vascular access devices (2017)’
Antimicrobial resistance – the ‘ticking time bomb’ • • • ESBL’s – – Extended spectrum beta lactamases CPE – – Carbapenamase-producing Enterobacteriaceae VRE – – Vancomycin-resistant Enterococcus MRSA – – Methicillin Resistant Staphylococcus aureus VRSA – – Vancomycin-resistant Staphylococcus aureus Linezolid resistance Daptomycin resistance Colistin resistance Pan-resistant Acinetobacter Baumannii
‘Start Smart - Then Focus’ Antimicrobial Stewardship Toolkit for English Hospitals • Start Smart – – Clear evidence of infection – Prompt treatment in severe sepsis/life threatening – Documentation / Indication / Duration / Review – Microbiology cultures
Start Smart - Then Focus Antimicrobial Stewardship Toolkit for English Hospitals • Then Focus – – Stop – Switch (IV to oral) – Change (narrower spectrum) – If continuing – stop/review date – OPAT (Hospital @ Home)
And finally………. • Remember Infection Prevention and Control is Everybody’s Responsibility • Infection control MUST be an integral part of all clinical tasks not an optional ‘add on’. • Contact Information – Infection Prevention and Control Team – Mon-Fri 9 am-5 pm Ext 6758, Bleep 2754 – Out of hours – Consultant Microbiologist via Switchboard