Infection Control Workshop Dr Brittney Jones DPM Dr

Infection Control Workshop Dr. Brittney Jones DPM Dr. Cory Jacoby DPM Midwest Podiatry Conference 2017

Outline • • • CDC/OSHEA recs Office Protocols Infection 101 Podiatry based infections Workshop: • Sterile Gloves • Sterile Gowns • Sharps

Infection Terms • MRSA: Methicillin-resistant Staphlococcus Aureus • Gram positive cocci bacteria • On susceptibility tests negative to oxacillin • Antibiotic options: Clindamycin, Bactrim, Doxycycline, Linezolid, Vancomycin, tigacyline • Ca-MRSA is community acquired and Ha-MRSA is hospital acquired • VRE: Vancomycin-resistant Enterococcus • Found in the intestine and female genital tract • ESBL: Extended Spectrum Beta-Lactamases • Commonly E. coli or Klebsiella • Resistant to penicillins and cephalosporins • Hospital aquired UTI most common but can be cause other infections in the immunocompromised
 with")
Infection Terms • C. Diff: Clostridium difficile • Causes severe colitis (colon irriitation) with watery diarrhea, fever, loss of appetite, nausea • Transferred via spores which can live for long periods of time on surfaces • Common treatments of IV Flagyl or oral Vanc • • HAI: Hospital acquired infections Cellulitis: Infection of skin and underlying soft tissues Osteomyelitis: Infection of bone SIRS: Septic inflammatory response sydrome includes • Criteria are HR, Temp, WBC, Respiratory Rate Sepsis: SIRS in the presence of infection

Infection Terms • Bacteria: Single cell organisms • • They are prokaryotic Can be Gram + or Gram – Can be multiple shapes, commonly cocci or bacillus Treated with anti-biotics or natural immunity • Viruses: Infectious agent that replcates within host cell • Treated with anti-virals or natural immunity • Common Viruses: HIV, HPV, Influenza • Fungus, molds, yeasts: Eukaryotic organisms

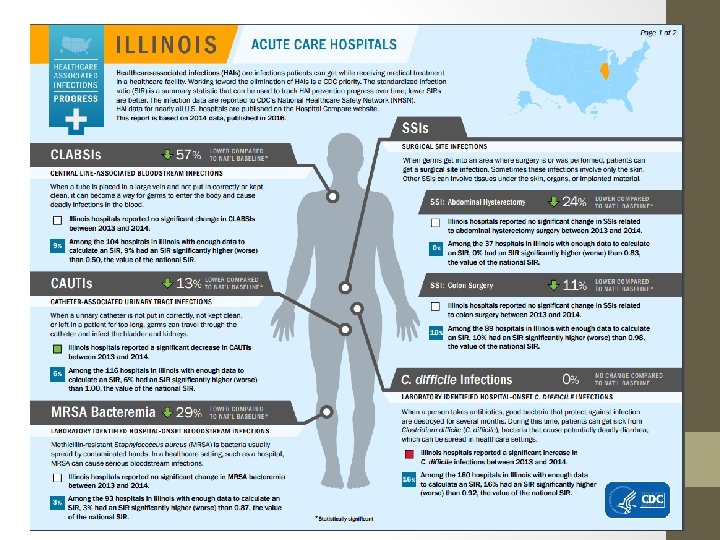
Common Infections Seen by Podiatrist In the Podiatry Office Cellulitis Osteomyelitis Post-Operative Infections Drug resistant infections (VRE, ESBL, MRSA) • Systemic illness not related to foot (Flu, GI distress, C. diff, ect) • Blood Borne Pathogens (HAV, HBV, ect. ) • • Hospital Based • Central line associated blood infections • Catheter associated UTI • MRSA bacteremia • Surgical site Infection • C. difficile Infections • Airborn/Droplet (TB) • Drug resistant local infection (VRE, ESBL, MRSA) • Blood Borne Pathogens (HIV, HBV)

Local Signs of Infection • 4 Classic Signs of Inflammation: • • Rubor: Redness Calor: Heat Tumor: Swelling Dolor: Pain • Purulent Drainage • Mal odor


Systemic signs of infection • • Fever/Chills Nausea/Vommiting Increased blood sugars Increased While Blood Cell count > 12000 cells/mm^3 Increased Inflammatory Markers (ESR, CRP) Increased Heart Rate and Respiratory Rate Blood pressure can be increased in infection though can drop when in sepsis
 considered an infection of the incision")
Post Operative Infection • Surgical site infection (SSI) considered an infection of the incision site within 30 days of surgery or 1 year of an implant • SSI incidence is 2. 55% annually • Higher in trauma cases than elective cases • High incidence >55 years old • Higher incidence in immunocompromised • Higher with increased ASA score over 1

Post-Operative Infections • Can be superficial and involve only skin 5 weeks post-op 6 weeks post-op after 1 week of antibiotics

Post-Operative Infections • Can be deep and involve bone and/or hardware • This often requires major intervention • Long term antibiotics • Removal of hardware • Revision surgery

Why is this an issue? • Infections of the foot and ankle can lead to loss of limb or life • Post-operative infections and hospital based infections are often preventable and pose risks to patient overall health • SSI infections decrease patient satisfaction • SSI lead to longer hospital stays • Annual cost of SSI estimated at 10 billion • Annual deaths of SSI estimated at 8000

• In 1992 the annual direct costs for hospital acquired infections was 4. 5 billion dollars • In 2007 the annual direct costs for HAI ranges from 28. 4 billion – 45 billion dollars based on CPI adjustment models • Epidemiology of infections is changing and price of treatments inflating Douglas Scott II, R. "Direct Medical Costs. " Encyclopedia of Public Health (n. d. ): 267. Why is this an issue?

Infection Control • As podiatrists and podiatric assistants we must aim to prevent and control lower extremity infections • Today we are also focusing on systemic infection control and ways to prevent the spread of disease • Being proactive and educated is a major factor in infection control and prevention

Goal is prevention • The goal is to follow proper office protocols to prevent infections. • This includes proper room cleaning, sharps management, glove use, instrument use/turnover/cleaning

Goal is prevention • Even with perfect technique and protocols, infections will still happen. • Secondary goal is early identification of infection to lead to early treatment and reduction of complications • If you see something, say something

Disease Transmission

Disease Transmission • As health care providers we most protect ourselves and our patients considering all possibilities of infection transmission in our offices • • • Patient to another patient Patient to the community Patient to a health care provider Health care provider to a patient Patient to themselves (Consider spread of warts from one foot location to another)

At Risk Patients • Immunocompromised • • Diabetes HIV Cancer/Chemotherapy Medications: e. g. Methotrexate, long term steroid use

At Risk Patients • Non-vaccinated: By choice or medically unable to vaccinate • Children? Child with open growth plates who developed a hematogenous infection

We DO NOT only treat feet • Patient’s are more than just their feet • As health care professionals we are responsible for helping control spread of all infectious disease • This includes influenza, c. diff, blood born pathogens • Patients cough in our waiting rooms • Patients bleed in our offices • We obtain a detailed medical history, not just a chief complaint. This includes a review of systems.

Hand Washing • CDC has a 56 page “Guideline for Hand Hygiene in Health-Care Settings” • Moral of the story: Hand washing reduced infection spread

Hand Washing Alcohol Based Soap and Water > 15 seconds • Faster • Often more accessible • More efficient at killing most bacteria • Cases less dryness than frequent soap and water • Work via denaturing proteins • Does not kill Clostridium difficile spores • More time consuming • Higher bacteria count post cleaning than alcohol based • Removes debris • Effective in removing C. Diff spores reducing spread.

Hand Washing • Chlorhexidine: Effective against many viruses but not against spores • Iodine Based: Have bactericidal activity against most bacteria and many spores including c. diff • 25% nurses relate to some level of dermatitis due to hand washing • Allergic contact dermatitis can be associated with hand hygiene products

Thank you • Questions • Take a short break and then we will work hands on with gloves, gowns and sharps with goals being to learn to reduce the spread of infection.

Work Cited • Douglas Scott II, R. "Direct Medical Costs. " Encyclopedia of Public Health (n. d. ): 267. • Cdc. CDC_IC_Assessment_Tool_Outpatient_v 2_3 (n. d. ): n. pag. CDC. Web. 25 Apr. 2017. • "Guideline for Hand Hygiene in Health-Care Settings. " Psyc. EXTRA Dataset (n. d. ): n. pag. Web. 25 Apr. 2017. • Al-Mulhim, Fahad A. , Mohammed A. Baragbah, Mir Sadat-Ali, Abdallah S. Alomran, and Md Q. Azam. "Prevalence of Surgical Site Infection in Orthopedic Surgery: A 5 -year Analysis. " International Surgery. The International College of Surgeons, World Federation of General Surgeons and Surgical Specialists, Inc. , 2014. Web. 26 Apr. 2017. • Centers for Disease Control and Prevention, 17 Apr. 2017. Web. 26 Apr. 2017.
- Slides: 28