Indications of Blood Therapy Low O 2 carrying
 LOCC & low blood")
Indications of Blood Therapy Low O 2 carrying capacity (LOCC) LOCC & low blood volume Bleeding due to coagulopathy
 Cryoprecipitate Cryopoor plasma (CPP) Factor concentrate")
BLOOD PRODUCTS ♦Blood-plasma products Fresh Frozen Plasma (FFP) Cryoprecipitate Cryopoor plasma (CPP) Factor concentrate (VIII, IX) Albumin Immune globulins

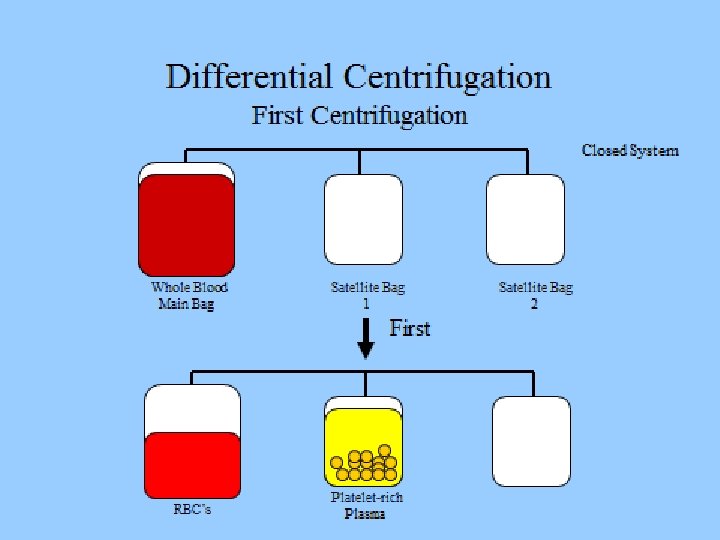
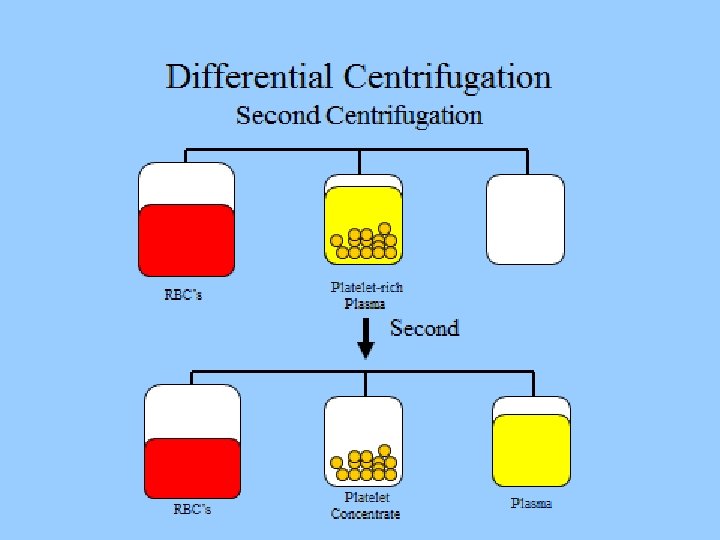
Blood product preparation

Blood product preparation PLT PRBC FFP
")
FRESH FROZEN PLASMA (FFP)

FFP: FFP preparation

FFP: FFP preparation
 • • • prepared by removing plasma from W.")
FFP: Fresh Frozen Plasma (FFP) • • • prepared by removing plasma from W. B within 8 h of collection. 200 -250 ml Stored at – 30ºC or below for 2 years / -20 to -25 ºC for 1 year Contains : Water, carbohydrates, fats, minerals albumin, clotting factors(all labile & stable clotting fx), immunoglobulin, antithrombin Each unit of FFP increases the level of each clotting fx by 2 -3% in adults.
 • Thaw at 37 ºC & use within 4")
FFP: Fresh Frozen Plasma (FFP) • Thaw at 37 ºC & use within 4 h , if not used keep at 2 -6 ºC for 24 h • transfusion rate: adults= 200 -300 ml/h or 4 ml/min child. = 60 -120 ml/h • Transfuse by filter (170 -260 micron)
-Indications • Coagulopathy due to multiple factor deficiencies • Corrections")
FFP: Fresh Frozen Plasma (FFP)-Indications • Coagulopathy due to multiple factor deficiencies • Corrections of known congenital or acquired coagulation factor deficiencies(e. g. , factors II, V, VII, X, XI, or XIII) in patients with hemorrhage • Urgent reversal of warfarin effect • Treatment of microvascular hemorrhage in the presence of prolonged PT, a. PTT (> 1. 5 x normal) • Treatment of microvascular bleeding following massive blood transfusion when timely reporting of laboratory test result is not available • Plasma exchange for TTP
-Contraindications Plasma should not be used: - as a volume")
FFP: Fresh Frozen Plasma (FFP)-Contraindications Plasma should not be used: - as a volume expander or as a nutritional supplement - as albumin supplementation - for correction of hypogammaglobulinemia - for treatment of hemophilia or von Willebrand disease or other congenital procoagulant and anticoagulant factor deficiency where virally inactivated or recombinant factor concentrates are preferred - to treat bleeding alone or prolonged PT or PTT alone
 • Therapeutic dose : 10 -20 ml/kg to correct")
FFP: Fresh Frozen Plasma (FFP) • Therapeutic dose : 10 -20 ml/kg to correct clotting factors 5 -7 ml/kg to reverse warfarin effect

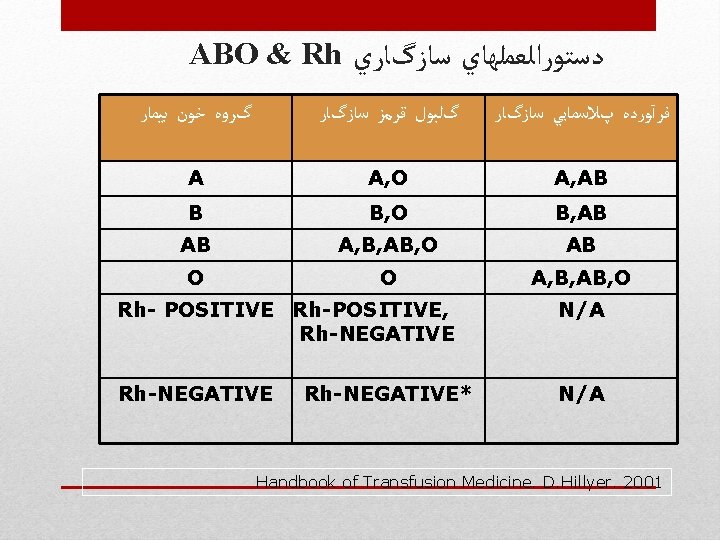
FFP: Patient and donor plasma selection by ABO Recipient O A B AB Donor O, A, B, AB A, AB B, AB AB

CRYOPRECIPITATE &CPP

CRYOPRECIPITATE: Cryoprecipitate • • Vol= 15 ml The cold-insoluble portion of plasma that remains after FFP has been thawed at 1 -6 º C Use as soon as prepared / freeze Stored at -30ºC or below for 2 years / -20 to -25 ºC for 1 year

CRYOPRECIPITATE: Cryoprecipitate • • Thaw at 37ºC, kept max. 6 h. at room temp. Factor VIII decrease: 1 st h. 10% 4 h. 20% 6 h. 30% hence for Factor VIII replacement use within 4 h. of thawing • Transfusion rate: 5 ml/min

CRYOPRECIPITATE: Cryoprecipitate • Contains: – – – Factor VIII: C = 80 -120 U Factor VIII: v. WF = 70 -80 U Factor XIII = 40 -60 U Fibrinogen = 150 -250 mg Fibronectin = 30 -60 mg About 10 -15 ml of plasma • Dose: 1 U/ 5 -10 kg in hypofibrinogenemia
 Hemophillia A")
CRYOPRECIPITATE: Cryoprecipitate-Indications • • • von Willebrand’s disease (if concentrate not available) Hemophillia A (if concentrate not available) Factor XIII def. Cong. /acquired fibrinogen def. Uremic bleeding (DDAVP prefered) fibrin glue
 • 200 -250 ml = cryoprecipitate reduced • Contains:")
CRYOPOOR PLASMA: Cryopoor plasma (CPP) • 200 -250 ml = cryoprecipitate reduced • Contains: very low level of fibrinogen, factor. VIII and von Willebrand factor but enough of other factors • Usage: treatment TTP

PLATELET PRODUCTION & STORAGE

PLATELET: Random donor Platelets

PLATELET: Random donor Platelets

PLATELET: Random donor Platelets

PLATELET: Random donor Platelets • ≤ 5. 5 x 1010 platelet in 50 -70 ml of plasma • Each unit of plt. expected to increase 5000 -10000 plt.

PLATELET:

Apheresis

PLATELET: Single donor platelet • • Plateletphresis ≤ 3 x 1011 platelet in 300 ml of plasma Stored at 20 -24ºC in shaker incubator Each unit of plateletphresis unit increase plt. 30000 -60000. ( 1 U random plt expected to increase 5000 -10000 plt) • Equals 6 random platelet • Decrease donor exposure(safety)

PLATELET: Pooled leukoreduced platelet • • 5 -6 random platelet pooled in a close system Stored at 20 -24ºC for 3 days Benefit: leukoreduced Implication: - prevent alloimmunization - to minimize transmission of viral disease such as CMV

PLATELET: Platelet transfusion-indication • Prophylaxis in otherwise healthy man • Treatment of patient on Chemotherapy • Treatment of patient with fever, infection or antiplatelet therapy • Treatment of patient with mucosal bleeding • Treatment of surgical patient • Bleeding in patients with thrombocytopenia or functional platelet abnormality • After massive transfusion(RBC) and thrombocytopenia • Cardiac surgery with extracorporeal circulation

PLATELET: • Thrombocytopenia • • <10, 000 in uncomplicated patients <20, 000 if febrile or septic <50, 000 if bleeding or undergoing major surgery <100, 000 for neurosurgery or ophthalmologic procedures • Thrombocytopathy • Congenital defects • Drugs (ASA, Plavix) • External agents (cardiac bypass or ECMO)
 ITP (relative contraindication) Uremia-related platelet dysfunction")
PLATELET: Contraindications • • TTP/HUS Heparin-induced thrombocytopenia (HIT) ITP (relative contraindication) Uremia-related platelet dysfunction • DDAVP • Cryoprecipitate • RBC transfusion (keep HCT > 30%)

PLATELET: Dosage: • Adult dose: 1 random platelet unit/ 10 kg wt. (one dose=5 or more units of random platelets) • Child: 5 -10 ml/kg increases platelet count by 50000100000
 ×")
PLATELET: Response evaluation to platelet transfusion: * CCI = (P 1 -P 0) × BSA (m 2) no. Platelet transfused × *Corrected count increment 10 11

PLATELET: Response Evaluation: • CCI must be at least 7500 one hour and 4500 , 20 hours after transfusion. • So if it doesn’t occur we can say that patient has platelet resistance.

PLATELET: Causes of platelet resistance: 1. Fever. 2. Sepsis. 3. Splenomegaly. 4. DIC. 5. Post BMT. 6. Drugs (Amphotricin) 7. Alloimmunization.
 • • •")
PLATELET: Failure of expected platelet increment • Consumption (after 24 hours) • • • Fever Infection Drugs (Amphotericin) Bleeding Hepatosplenomegaly DIC • Anti-HLA or platelet-antigen antibodies (after 10 -60 minutes)

PLATELET: Modified Platelet Units • Leukocyte-reduced platelets • Irradiated

PLATELET: • Rh negative patients should receive negative platelet especially women in reproductive age and children if not use Rh immunoglobulin • Use transfusion set for infusion • Transfuse pooled platelets within 4 hr. • Notice: bacterial contamination

RBC:

PLASMA: plasma Yes No No Yes Yes Yes No No No Yes

Principles of Transfusion • Right blood • Right patient • Right reason • Right test • Right dose • Right time

ATTENTION • The most logical approach to reducing the risk of transfusion is only to use blood when it is strictly clinically necessary and there is no alternative • Ref= ABC of transfusion

- Slides: 50