Indication and Contraindications for Intervention in TEVAR Type


















 Renal (17) 6 (21%) 2 (7%) 3 (10%)")
 Mesenteric (N=18; 62%) # of patients Presentation Abdominal pain Ileus, abdominal")
 # of")
 Vessel #")

 Presentation # of Patients % Chest/back pain 23 95. 8 Hemothorax/Contained")
 Device characteristics # of Devices")
 Stroke Transient paraparesis")







- Slides: 34
Indication and Contraindications for Intervention in TEVAR Type B Dissection Edward Woo Associate Professor Vice Chief/Program Director Division of Vascular Surgery and Endovascular Therapy University of Pennsylvania Health System Department of Surgery, University of Pennsylvania Health System
Disclosures § Medtronic, Cook, Gore, Atrium Department of Surgery, University of Pennsylvania Health System
Acute Type B Aortic Dissection § Incidence: 2. 6 -3. 5 per 100, 000 patient-year § Uncomplicated § Complicated – Malperfusion – Rupture Department of Surgery, University of Pennsylvania Health System
Uncomplicated § Incidental finding § Pain that resolves § Why treat – Fix dissection – Aneurysmal enlargement § Why not treat – Complications of intervention Department of Surgery, University of Pennsylvania Health System
Department of Surgery, University of Pennsylvania Health System
TEVAR demonstrating improved results after 3 yrs INSTEAD trial-Nienaber Veith Symposium 2011 Department of Surgery, University of Pennsylvania Health System
Complicated § Complicated type B dissection – Malperfusion – Rupture § Significant Morbidity and Mortality if not treated – Prior treatment options-poor results » Fenestration » Open repair Department of Surgery, University of Pennsylvania Health System
TEVAR and Acute Complicated Type B Dissection: A New Surgical Paradigm § Surgical management of acute complicated type B aortic dissection is associated with significant morbidity and mortality – Open Surgical repair has a mortality ranging from 21%-50% (22. 5% in Bozinovski et al. Annals of Thoracic Surgery 2008) § Medical management is also associated with poor outcome – In hospital mortality 19% (Estrera et al. Circulation 2006) § Is TEVAR the new paradigm Department of Surgery, University of Pennsylvania Health System
Acute Type B and Malperfusion Mechanism § Dynamic – – § Pressurization of false lumen and mobile dissection flap Leads to narrowing or occlusion of true lumen Dynamic process Degree of malperfusion relates to degree of compression Compromised perfusion to end organ Static – Dissection extends into branch vessel – Narrows branch vessel – Creates a fixed obstruction § Combination Department of Surgery, University of Pennsylvania Health System
IVUS-Dynamic Compression Department of Surgery, University of Pennsylvania Health System
Treatment § Aortic endograft – Cover proximal entry tear – Distal degree of extension determined by repressurization of true lumen and restoration of visceral perfusion § Possible adjunctive stenting Department of Surgery, University of Pennsylvania Health System
Reexpansion of True lumen Department of Surgery, University of Pennsylvania Health System
IVUS-post TEVAR Department of Surgery, University of Pennsylvania Health System
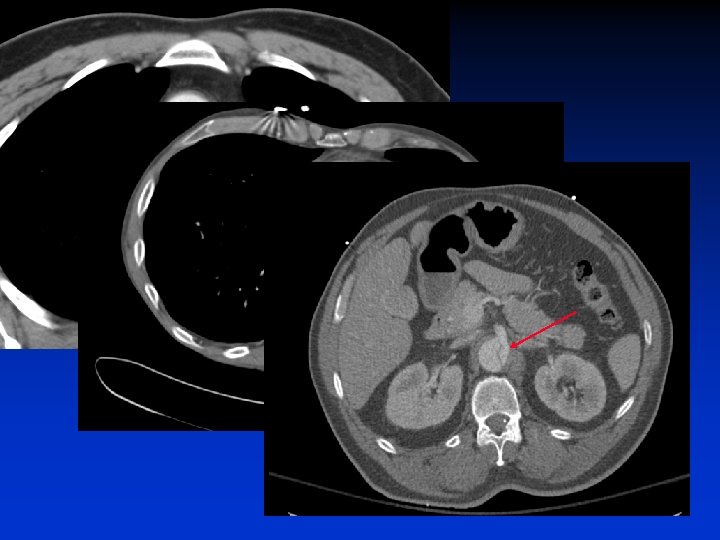
Static Obstruction Department of Surgery, University of Pennsylvania Health System
Treatment § TEVAR – Seal entry tear – Expand true lumen-if necessary § Adjunctive stenting! Department of Surgery, University of Pennsylvania Health System
Static-Angio Department of Surgery, University of Pennsylvania Health System
Adjunctive Stent Department of Surgery, University of Pennsylvania Health System
F/U CTA Department of Surgery, University of Pennsylvania Health System
Malperfusion Patterns-Results at PENN Mesenteric (18) Renal (17) 6 (21%) 2 (7%) 3 (10%) 6 (21%) 2 (7%) 4 (14%) 6 (21%) LE (17) Department of Surgery, University of Pennsylvania Health System
Malperfusion Presentation (N=29) Mesenteric (N=18; 62%) # of patients Presentation Abdominal pain Ileus, abdominal distension Nausea, vomiting Elevated LFT, pancreatic enzymes, lactate Post-prandial angina Diarrhea Splenic infarct Renal (N=17; 59%) Presentation # of patients Cr elevation from baseline Oliguria, anuria Renal infarct 15 (88%) 7 (41%) 2 (11. 8%) 11 (61%) 6 (33%) 3 (16. 6%) 2 (11. 1%) 1 (5. 6%) LE (N=18; 62%) Presentation # of patients Absent femoral pulses 15 (83%) Ischemic LE 9 (50%) Neurologic LE deficits 5 (27. 8%) Claudication 1 (5. 5%)
Mesenteric Malperfusion § 18 patients § Adjunctive procedures: 1 patient (5. 6%) # of stents Celiac (1) SMA (1) 1 1 Stent make Stent size Herculink Acculink 5 x 15 7 -10 x 40 § Exploratory laparotomy: 2 patients § No bowel resections Department of Surgery, University of Pennsylvania Health System
Renal Malperfusion § 17 patients § Adjunctive procedures: 3 patients (17. 6%) Vessel # of stents Stent make Stent size Right 1 1 1 Herculink 7 x 15 6 x 15 5 x 15 § Renal function recovery – Pre-op Cr 3. 6 vs. D/C Cr 1. 5, p=0. 006 § Dialysis: 1 patients – CRI s/p previous nephrectomy Department of Surgery, University of Pennsylvania Health System
Lower Extremity Malperfusion § 18 patients Vessel § Adjunctive procedure details Infrarenal # of stents Stent make 5 patients 1 1 1 2 1 Zenith Wallstent Palmaz Common Iliac (R/L) 8 patients 13 vessels Stent size 22 x 55 32 x 39 20 x 40 22 x 35, 22 x 40 50 x 10 External Iliac (R/L) 4 patients 6 vessels Femoral (R/L) 2 patients 2 vessels # of stents Stent make Stent size 1/2 -/2 1/1 Wallstent/Express 10 x 40 /12 x 40 x 2 10 x 20 / 10 x 25 1/- Wallstent 14 x 40 1/1 1/1 1/-/1 1/1 Wallstent Express Wallstent/Sentinel Wallstent 14 x 40 / 14 x 40 12 x 40 / 12 x 40 10 x 25 10 x 40 x 2 8 x 42 12 x 40 / 7 x 78 8 x 40 / 8 x 40 -/1 1/- Sentinel Viabahn 7 x 78 8 x 5 § Fasciotomy – – 5 patients Adjunctive group only (p=0. 068) § No amputations Department of Surgery, University of Pennsylvania Health System
Rupture Presentation (N=24) Presentation # of Patients % Chest/back pain 23 95. 8 Hemothorax/Contained leak 18 75. 0 Mediastinal hematoma 11 45. 8 Hypertensive crisis 2 8. 3 Hypotension 2 8. 3 Department of Surgery, University of Pennsylvania Health System
Operative Strategy Malperfusion Rupture Time to Surgery ( days) Device characteristics # of Devices Mean prox endograft diameter (mm) Mean distal endograft diameter (mm) Total length (Combined length, cm) p 2 ± 2. 5 0. 67 ± 1. 2 0. 02 1. 9 ± 0. 70 33. 2 ± 5. 3 31. 5 ± 5. 7 28. 7 ± 137 2 ± 0. 83 33. 8 ± 3. 9 31. 1 ± 3. 9 33. 9 ± 128 0. 75 0. 69 0. 8 0. 16 21 (72. 4%) 2 (6. 9%) 21 (87. 5%) 1 (4. 2%) 0. 18 0. 67 0 1 (4. 2%) -- 0 283 ± 118 1 (4. 2%) 223 ± 89 -0. 056 Left SCA management SCA coverage L SCA coil embolization CCA-SCA bypass Celiac coverage Operative Time (min) Adjunctive Stenting: Malperfusion 14 (48%) vs. rupture 1 (4%), p=0. 004
Results § Follow-up 27. 7 ± 15. 6 months (3 -67) Stroke Transient paraparesis Paralysis Malperfusion Rupture p 0 6 2 1 0. 92 0. 21 0. 67 § Excellent 30 -day and 1 year survival achieved in both groups Survival 30 days All Dissection-related 1 Year All Dissection-related Malperfusion Rupture p 28/29 (96. 6%) 28/28 (100%) 23/24 (95. 8%) 0. 89 0. 94 22/24 (91. 7%) 22/23 (95. 7%) 16/17 (94. 1%) 0. 77 0. 83
All-Cause Mortality Department of Surgery, University of Pennsylvania Health System
Department of Surgery, University of Pennsylvania Health System
Clinical Trials § Medtronic-Valiant § Gore-CTAG § Cook-Zenith Dissection
Department of Surgery, University of Pennsylvania Health System
Department of Surgery, University of Pennsylvania Health System
Concerns § IMH § Retrograde extension Department of Surgery, University of Pennsylvania Health System
Conclusions § Type B Aortic Dissections – Uncomplicated » Manage medically-for now » Aortic remodeling – Complicated » TEVAR offers improved morbidity and mortality Department of Surgery, University of Pennsylvania Health System