Indian Scenario TB Situation HIV Situation Estimated 400

Indian Scenario TB Situation HIV Situation • Estimated 400 million • Estimated 2. 5 million infected with TB with HIV ( National Adult HIV Prevalence • 1. 8 million new TB 0. 36%) cases annually • Incidence of TB is higher • Prevalence of HIV higher in north in south TB/HIV Co-infection Estimated 1 million co-infected with TB and HIV Estimated ~5% of TB patients are HIV positive nationwide ( WHO Global TB Report-2005)

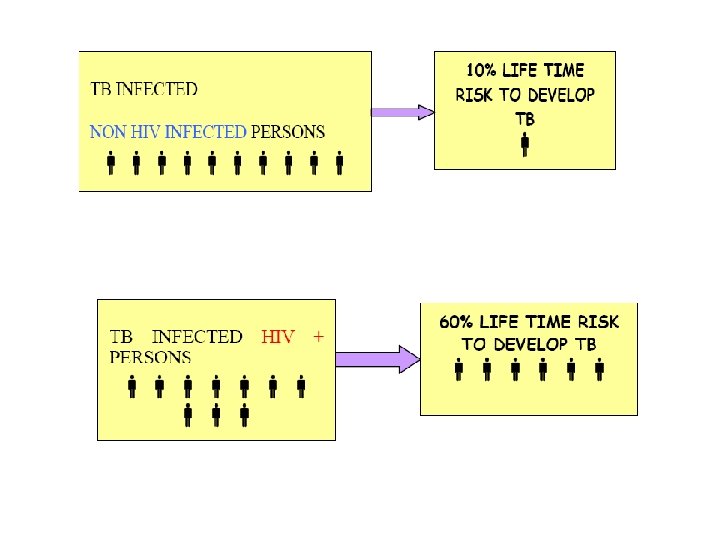
Influence of HIV on TB Lifetime Risk of TB

Common Opportunistic Infections in INDIA Opportunistic Infection Prevalence Pulmonary TB 49% Pneumocystis Carinii Pneumonia 6% Cryptococcal Meningitis 5% Cerebral Toxoplasmosis 3%

Impact of TB on HIV programme • Increased caseload of active TB among PLWHA • Increased morbidity and mortality from TB among PLWHA • Difficulties with diagnosing TB among PLWHA due to different clinical presentation. . . (Extra Pulmonary TB) • Increased burden on HIV services

Impact of HIV on TB programme • Increased caseload of active TB attributable to HIV • Higher default rates, lower cure rates • More adverse drug reactions • Increased burden on TB services

INTENSIFIED TB CASE FINDING AT ICTCS • All ICTC clients should be screened by the ICTC Counsellor for the presence of the symptoms of TB disease. – 10 point counseling tool on TB in place – At pre, post, and follow-up Counselling – All TB suspects, irrespective of their HIV status, should be referred to nearest facility providing RNTCP services. 9/25/2020

ICF at ICTC Counselors trained in TB symptom screening “ 10 -point TB Screening Tool” visible to counselor, with referral list for TB diagnosis

Treatment of TB in HIV-Infected Patients • Anti-TB treatment is the same for HIV-infected persons as it is for HIV-negative TB patients, and all patients should be treated with RNTCP regimens under the DOTS strategy. • All New TB cases known to be HIV positive should be treated with Category I regimen. • The re-treatment cases are to be treated with Category II regimen. • RNTCP regimens, if supervised properly are as effective in HIV positive as in HIV negative patients.

TB/HIV • CROSS REFERRAL NACP-RNTCP • Treatment should be first administered for TB under the DOTS strategy and if the patient’s clinical condition allows, ART should be started after completion of TB treatment. • All TB patients diagnosed to be HIV positive are to be provided CPT. 9/25/2020

TB/HIV • In patients with very low CD 4 counts requiring concomitant administration of ART and anti-TB treatment: - ART regimen should be modified by replacing Nevirapine with Efavirenz. - On completion of TB treatment, such patients can be switched back to Nevirapine. 9/25/2020
- Slides: 11