Incidence of the Acetabuar Fracture In ALThawra Modern

Incidence of the Acetabuar Fracture In AL-Thawra Modern general hospital During 2009 –Sana'a-Yemen


Ant. View of ACETABULAM

Post. View of ACETABULAM

. Callisen in 1788 start to said and to have reported the case of an acetabular fracture

During 2009 70 patients with acetabular fractures
 56 cases(80%)")
Gender distribution of 70 patients with acetabular fractures 14(20%) 56 cases(80%)

The main cause of fracture is DISLUCATION OF THE HIP

● this injury is due to massive force transmitted along the femoral shaft, e. g. road traffic accidents or a back injury in someone kneeling.

distribution of 70 patients with acetabular fracture according to mechanism of injury MECHANISM OF TRAUMA GENDER FEMALE T % RTA 40 57% GUN SHOT 5 7% FALLING 21 30% OTHER 4 6% TOTAL 70 100. 00%


Type of Dislocation depends on position :

I. Anterior dislocation of hip 7 -10% OF DIS NON FRACTURE OF ACETABULAM

II. Posterior dislocation Most common type of dislocation. Posterior rim is usually fractured Associated sciatic nerve injury in 10%

flexed, shortened, adducted and internally rotated

III. CENTRAL dislocation Direct impact to the aspect of the hip through the acetabulum. This is a fracture dislocation.


Distribution of the acetabualr fracture by age group and gender AGE GROUPS GENDER TOTAL M F N % 19 -20 7 3 10 7% 21 -30 36 7 43 30. 1% 31 -40 11 1 12 8. 4% 41 -50 4 1 3 2. 1% 51 -60 9 2 9 6. 3% TOTAL 56 14 70 100. 00%

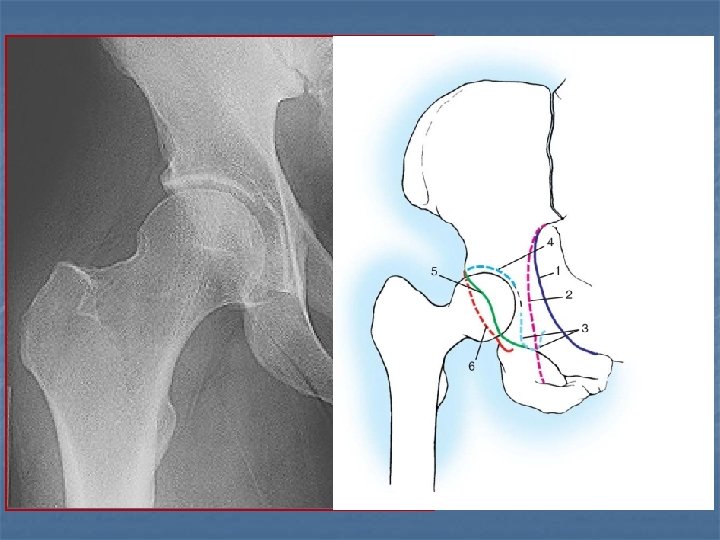
I. AP View pelvis

ACETABLUM FEMORAL HEAD FEMORAL NECK GREATER TROCHANTER FOVEA CAPITIS LESSER TROCHANTER CORTICAL BONE MEDULLARY BONE
")
II. JUDET view OBTURATOR (Internal oblique view)
")
III. JUDET view Iliac (exteternal oblique view)

WE CAN DIAGNOSED THE FRACTURE IN ONE OF 3 VIEW

CT is a very useful to assessment and planning of surgery.


70 patients with acetabular fracture accoding to associated injures TOTAL ASSOCIATED TRAUMA N % MULTIBLE TRAUMA 27 38% ISOLATED ACETABULAR 43 62% 70 100% FRACTURE TOTAL

Distrubiton of acetabular fracture according to departement of intial admission INTENSIVE CARE UNIT GENDER M F 5 2 TOTAL T % 7 10% SURGICAL DEP. 7 2 9 12. 8% ORTHOPEDIC DEP. 35 8 43 61. 4% NEUROSURGICAL DEP. 4 1 5 7% UROLOGY DEP. 5 1 6 8. 5% 56 14 70 100% DEPARTMENT TOTAL

associated injury

distribution of complication releated to the associated injury in 27 patients: ASSOCIATED INJURIE N % LIMBS 6 22. 2 VASCULAR 3 16. 2 NEUROLOGY 2 11. 6 UROLOGY 9 33. 3 ABOMINAL 3 4. 6 THORACIC 4 2. 3 TOTAL 27 38%

We used Letournel ANATOMICAL system classification

TYPE OF CLASSIFICATION NO % SIMPLE FRACTURE TYPE posterior wall 20 28% posterior column 3 4. 2% anterior wall 1 1. 4% anterior column 2 2. 8% transverse 7 10%

ASSOCIATED FRACTURE TYPE posterior column +posterior wall 1 1. 4% transverse +posterior wall 11 15. 7% T- shape 5 7% 8 11. 4% 12 17% anterior column or wall + posteriorhemitransverase both column

 II. SURGICAL")
Treatment I. Closed reduction ( to reduce pain ) II. SURGICAL

Closed reduction Four methods of closed reduction :

1.

Allis traction. 2

3.

4. Classical watson`s– jones method :

Skin Traction

Skeletal traction

II. SURGICAL treatment should be considered for: . all displaced fractures of the acetabulum. . that do not meet the criteria for nonoperative therapy.

Orthopaedic Surgeon Can Get You Back Into The Game
- Slides: 45