Inability to conceive within 1 year of regular

Inability to conceive within 1 year of regular unprotected sexual intercourse

§ Female factor § Male factor § Combined § Unexplained
 § metformin (corrects hyperinsulinaemia in")
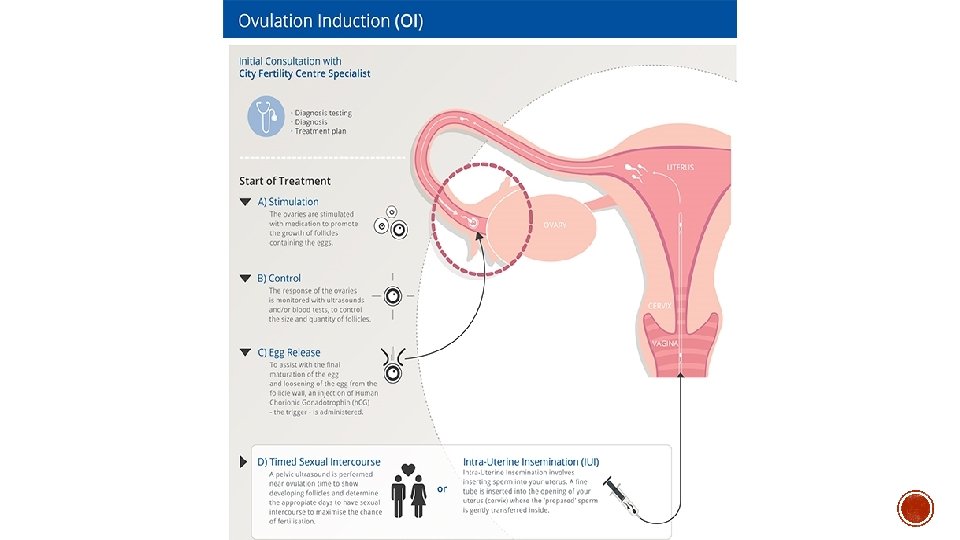
§ Ovulation induction § for anovulation § clomiphene (SERM) § metformin (corrects hyperinsulinaemia in PCOS) § letrozole (aromatase inhibitor) § Gn. RH therapy § FSH, h. MG § ovarian drilling § IVF
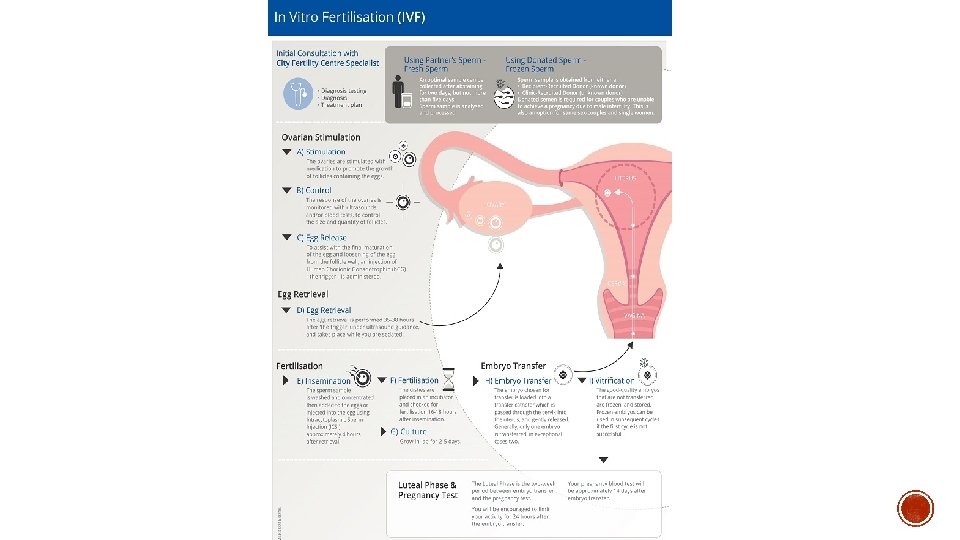

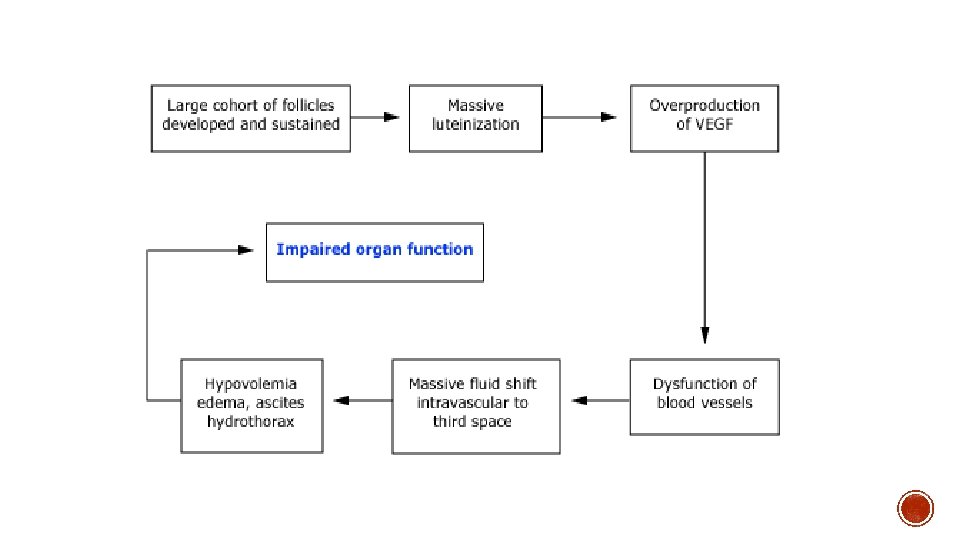
§ In normal ovulatory cycle – HPO feedback cycle limits follicle recruitment to small number of early antral follicles + subsequent single dominant follicle responding to LH surge § OHSS occurs when disruption of normal feedback mechanisms happens secondary to administration of exogenous gonadotrophins

§ Previous OHSS PCOS § Lower age <30 § GNRH agonists § Low body weight § Secondary risk factors: § High No. follicles § High serum oestradiol § No. oocytes retrieved § Administration of h. CG

§ Mild, moderate, severe

Clinical Bilateral ovarian enlargement Multiple follicular and CL cysts Abdo distension Mild nausea Occasional vomiting, diarrhoea Biochemical No abnormalities

Clinical As above + USS evidence of ascites Ovaries enlarged up to 12 cm Abdo distension + GI Sx Weight increase of >3 kg Biochemical PCV >41% (0. 4) WCC >15 Hypoproteinaemia
 Severe abdo pain Intractable n&v")
Clinical Biochemical As above + Clinical ascites (tense/rigid abdo) Severe abdo pain Intractable n&v Rapid wt gain Pleural effusion Severe dyspnoea Oliguria/anuria Low BP/central venous pressure Syncope Venous thrombosis Haemoconcentration PCV >0. 5 WCC >25 GFR <50 Hyponatraemia Hypokalaemia Elevated liver enzymes

Clinical As above + Anuria/acute renal failure Arrhythmia Pericardial effusion Massive hydrothorax Thromboembolism Arterial thrombosis ARDS/Sepsis Biochemical Worsening of above note risk of ovarian torsion as increased ovarian volume

§ History of ovarian stimulation + ovulation or administration of h. CG § Clinical Presentation § Bedside: ECG if suspect PE/Pericardial effusion § Bloods (as above) § Imaging: TV USS, CXR (If resp. Sx) § Special tests: VQ/CTPA, Echo DDx: Ectopic, haemorrhagic cyst, ruptured ovarian cyst, ovarian torsion

Mild/moderate: § generally as outpatient § if unable to control Sx – admit for analgesia/antiemetics § Analgesia – paracetamol. Avoid NSAIDs – compromise renal function § Drink to thirst § monitor Bloods § monitor input and output § Reassurance § provide contact details
, ICU (ARDS, renal failure), Med (VTE)")
§ Hospital admission § MDT – Resp (ARDS), ICU (ARDS, renal failure), Med (VTE) § O 2 § Daily weight/abdominal girth § Invasive monitoring § Analgesia, antiemetics § Strict fluid balance – § Drink to thirst § Avoid diuretics as deplete intravascular vol. § IV normal saline if not tolerating PO, average 2 -3 L per day § colloids if persistent haemoconcentration + oliguria § IDC § Daily bloods: FBC, UECs, LFTs, coags, bhcg, estradiol § Thromboprophylaxis § Ascites/Effusion Mx § Paracentesis if abdo distension or persistent oliguria (drainage may promote renal perfusion and Improve urine output). § Surgical Mx § Ovarian torsion § Do not proceed with embryo transfer, freeze for later transfer § Consider TOP if life threatening

§ infection/peritonitis § bleeding § trauma to bowel/vv
- Slides: 18