In the name of God Molecular Basis Of

In the name of God Molecular Basis Of Aortic Aneurysms M. Mohamadian

Definitions Aneurysm A permanent dilatation of 50% or more compared wit the expected normal diameter of the vessel. Ectasia An arterial dilatation less then 50% of the or Diameter. Arteriomegaly A diffuse enlargement in several arterial segments greater than 50% in diameter
 - Bicuspid aortic valve(BAV) -")
Aortic Aneurysms 1. Thoracic Aortic Aneurysms - Marfan syndrome(MFS) - Bicuspid aortic valve(BAV) - Familial thoracic aortic aneurysm syndrome 2. Abdominal Aortic Aneurysms

MFS Review - MFS is a systemic disorder of connective tissue with protean manifestations, with the skeletal, ocular, and cardiovascular systems most often affected. - The hallmark of MFS is abnormality of the medial layer of the aortic wall and the most threatening consequence of MFS is dilatation of the aortic root and the ascending aorta, which, if untreated, can result in fatal aortic dissection or rupture. - Autosomal-dominant with complete penetrance. - FBN 1 mutations were linked to the majority of the cases of MFS - In addition, a distinct gene on chromosome 3 p 24 (TGFBR 2) was linked to another family with MFS.

Notice ü It is possible that the genes responsible for MFS may also account for the development of the associated thoracic aortopathy, because of a shared embryological origin of the aortic valve and the ascending aorta from the cardiac neural crest cells.

FBN 1

TGFBR 1, TGFBR 2, SMAD 3 - TGFβR 1, 2: Four missense mutations that affect the kinase domains, causing MFS and familial thoracic aortic aneurysm and aortic dissections (TAAD), have been described. - SMAD 3: One frameshift mutation and three missense mutations were identified in individuals with FTAAD, located in exons 2, 5, and 6 Dysregulation of ECM, proliferation and differentiation in aortic wall cells.
 - BAVD is the most common congenital cardiac malformation,")
Bicuspid aortic valve disease (BAVD) - BAVD is the most common congenital cardiac malformation, affecting 1– 2% of the population. - BAVD is highly associated with other congenital aorta abnormalities, such as coarctation , dilatation of the aortic root or ascending aorta and may progress to frank thoracic aortic aneurysms and aortic dissection. - The histopathology in such cases is similar to that of patients with MFS who also have abnormal FBN 1 content in their aortic wall. - Fibrillin-1 deficiency is also observed in the pulmonary arteries of BAV patients and main pulmonary artery dilatation has been noted to occur in association with BAV in the absence of pulmonary valve abnormality.
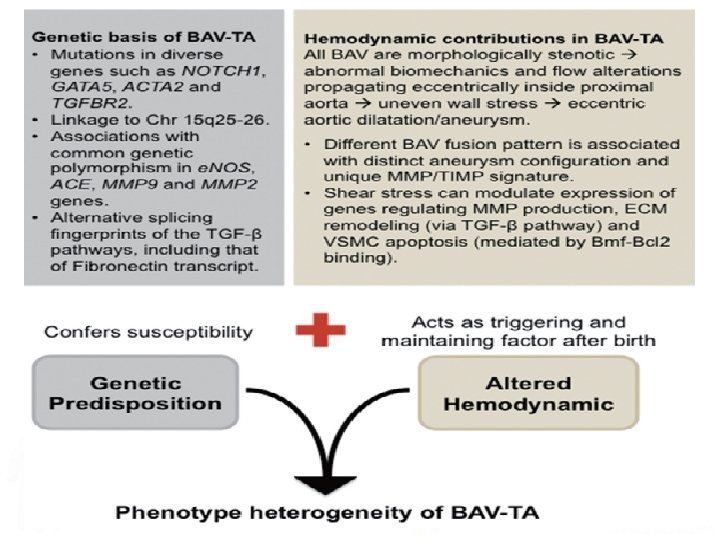

Hemodynamic contributions in BAV-TA - Increased expression of MMP 2 and a higher MMP 2 to TIMP 1 activity in tissue samples from aortic aneurysms in BAV patients. matrix degradation, weakening of aortic wall structural integrity, loss of aortic elasticity, progressive aortic dilatation, and aneurysm and/or dissection. - Reduction of endothelial nitric oxide synthase (e. NOS) protein expression, with site-dependent variability, which is probably triggered by variations in shear stress along the aortic wall. cytosolic accumulation of HTRA 2/Omi, a proapoptotic mitochondrial serine protease, which presumably mediates VSMC apoptosis in BAV aortas. - ECM remodelling occurs early in BAV(during development and valvulogenesis): collagen, laminin , fibrillin and fibulin reduction and increases in fibronectin and tenascin expression. increased Bcl-2 -modifying factor-Bcl-2 binding (Bmf-Bcl 2), a known matrix-dependent proapoptotic, enhanced VSMC apoptotic indices.

SO, … BAVD is the result of intrinsic defects in the ECM rather than a secondary consequence of valvular dysfunction. Evidences - Dilatation of the ascending thoracic aorta can be found in young adults with a bicuspid aortic valve but without significant valvular stenosis or regurgitation. - BAVD patients who have undergone aortic valve replacement can develop ascending thoracic aortic aneurysms at a later date.

Genetic and molecular basis of BAV-TA - BAV is a heritable trait: approximately 9% prevalence amongst first degree relatives, and up to 24% in families with more than one affected family member. - Genetic heterogeneity with variable patterns of inheritance. Major related genes: -Transcriptional regulator NOTCH 1 gene at chromosome 9 q 34. 3 -Homozygous deletion of the e. NOS (Nos 3) gene -Cardiac homeobox Nkx 2 -5 haploinsufficiency -Deletion of the cardiac transcription factor GATA 5 (essential factor in cardiogenesis and aortic valve development, endocardial cell differentiation).

NOTCH 1 - Activation of inflammatory pathways plays a critical role in the development of aneurysm. - Notch 1 signaling is a significant regulator of the inflammatory response. - Overexpression of NOTCH 1 increasing inflammatory response in the aorta. BAV

Genetic and molecular basis of BAV-TA - BAV has been observed to occur more frequently in patients with thoracic aortic aneurysm who have mutations in the FBN 1 and ACTA 2 genes. - A single nucleotide substitution in the TGFBR 2 gene, c 1159 G>A, which results in an amino acid change (i. e. missense mutation) and destabilizes the mutant TGFBR 2 protein structure of the aortic media, was segregated in a family with BAV and proximal aortic aneurysm. - Genome-wide marker-based linkage analyses have provided evidence on the genetic basis of BAV-TA with some families with BAV and ascending aortic aneurysms showing linkage to chromosome 15 q 2526. although the causal gene(s) are yet to be identified.

ACTA 2 - ACTA 2 mutated in 14 -20% of people with thorasic aortic aneurysm The ACTA 2 gene smooth muscle alpha (α)-2 actin, which is ound in vascular smooth muscle cells. (walls of the aorta) omeres formation which are necessary for muscles to contract. allows the arteries to maintain their shape instead of stretching out as blood is pumped through them. ACTA 2 dominant negative mutations Abnormal stretching of the aorta results in the aortic dilatation, aneurysms, and dissections.

further clues - Recently, a comparative study on global gene expression levels was performed in aortic tissues from patients with bicuspid or tricuspid aortic valve, with and without thoracic aortic aneurysm, Only 7 genes showed differential expression in 2 groups: LEFTY 2 (a TGF-β family member), The 4 upregulated genes FRAS 1 (a member of ECM family of protein), SHC 4(Src Homology 2 Domain Containing) DAPK 3 (a proapoptotic gene). The 3 downregulated genes VEGFC (a member of VEGF family) NFASC (a member of the L 1 family of CAMs) LSP 1 (lymphocyte-specific protein-1).

further clues - BAV patients with aortic dilatation showed an almost exclusive expression of the TGF-β binding proteins LTBP 3/4, ADAMTSL 1 and an alternatively spliced isoform of Fibronectin-1 (FN 1). Likely, they have impaired TGF-β mediated splicing mechanisms of fibronectin transcript, thereby leading to altered fibronectin expression in the aortic aneurysm tissue and consequently contributing to the increased susceptibility to aortopathy development in BAV patients.

Familial thoracic aortic aneurysm syndrome - Familial TAAD is expected to cause about 20% of all cases of thoracic aortic aneurysms and dissections. - This disorder can occur in conjunction with other genetic syndromes including Marfan syndrome, Loeys-Dietz syndrome, Ehlers-Danolos, and other related syndromes. - Not have identifiable congenital abnormalities. - Absence of overt connective tissue disorders. - Most pedigrees suggested autosomal-dominant of inheritance. - Variability in the expression and penetrance - Genetic heterogeneity

Genetics of familial thoracic aortic aneurysm syndrome

MYH 11 - Account for 2% of non-syndromic TAAD. - Heterozygous MYH 11 mutations result in thoracic aortic aneurysms and are thought to act via a dominant negative mechanism with wild-type MYH 11.

MYLK - MYLK encodes three gene products expressed from separate promoters, with two isoforms containing the catalytic and Ca. M-binding domains and a third, small, non-catalytic protein called telokin (that affects calcium sensitivity of contraction). - A c. 4438 C>T (p. Arg 1480 Ter) mutation located in the MLCK kinase domain leads to either nonsense-mediated decay or a truncated protein. - Two other missense alterations, c. 5260 G>A and c. 5275 T>C, disrupt in calmodulin-binding sequence and lead to decreased MLCK function
 - AAA is usually defined as infrarenal aortic diameter >30 mm.")
Abdominal Aortic Aneurysms(AAA) - AAA is usually defined as infrarenal aortic diameter >30 mm. - AAAs are typically associated with aging and atherosclerosis. - Gender plays a role; men are 10 times more likely than women to have an AAA of 4 cm or greater, BUT women with an AAA have a significantly greater risk of rupture than men. - Approximately 20 % of the patients with an abdominal aortic aneurysm (AAA) have a positive family history for aneurysms. - Those having a first-degree relative with an AAA have an increased risk of 13– 32% compared with the 2– 5% risk in the general population. - Those with familial aneurysms tend to be younger and have higher rates of rupture than those with sporadic aneurysms.

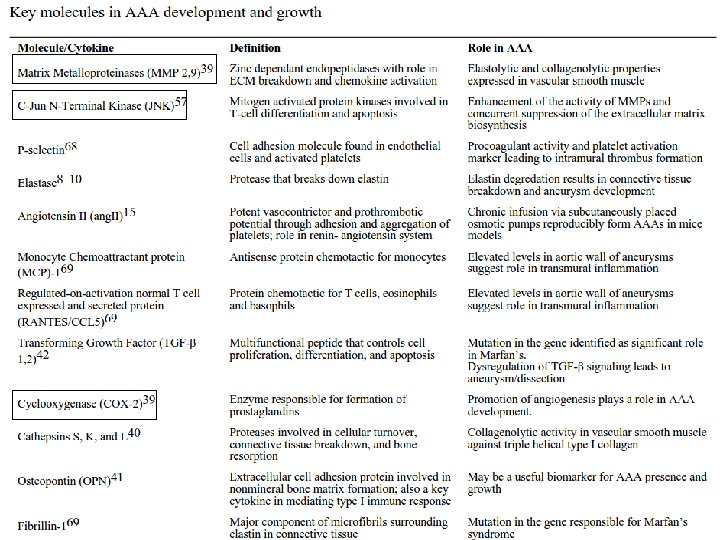
Pathophysiology of AAA Biochemical wall stress. - Natural reduction in the number of elastin layers in the aortic wall in the infrarenal aorta. - Decrease in the collagen content from the proximal to the distal aorta. - A calcified plaque, a common feature of AAAs, causes increased local wall stress due to the focal stiffness Destructive remodeling of the elastic media of the aortic wall Infiltration of inflammatory cells, including B lymphocytes, T lymphocytes, and macrophages. Increased immunoreactivity for elastolytic matrix metalloproteases (MMP), particularly MMP-2, MMP-9, and MMP-12, secreted by the infiltrating macrophages, and cytokines. Elastolysis Aortic aneurysms

Genetic basis of AAA - Genes associated with the familial thoracic aortic aneurysm play a role in the degenerative changes of the extracellular matrix of the abdominal aortic wall underlying the formation of AAA. - In addition, an association between abdominal aneurysm and the c. 665 C>T variant in MTHFR have been investigated. - There is higher incidence of the allele subtype HLA-DR B 1*0401 and HLADQA 1*0102 in the AAA patient. In contrast, the HLA-DR B 1*01 allele tended to behave as a protective factor for AAA.

MTHFR - Serum folate deficiency and hyperhomocysteinemia were associated with an increased risk of AAA - ER stress induced by homocysteine increases gene expression of MMP-3 (ER stress-induced apoptosis in aortic wall cells)

Apo-E, NOS Atherosclerotic lesions, such as those seen in the apo-E mutation, serve as the initial insult leading to a chronic inflammatory state. But not sufficient to induce the formation of aneurysms, a significant endothelial dysfunction (such as lack of the critical endothelial regulator nitric oxide) may be the second factor that accelerates the process of AAA formation. Apo-E Knockout & NOS knockout Mice were more hypertensive than control wild -type mice, and a significant proportion of these mice developed an AAA. The development of the AAA was not simply owing to hypertension, because lowering the blood pressure to levels seen in the control mice had no effect in reducing aneurysm development!

Genetic Associations by meta-analyses. LRP 1, LDLR, SORT 1 affect cholesterol metabolism and atherosclerosis. LRP 1 has other important regulatory roles, including regulation of extracellular matrix breakdown by the endocytosis of proteinases. LPA produces lipoprotein A, which increases cardiovascular risk. IL 6 R polymorphisms alter cardiovascular risk, possibly through inflammation. MMP 3 affects atherosclerosis and tissue remodelling. AGTR 1 affects blood pressure, which is consistent with the association between hypertension and AAA. DAB 2 IP is a tumour suppressor gene involved in cell signalling, survival, migration, maturation, and apoptosis.
 or other proteases such as cathepsins")
Pharmacotherapy - Inhibitors of MMPs (doxycycline and BB-94) or other proteases such as cathepsins and plasminogen-activator inhibitor (PAI-1) offers a tremendous therapeutic strategy to prevent AAA enlargement. - Inflammation plays an integral role in the development of AAA and expression of the inflammatory molecule, cyclooxygenase (COX)-2, is increased in aneurysmal tissues: NSAIDs (celecoxib) decreased the incidence and severity of AAA formation - C-Jun N-Terminal Kinase (JNK) is highly active in human AAA walls and specific inhibition of JNK can significantly suppress the secretion of MMP-9 and prevent collagen degradation. JNK inhibition may play a significant role in impeding the progression of AAA.

References D. T. Bradley a, S. A. Badger et al. Abdominal Aortic Aneurysm Genetic Associations: Mostly False? A Systematic Review and Meta-analysis. Eur J Vasc Endovasc Surg (2016) 51, 64 -75 Koen M. van de Luijtgaarden et al. First genetic analysis of aneurysm genes in familial and sporadic abdominal aortic aneurysm. Hum Genet (2015) 134: 881– 893. Ratnasari Padang, Paul G. Bannon et al. The genetic and molecular basis of bicuspid aortic valve associated thoracic aortopathy: a link to phenotype heterogeneity. Ann Cardiothorac Surg 2013; 2(1): 83 -91 Suman Annambhotla, Sebastian Bourgeois et al. Recent Advances in Molecular Mechanisms of Abdominal Aortic Aneurysm Formation. World J Surg. 2008 June ; 32(6): 976– 986

- Slides: 31