In the name of God Dr M Habibi

In the name of God Dr. M. Habibi Neonatologist Assistant professor of pediatrics

Vasospasms and thromboembolism in neonate: *Cause : usually occur with indwelling arterial or sometime venous catheters. More commonly umbilical & less common with peripheral line. Neonates are at a high risk because of their : A: immature hemostatic system B: smaller vessel size Vasospasm commonly occur in arterial catheterization but thromboembolism common with venous catheterization. * most medications if given too rapidly can cause vasospasms
 Maternal: 1) Autoimmune disorder 2) PROM 3) Diabetes 4) Preeclampsia")
*risk factors : A) Maternal: 1) Autoimmune disorder 2) PROM 3) Diabetes 4) Preeclampsia 5) Oligohydramnios 6) Prothrombotic disorder 7) Chorioamnionitis 8) familial history of thrombosis 9) anti-phospholipid or anti-cardiolipin Ab
Delivery : 1) Instrumentation 2) Fetal heart rate abnormality 3) C/S Emergency 4) Traumatic")
B)Delivery : 1) Instrumentation 2) Fetal heart rate abnormality 3) C/S Emergency 4) Traumatic delivery
 Neonate : 1) C. A. C (central arterial catheter)is the most common risk")
C) Neonate : 1) C. A. C (central arterial catheter)is the most common risk factor 2) Central venous catheters 3) Congenital heart disease 4) Asphyxia 5) Sepsis 6) SGA & IUGR 7) RDS 8) NEC
 Polycytemia 10) PPHN 11) Dehydration 12) Congenital Nephrotic syndrome 13)DIC 14) Impaired liver")
9) Polycytemia 10) PPHN 11) Dehydration 12) Congenital Nephrotic syndrome 13)DIC 14) Impaired liver function 15) low cardiac output & hypotention 16) Prothrombotic disorder ( protein C & S deficiency, factor V leiden mutation, anti-thrombin deficiency , elevation of lipoprotein A level & other things like impaired liver function. )
 Vasospasm: Due to muscular contraction it is commonly arterial 1. catheter 2. injection")
ɪ) Vasospasm: Due to muscular contraction it is commonly arterial 1. catheter 2. injection of medication 3. Sampling a. Less severe vasospasm: Involves a small area of one or both legs (usually some of the toes and parts of the foot or hand) * in this type : skin has a mottled appearance & pulses are present but diminished.
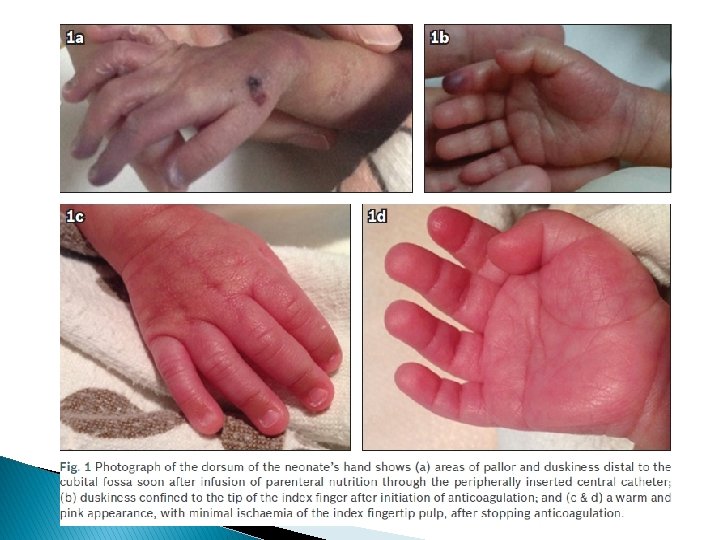


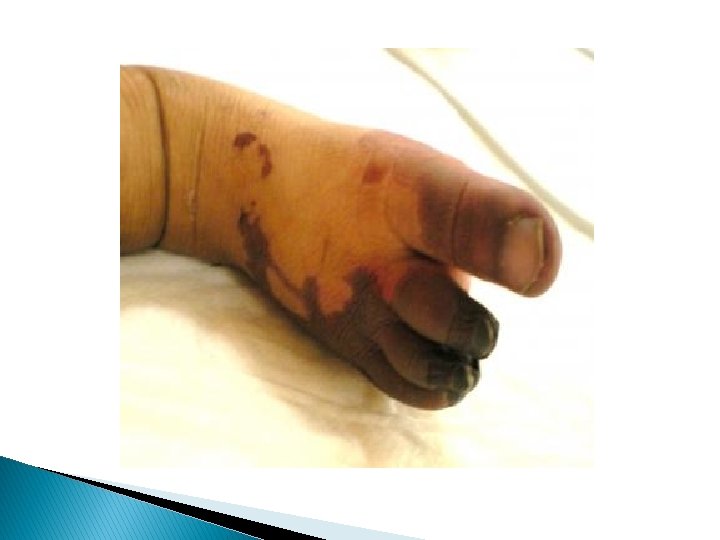
b. severe vasospasm: Involves large area of one or both extremity and sometime progresses to buttocks and abdomen. * in this type: skin maybe completely white -Perfusion decreased -Pulses of affected extremity are week but detectable



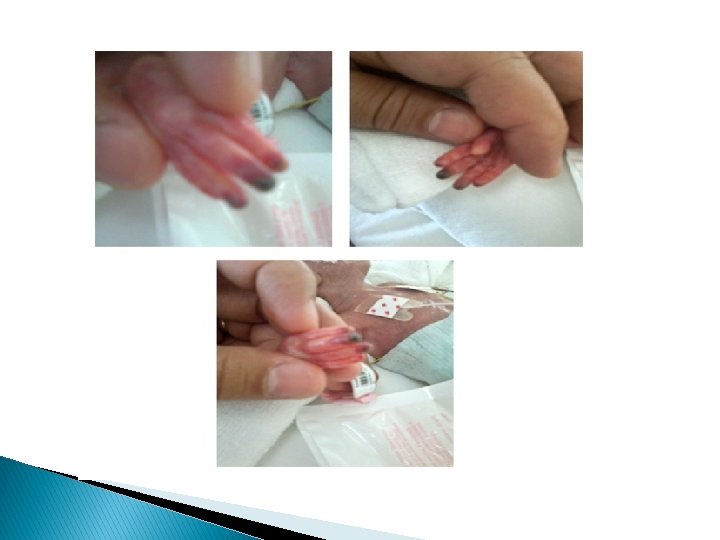

Arterial thrombosis: Is a medical emergency in which pulse usually are completely absent & persistent bacteremia & thrombocytopenia may be associated with thrombosis Venous thrombosis : More common and it’s first sign is catheter dysfunction Extremities are swollen – cyanotic –hyperemic and discolored with distended superficial veins but renal vein thrombosis is most common type of spontaneous venous thrombosis




Laboratory studies: Not usually needed for vasospasm but in suspected thromboembolism following studies should be done: 1. Coagulation profile : PT, PTT , Plasma fibrinogen concentration. 2. Hb & HCT 3. Plate count & function (BT) 4. CMV workup 5. workup for thrombotic disorder (Protein C & S & anti-thrombin ɪɪɪ - factor V leiden & antiphospholipid & cardiolipin Ab
 2. ultrasound (Doppler flow)")
Imaging: 1. Plain radiograph of the abdomen (for catheter placement) 2. ultrasound (Doppler flow) for thrombosis(also evaluate Brain & kidney sonography) arterial 3. Contrast angiography ( gold standard) Venous arterial 4. magnetic resonance (MR)angiograph Venous Is done in some centers especially for suspected stroke.

Some general recommendations for Prophylaxy: 1. Small catheters should be used 2. heparin is used for patency of peripheral and central Arterial catheter 25 -200 u/kg/d(0. 5 unit/ml)concentration 3. heparin is not used in peripheral venous line 4. in central venous and PICC sometimes Heparin is recommended 5. Umblical line Should be removed as soon as possible ; arterial line should not be in place longer than 5 days and venous line not longer than 14 days. 6. PICC line has lower incidence of thrombosis. 7. Use peripheral line over umblical line.
Vasospasm: Guide lines vary extensively 1. If possible remove the catheter 2. Warming")
Management: A)Vasospasm: Guide lines vary extensively 1. If possible remove the catheter 2. Warming the contra lateral extremity wrapping of unaffected extremity should cause reflex vasodilation of the affected vessels. continue it for 15 -30 min. 3. Gentle massage at the Site of occlusion) 4. Topical nitroglycerin therapy (2%ointment)4 mm/kg every 8 hours for (2 -27 day) improvement usually seen within 15 -45 min.

5. If it is not possible to remove the catheter (it is the only line) consider papaverin 60 mg/500 cc/N/s with 0/1 unit/ml heparin continuous for 48 hr if vasospasm persist removed catheter. 6. lidocaine(controversial) 2 mg/kg/hr 7. Morphine 8. surgery (sympathectomy)
 Thromboemboli : ** Supportive care ** 1. prompt removal of the catheter 2.")
B) Thromboemboli : ** Supportive care ** 1. prompt removal of the catheter 2. treatment of volume depletion- Electrolyte abnormality – Sepsis – Thrombocytopenia – anemia 3. Emergency consultant with surgeon & hematologist 4. Evaluate for IVH 5. Rule out contraindication of anticoagulant & thrombolytic therapy (surgery & asphyxia in the last 10 days) – severe coagulation deficiency – plate under 50000 – fibrinogen under 100 mg/dl – INR>2
- Slides: 26