In the name of God Dr F Shariati







 less than 6")





, or delayed (days). v immunological(Type I")




 and")
 Ø American College of Rheumatology proposed the following five criteria. The presence")





















- Slides: 42
In the name of God Dr. F. Shariati
In medicine v. Most drug-induced cutaneous reactions are mild and disappear when the offending drug is withdrawn. v Drugs can also cause hair and nail changes, affect the mucous membranes, or cause itching without outward skin changes
Drug Eruptions v Drug eruptions are diagnosed mainly from the: ü medical history ü clinical examination v However, they can mimic a wide range of other conditions
Drug Eruptions v. A drug-induced reaction should be considered in any patient who is taking medications and who suddenly develops a symmetric cutaneous eruption
Drug Eruptions v to ccurs in approximately 2 -5% of inpatients and in greater than 1%-3% of outpatients v. The serious drug eruptions occur in around 1 in 1000 patients
Drug Eruptions v Drug Reaction mortality : 1. 8% percent v Mortality rates for Stevens-Johnson syndrome (SJS) has a less than 5%, vwhereas the rate for TEN approaches 20 - 30%; most patients die from sepsis
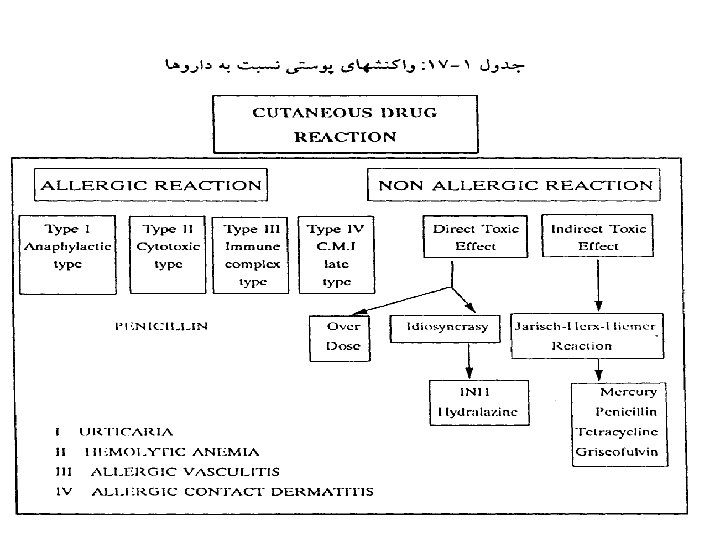
Classification v By appearance The most common type of eruption is a morbilliform resembling measles or erythematous rash, (but the appearance may also be……. . ) v By mechanism The underlying mechanism can be immunological in drug or non-immunological v By drug The culprit can be both a prescription drug or an overcounter medication. (antibiotic, analgesic, herbal supplement)
Drug Eruptions Physiopathology of Cutaneous Drug Reaction v Allergic Reaction (Immunologic) less than 6 -10% v Non allergic Reaction (Non Immunologic) More than. 90%
Non - allergic Drug Reaction v v v v Over Dose Side Effects Cumulative Toxicity Delayed Toxicity Facultative Effects Drug Interaction Metabolic Changes Teratogenicity of Fetus Activation of Effector Pathways Exacerbation of Diseases Chromosomal Damage by Drug Intolerance and Idiosyncrasy Jarisch — herxheimer reaction Infectious mono - , ampicillin reaction
Drug Eruptions: clinical appearance Ø Drug-induced exanthems Ø Urticaria Ø Angioedema/anaphylaxis Ø DRESS Sydrome Ø Hypersensitivity vasculitis Ø Exfoliative dermatitis/Erythroderma Ø SJS/TEN Ø Fixed drug eruption Ø Photosensitivity
Drug-induced Exanthems Ø Account for close to 75% of all drug eruptions. Ø Morbilliform, maculopapular eruptions. Ø Most commonly implicated medications are the most commonly prescribed medications (antibiotics, sulfa). Ø Usually begin in generalize areas. Ø Often associated with pruritis, low-grade fever, eosinophilia. Ø Onset within 2 weeks of starting a new drug, or within days of reexposure. Ø Delayed (type IV) hypersensitivity is most likely etiology. Ø More common in patients with altered immunity, such as those with HIV or mononucleosis (“ampicillin rash”). Ø Treatment is dicontinuation of the drug. Antihistamines, topical steroids, and topical antipruritics may also help.
Drug-induced Exanthems
Urticaria: v Time to onset: immediate, accelerated (hours), or delayed (days). v immunological(Type I hypersensitivity reactions) : antibiotics (especially PCN, cephalosporins, and sulfonamides), local anesthetics, radiocontrast media, blood products, and gamma globulin. v Non-immune urticaria: Mast cell degranulation by non. Ig. E mechanisms: opiate analgesics, anesthetic, muscle relaxants, and Vancomycin (Red Man Syndrome).
Angioedema/Anaphylaxis Ø Caused by degranulation of mast cells in the deeper dermis and subcutaneous tissues. Ø May occur along with urticaria (50% of cases) Ø Can be life-threatening if it causes laryngeal edema or tongue swelling. Ø Can be non-mast cell mediated, as in the case of ACEinhibitors.
Angioedema/An aphylaxis
DRESs Syndrome Drug Rash with Eosinophilia and Systemic Symptoms v Formerly called Hypersensitivity Syndrome (HSS) ü Typically presents with rash and fever (87%), classically erythematous follicular papules and pustules, but may also include bullae or purpura. ü Other severe systemic manifestations such as arthralgias, lymphadenopathy (75%), hepatitis (51%), or hematologic abnormalities (30%). interstitial nephritis (11%), ü Hematologic abnormalities include eosinophilia, thrombocytopenia, neutropenia, and atypical lymphocytosis. ü Other symptoms: pruritis, nephritis, oliguria, hepato-renal syndrome, and asthenia. ü DDx includes SJS/TEN, hypereosinophilic syndrome, and Still’s disease. ü Skin biopsy is non-specific.
DRESS Syndrome Ø Common causes: aromatic anticonvulsants (oxcarbazepine, carbamazepine, phenytoin, phenobarbital, etc. ) and sulfonamides. Ø Other drugs implicated: Ø Ø Ø Ø Ø lamotrigine allopurinol NSAIDs Captopril fluoxetine dapsone metronidazole minocycline antiretrovirals.
Hypersensitivity vasculitis(DHS) Ø American College of Rheumatology proposed the following five criteria. The presence of three or more had a sensitivity of 71% and a specificity of 84% for the diagnosis Ø Age > 16 Ø Use of possible offending drug in temporal relation to symptoms Ø Palpable purpura Ø Maculopapular rash Ø Biopsy of a skin lesion showing neutrophils around an arteriole or venule. Ø Most likely due to drugs that can act as haptens to stimulate the immune response: PCN, cephalosporins, sulfonamides, phenytoin, and allopurinol. Ø Additional findings: fever, urticaria, arthralgias, low complement (CH 50) levels, and elevated ESR.
Hypersensitivity vasculitis
Exfoliative dermatitis/ Erythroderma Ø Erythroderma is defined as a cutaneous reactional state with chronic erythema and scale involving greater than 50% of the body surface area. Ø Usually begins as an eczematous or morbilliform eruption and progresses. Ø Drugs including, gold, arsenic, mercury, PCN, and barbituates, are implicated in about 10% of cases.
Erythroderma: Marked inflammation and scaling which can result from a variety of medical conditions.
DICR SJS/TEN EMMi EMMa TEN SJS Ø Stevens-Johnson Syndrome and toxic epidermal necrolysis are likely two manifestations on the same spectrum. The disease is best termed SJS when epidermal detachment involves less than 10% of the body surface area, whereas TEN involves greater than 30%. Ø SJS is distinct from erythema multiforme major, which is usually caused by infections and runs a benign course. SJS is usually drug induced and can be fatal. Ø SJS and TEN usually occur 1 -3 weeks after exposure, but can occur more rapidly with re-exposure, which suggests an immunologic mechanism. Ø Mucosal involvement is seen in 90% of cases, including painful crusts and erosions on the oral mucosa, conjuntivae, and genital mucosa.
Toxic epidermal necrolysis
Fixed Drug Eruptions Ø Drug eruption that occurs at the same location every time a particular medication is used. Ø Begins as an erythematous, edematous plaque with a grayish center or frank bullae, then progresses to dark, post-inflammatory pigmentation. Ø Sites include the mouth, genetalia, face, and acral areas. Ø Causes include phenolphthalein, tetracyclines, barbituates, sulfonamides, NSAIDs, and salicylates.
fixed_drug_eruption_
Fixed drug eruption
PHTOSENSITIVE DRUG ERUPTION Photosensitive drug eruption: ü thiazides ü phenothiazines ü sulfa drugs ü tetracyclines ü Others
Characteristic Drug Changes ü Pigmentation of teeth due to tetracyclines
LICHENOID DRUG REACTION ü Type. II/III reaction ü lasix, captopril, chloroquin, gold, beta blockers, aldomet, penicillamine, thiazides, sulfa, many others ü *features diff. From LP: parakeratosis, hypogranul osis, EOS spongiosis, plasmacells, many EOS
LUPUS-LIKE SYNDROM Skin lesions: ü malar or butterfly rash ü Offending drugs: procaineamid, hydralazin, INH, methyldopa, chlorpromazin, penicillamine, ü PUVA, others
Silver : lunula discoloration D-penicillamine: Yellow nail Cytotoxics: Beau’s lines Minocycline: blue nails
Investigations • If history and physical examination are not sufficient for diagnosis, ØBiopsy e. g. by showing eosinophils in morbilliform eruptions or numerous neutrophils without vasculitis ØCBC count with differential may show leukopenia, thrombocytopenia, and eosinophilia in patients with serious drug eruptions
Confluent necrosis of the epidermis in toxic epidermal necrolysis
Perivascular mixed inflammatory infiltrate with eosinophils characteristic of drug induced urticaria
Treatment • Once the offending drug has been identified, it should be promptly stopped. • since traces of the drug may persist for long periods, and some reactions, continue for many days without reexposure to the drug • Patients with morbilliform eruptions can continue medication even in presence of rash as the eruption often resolves, especially if the individual is being treated for a serious disease
stage • Treatment of a drug eruption depends on the specific type of reaction ü Therapy for exanthematous drug eruptions is supportive in nature. ü First-generation antihistamines are used ü mild topical steroids (e. g. hydrocortisone) ü moisturizing lotions, especially during the late desquamative phase
• Topical steroids may provide some relief • If signs and symptoms are severe, a 2 -week course of systemic corticosteroids (prednisone, starting at 40 - 60 mg) will usually stop the symptoms and prevent further progression of the eruption within 48 hours of the onset of therapy
Good Luck