In the name of god Case presentation Dr


















 �Include just two groups: high risk group: with life-threatening anomalies")





































- Slides: 57
In the name of god Case presentation Dr. Mohammad Nemati
Tracheoesophageal Fistula �Case: A 12 -hour-old neonate born after 37 weeks of gestation and weighing 2200 grams had frothing about the nose and mouth. The infant regurgitated the first feeding almost immediately. coughing and cyanosis were associated with the regurgitation.
Medical disease and differential diagnosis
What is the working diagnosis? �The presence of frothing about the nose and mouth �History of polyhydramnios �Whether or not a catheter passes easily into the stomach
What information is needed to confirm the diagnosis? �Radiopaque catheter �Barium swallow or installation �Chest x-ray film �Flat plate of the abdomen
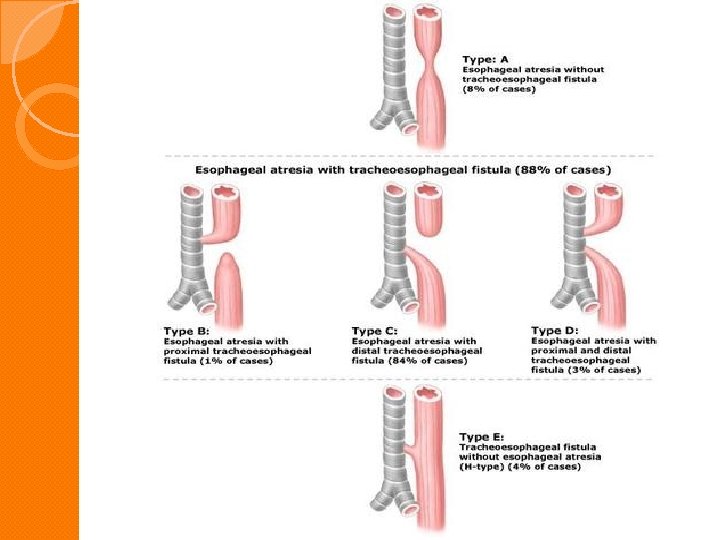
Classify TE fistula or atresia:
What other congenital anomalies are associate with TE fistula or atresia? �Associated anomalies occur in 30 -50% of cases. �Most common: cardiovascular anomalies genitourinary anomalies imperforated anus other intestinal athresia neurologic anomalies orthopedic anomalies
VATER: �Vascular and vertebral defect �Anal atresia and other GI atresia �TE fistula �Renal and radial anomalies �The more common cardiac anomalies: VSD Coarectation of aorta TOF ASD
Preoperative Evaluation and preparation
What problems concern you and what laboratory do you need to evaluate these problems? �Infants with TEF may have pneumonia or atelectasis secondary to aspiration of secretiont that cannot be swallowed or to reflux from the stomach �To evaluate this condition a CXRay is needed
�Other complication expected when the diagnosis is delayed: sepsis Shunting Hypoxia Hypercarbia Metbolic acidosis(secondary to dehydration) Respiratory acidosis
LAB data that you need: �ABG �CBC �U/A �Type and cross match
�Once the Dx is made the infant is placed in the head up- face down position. �The upper pouch is placed on continuous or intermittent suction �If atelectasis or pnumonia is a prominent feature , endotracheal intubation with ventilatory support may be required.
�Care must be taken not to overdistent the stomach, which could be rupture. �Gastrostomy may be required if distention of the stomach prevents adequate ventilation.
Risk classification of infants with TEF:
criteria of Waterson includes five group: �Group A: BWt > 2500 gr and well �Group B 1: BWt 1800 -2500 gr and well �Group B 2: BWt >2500 gr , moderate pneumonia and congenital anomaly �Group C 1: BWt < 1800 gr �Group C 2: BWt >2500 gr and severe pneumonia and severe congenital anomaly
�Infants classified in group A could be operated on immediately with definitive correction undertaken. �Those infants in group B 1 and B 2 could safely undergo a staged repair. �Group C 1 and C 2 presented the greatest challenge, and surgery should be delayed in these cases.
Survival rates: � 100% in group A , B 1, B 2 � 22% in group C 1 � 59% in group C 2
New classification (montreal classification) �Include just two groups: high risk group: with life-threatening anomalies or both a major anomaly and ventilator dependence. Low risk group: that includes all other patients.
Fluid replacement for this infants: �Fluid replacement should be conservative. �Approximately 4 ml/kg/h should be sufficient, with allowances for suction and gastric drainage and blood loss. �Special care is required to prevent fluid overload (because of the highe incidence of congenital cardiac disease associate with TEF) �A solution of dextrose 5% in ¼ strength normal saline may be used.
�The use of a halter pump or similar device will prevent adminstration of excessive fluid. �When administering intravenous drugs or anesthetics the site of adminstration should be as close to the entry site of the infusion possible. �To ensure that the medication reaches the patient , small measured flush volumes may be used and should be calculated in the total volume of fluid adminstered.
Role of antibiotics preoperatively or postoperatively: �It is standard practice to use preoprative antibiotics to control pulmonary infection. specifically a broad spectrum antibiotics is used. Postoperatively , antibiotics are used for the same purpose. In addition antibiotics are used to control infection if there is anastomotic leak.
Role of gastrostomy in the management af TEF: � gastrostomy may be preformed as a first step. It will decrease the possibibility of gastric distention and prevent reflux of gastric contents in to the lung. �Gastrostomy can be preformed during the definitive repair. �In some cases, as in acute distention of the stomach with elevation and immobilization of the diaphragm, gastrostomy may be a lifesaving maneuver.
�If surgery is delayed and a gastrostomy is not performed, TPN can be employad successfully. � Gastrostomy may interfere with ventilation. if the resistance to air passage is greater in the lungs than in the stomach, airflow will be preferentially directed toward the stomach.
This can be prevented by placing the gastrostomy catheter under water seal of approximately 20 cm H 2 O. �During surgery, and especially during induction of anesthesia , it may be necessary to totally or partially clamp the gastrostomy tube, if maintenance of ventilation is difficult.
What premedication is indicated in this patient? �Atropine is indicated to decrease secretion and to prevent the bradicardia associated with halothane anesthesia. �Dose of atropine 0. 01 to 0. 03 mg/kg IM(min dose 0. 1 mg) �Sedation is not required preoperatively.
Intraoperative Management:
The problem of transport of this infant to the operating room: �Every effort must be made to prevent or control the aspiration of secretion from the blind upper pouch and to prevent reflux of gastric contents through the fistula into the trachea and lungs. �For this reason the blind upper pouch is maintained on suction as established in the preoperative period.
�Since infants are obligate nasal breather, the suction catheter should be passed via the mouth rather than the nose. �Maintaining the 45 degree head up-face down position used in the preoprative period will further help in preventing aspiration. �The infant should not transported to the OR until all preparation have been completed. this include the warming of the room to 25 C.
What type of monitoring would you use for this case? �An ECG and a reliable blood pressure monitor are mandatory. �In children with complicated cardiac lesions an intraarterial cannula will permit frequent blood gas sampling as well as blood pressure monitoring. �A precordial stethoscope will monitor both respiratory and cardiac rates and quality. it will also detected the presence of secretions.
�An esophageal stethoscope is not indicated because of the danger of perforating the blind upper pouch. �Pulse oximetry and end-tidal CO 2 monitoring are standard. �Blood loss should be measured accurately. �Urine output should be measured and serial hematocrits may be helpful.
�Temperature must be monitored throughout the procedure. �The anesthesiologist must be careful to maintain normothermia by using : overhead heaters termal mattress warm operating rooms bair hugger or similar device fluids and blood should be warmed. �Humidification of the inspired gases will help to maintain normothermia o
What emergency drugs should be available? v For bradycardia: Atropine diluted to 0. 04 mg/ml. give 3 to 4 ml or 0. 12 to 0. 16 mg v Isotropic agents: Calcium chloride 20 mg/kg Epinephrine 1 mg/ml diluted to 0. 1 mg/ ml. give 0. 1 ml/kg v To produce peripheral vasoconstriction: Phenylephrine 0. 1 to 1 microgr/kg
The problems of induction and intubation: �Gastric distension and immobilization of the diapheragm �Bradycardia and severe cardiac depression(secondary to gastric dilatation) �For this reason, spontaneous respiration is preferred to assisted or controlled respiration during induction , until the fistula has been ligated.
�Frequently the infant can be intubated while awake after preoxygenation, but a struggling infant can regurgitate from the stomach into the trachea by way of the distal fistulous tract. �If a prior gastrostomy has been performed, the anesthetic gases may pass out of the lungs into the stomach. partial clamping of the gastrostomy tube may be necessary.
Where would you place the ET tube in relation to the fistula? �The ET tube should be large enough to permit easy suctioning and a small leak. �This will also prevent gastric distention when assisted or controlled ventilation is employed. �Salem has advocated using an ET tube without a Murphy eye, placed first into the right mainstem bronchus and then withdrawn until breath sounds are heard bilaterally but not over the stomach.
�The ET tube is placed with the bevel facing anteriorly. �The tracheal opening of the fistula is thereby blocked by the ET tube. this supposes that the opening of the fistula is above the carin and posterior in the membranous portion of the trachea. �In this case using an ET tube with a Murphy eye will ensure adequate ventilation of the left lung even if the ET tube enters the right mainstem bronchus.
�another method of dealing with the fistula involves the use of fogarty baloon catheter inserted into the fistula most commonly located in the posterior membranous portion of trachea. �This is done under fiberoptic control prior to intubation and prevents overdistention or loss of anesthetic gases. �One complication of its use is that the catheter can slip back into the trachea. �The infant then becomes diffcult to ventilate and the situation can be confused with surgical kinking of the trachea.
In what position would surgery be performed? how would this affected the management of the patient? �Gastrostomy is performed in the 45 degree head up position , but the difinitive repair requires that the infant be placed in the left lateral position , and the thoracotomy performed under the right scapula in the forth or fifth interspace. � 5% of patients with TEF have a right aortic arch, wich can complicated the repair in this position. a left thoracotomy repair is generally required in these cases.
�In the left lateral position, secretions from the right upper lobe can be a problem, draining into the trachea and the dependent lung. frequent suctioning may be needed to prevent obstruction of the endotracheal tube. �Traction on the upper lung is common during surgery and may kink the bronchus of the dependent lung. �A stethoscope placed in the dependent axilla will aid in the diagnosis of airway obstruction caused by blood purulent drainage , or kinking.
What problems can be anticipated during surgery? What anesthetic agent would you use? how can a stable mediastinum be accomplished? is there a role for muscle relaxants? �During repair of the esophagus, a stable mediastinum is essential for a good result. �A nondepolarizing muscle relaxant can be used for muscle relaxation. �controlled ventilation is used , and a small amount of CPAP may be needed to maintain mediastinal stability.
�Endobronchial intubation can occur at any time during the procedure and must be corrected. �Blood or mucus can obstruct the ET tube and must be suctioned. surgical manipulation can obstruct the ET tube or trachea. �Bradycardia can occure from traction and required treatment with atropine ( 0. 01 to 0. 02 mg /kg) �Frequent expansion of the collapsed or retracted lung is advocated by some anesthesiologist.
�No specific anesthetic agent is required or prohibited. �The use of nitrous oxide as part of the anesthetic regimen will decrease the inspired oxygen concentration , thereby avoiding the hyperoxia associated with retinopathy and retrolental fibroplasia in the premature infant. �It is recommended to keep arterial oxygen saturation between 90% nd 95% to prevent oxygen toxicity.
Postoperative Management
When can this infants be extubated? �If a nondepolarizing muscle relaxant has been used, and the infant is normothermic and there are no serious pulmonary problems, the relaxant can be reversead. �The anesthetic agent should be discontinued early enough to permit spontaneous respiration. �Most patient with an early diagnosis and no pulmonary complications , can be extubated at the end of surgery.
�The ET tube should be suctioned and the lungs inflated with oxygen prior to extubation. �Care is taken to avoid stress on the suture line. �During surgery a catheter may passed from above over which the repair of the esophagus is accomplished. �this catheter is used to measure the depth of the repair. The catheter is withdrawn on completion of the repair to a point above the suture line. this is measured on the catheter and recorded. all catheters are marked at this point and no suctioning beyond this depth should be done.
�If pulmonary complications are present postoperative mechanical ventilation may be needed. �when mechanical ventilation has been employed , it is recommended to extubate when mandatory intermittent ventilation has been discontinued the Pa. O 2 is >50 mm Hg and Pa. CO 2 is<50 mm Hg On an Fi. O 2 of 50%.
�In those infants with RDS in whom only a gastrostomy is performed without ligation of the fistula, mechanical ventilation may result in life-threatening air leaks. �this can be managed by placing the gastrostomy tube under 20 to 25 cm H 2 O or by passing a baloon fogarty catheter retrograde via the distal esophageal segment to occlude the fistula.
What are the dangers of hypothermia? �Hypothermia can affect the physical characteristics of inhalation anesthetics as well as the pharmacokinetics of intravenous agents. �Hypothermia lowers MAC of inhalation anesthestics, increase tissue solubility, and decreases requirements of nondepolarizing muscle relaxants, barbiturates , and narcotics. �Metabolism may double during light anesthesia.
�If set core temperature is not maintained by passive techniques, apnea overdose hypoventilation and metabolic acidosis occure. �Light anesthesia increases metabolism in response to hypothermia. �Norepinephrine release results in peripheral and pulmonary vasoconstriction with an increase in right-to-left shunting, acidosis, hypoxemia, and anaerobic metabolism.
Complication seen following TEF repair: Complications that existed prior to surgery , such as : � a continuing pneumonia �and problems related to other congenital anomalies, especially those involving the cardiovascular system.
Complications that occur as a result of surgery, such as: o pneumothorax , atelectasis, anastomotic leaks, esophageal stricture, subcutaneous emphysema, recurrent laryngeal nerve injury, recurrent fistula, and tracheomalacia. o o A late finding of impaired pulmonary function has been documented. o The principle causes of death are pulmonary complications, associated anomalies, and anastomotic leaks.
Management of postoperative pneumonia or atelectasia. Are these anesthetic complication? �Pulmonary complications are treated with antibiotics, suctionings, highe humidity, chest physiotherapy, and the promotions of crying. � These are probably not anesthetic complications, but are the result of traction on the lung during surgery or preexiisting infection from reflux or aspiration. �care must be taken at the end of surgery to reinflate he lungs and suctions the trachea adequately.
�When the anastomosis is complete, a catheter previously placed through the defect is removed to a point just above the anastomosis. the length of the catheter at this point is marked and recorded before being removed completely. �No suctioning should be deeper than that mark.
�If atelectasis develops in a previously extubated infant, the child is reintubated, suctioned , and ventilated after this the child may be extubated. �Hyperextension of the head and neck will place stress on the anastomosis and must be avoided. �it may be necessary for the infant to remain intubated and mechanically ventilated. �Under these circumstances the position of the endotracheal tubeis critical. the endotracheal tube must not extend to the anastomotic site.
THANK YOU