In the name of GOD Case presentation Dr





























, usually PAS+ diastase sensitive (glycogen),")

(q 24; q 12) or t(21; 22)(q 22; q 12)")

. •")


 • Overexpression of")




- Slides: 45
In the name of GOD
Case presentation Dr Azar baradaran Resident: Dr behnaz sabaghi
19 years boy without past history presents with fatigue, loss of energy and severe bone pain.
Radiologic study show multiple blastic lesion in bones. In lab data patient had increased ESR.
Panel 1
LCA
CK
CD 138
CD 20
CD 10
CD 99
S 100
CK 7
Ki 67
PLAP
TTF 1
CDX 2
Chromogranin
Step 2
Vim
Melan A
PAS
PAS+diastase
Ewing sarcoma/PNET
Clinical features ================= Usually ages 5 -20 years. May present with pain, fever, weight loss, leukocytosis and increased erythrocyte sedimentation rate mimicking osteomyelitis.
Sites: marrow of femur, tibia, humerus, fibula, pelvis, ribs, vertebra, mandible, clavicle; may permeate cortex and invade soft tissue.
Radiographic changes ============================= �Cortical thickening and widening of the medullary canal. �With progression of the lesion, reactive periosteal bone may be deposited in layers parallel to the cortex(onion-skin apearance) or at right angles to it (sun-ray appearance)
Typical ill-defined quality, with extensive involvement of medulla and cortex associated with elevation of periosteum
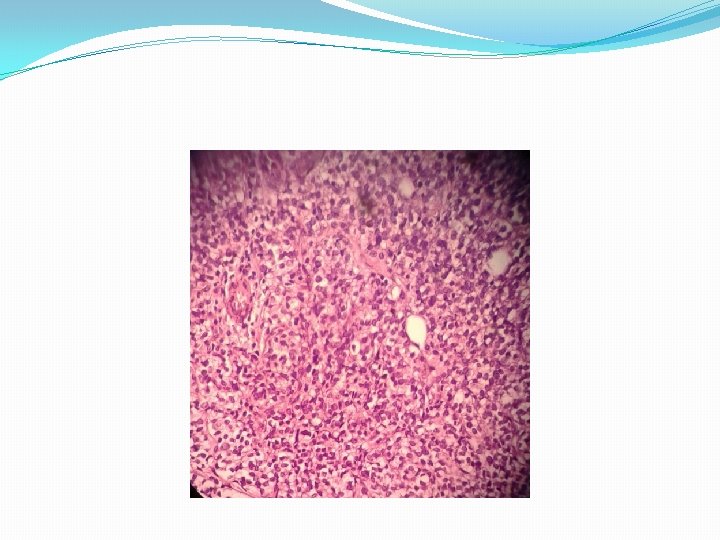
Microscopic feature: • Solid sheets of cells divided into irregular masses by fibrous strands. Individual cells are small and uniform. The nuclei are round, small nucleoli, and variable but usually brisk mitotic activity. • Well-developed vascular network. • Necrosis is common. • May have Homer-Wright rosettes (central fibrillary space) or pseudorosettes (cells arrange themselves around vessels).
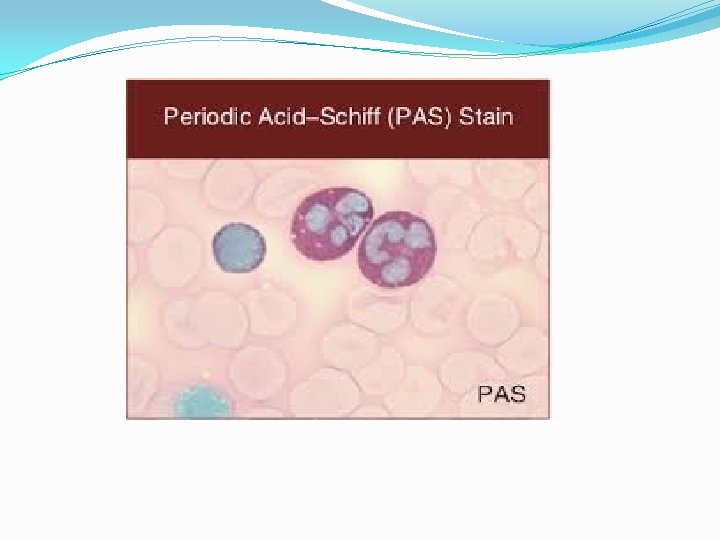
Positive stains • CD 99 (O 13, MIC 2), usually PAS+ diastase sensitive (glycogen), NSE, Leu 7/CD 57, FLI 1 protein, vimentin. • Variable low molecular weight keratin, variable synaptophysin.
Negative stains • S 100, CD 45/LCA, muscle markers, vascular markers.
Molecular description • t(11, 22)(q 24; q 12) or t(21; 22)(q 22; q 12) in 95%. • Fusion of the EWS(Ewing sarcoma) gene at 22 q 12 with the FLI 1 or ERG gene.
Electron microscopy description =========================== Undifferentiated tumor cells with multiple small foci of cytoplasmic glycogen are joined by two rudimentary cell junction.
Spread and metastases • The lung and pleura. • Other bones(particulary the skull). • CNS. • Regional lymph node(rarely). • About 25% of the patients have multiple bone and/or visceral lesion at the time of presentation.
Treatment: Preoperative chemotherapy, surgery, radiation therapy.
Poor prognostic factors • Extraosseous location. • Soft tissue extension. • Metastases. • Surgical margins. • Grossly viable tumor post chemotherapy. • possibly filigree pattern. • Neural differentiation.
• Type of gene fusion(expect of EWS-FLI 1 type fusion) • Overexpression of TP 53. • MYC. • Deletion of INK 4 a. • Aneuploidy.
Differential diagnosis: • Lymphoblastic lymphoma. • Desmoplastic small cell tumor. • Embryonal/alveolar rhabdomyosarcoma.
Desmoplastic small round cell tumor High grade malignant neoplasm, usually of peritoneum or other serosal surfaces, rarely in bone or soft tissue.
LYMPHOMA LCA+, TDT+, older patients, polymorphic infiltrate.
Embryonal/alveolar rhabdomyosarcoma • Loss of cellular cohesion so cells appear to float in alveolar spaces. • Posive for actin, desmin, myo. D 1.