Improving Patient Safety Using Health Information Technology Eric












 Ø Effort to decrease prescribing teratogenic medications to")






- Slides: 23
Improving Patient Safety Using Health Information Technology Eric G. Gayle, MD F. A. A. F. P IFH-Bronx Regional Medical Director and Regina Ginzburg, Pharm. D. Clinical Pharmacy Faculty, BI Family Medicine Associate Clinical Professor, St. Johns University
Medication Errors & Preventable Adverse Drug Events Ø At least 1. 5 million preventable ADEs occur each year in the United States l ~1/3 occur in the outpatient setting Ø Cost per preventable ADE: ~$2, 000 Ø National annual cost: $887 million Ø The numbers above are likely an underestimation! Preventing Medication Errors: Quality Chasm Series http: //www. nap. edu/catalog/11623. html
Electronic patient records and patient safety legibility communication Point of care interactions EHR “Electronic pharmacy” capabilities
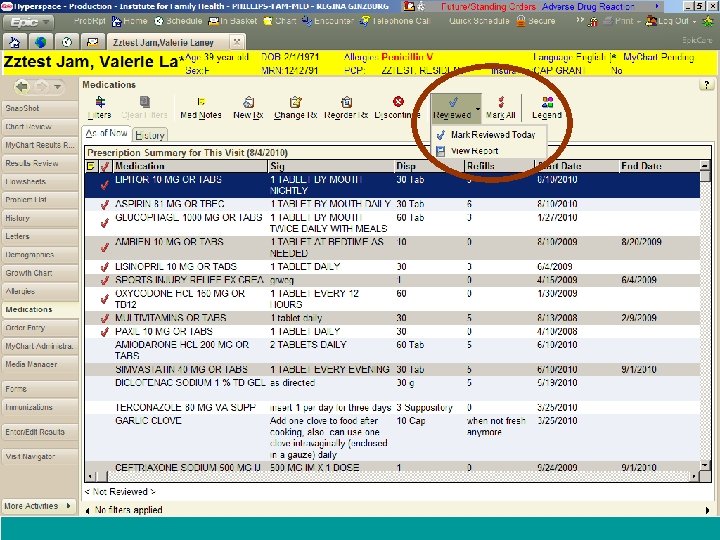
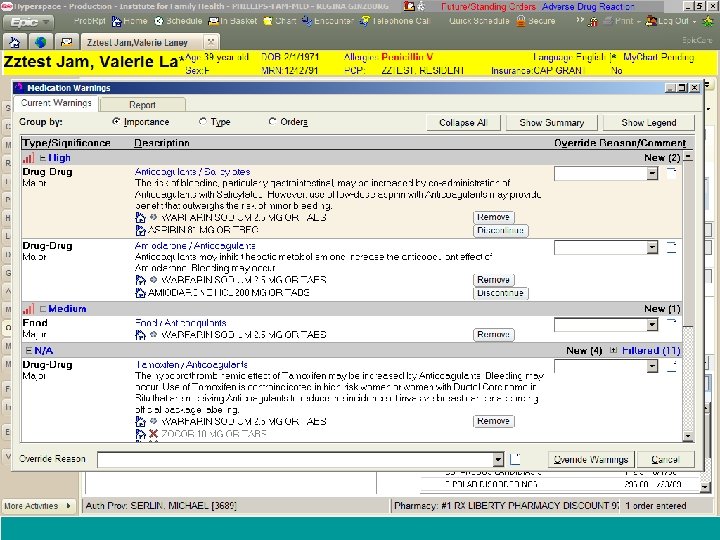
Effective Error-Prevention Strategies Ø Improving Patient-Provider communication l l l Verify active medication list with each encounter Review the name and purpose of the selected medication. Discuss when and how to take the medication. Discuss important and likely side effects and what to do about them. Discuss drug-drug, drug-food, and drug-disease interactions. Review the patient’s role in achieving appropriate medication use
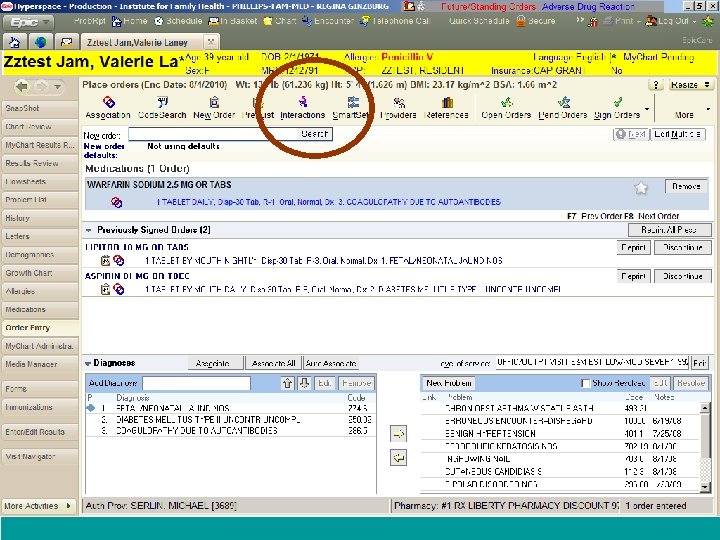
Improving patient safety using Health Information Technology Eliminates transcription errors Point of care checks and reviews “Electronic Pharmacy” within the EHR Electronic prescribing Improves patient medication history documentation
Effective Error-Prevention Strategies Ø Electronic prescribing
Ways to Improve Medication Errors Using HIT Ø Auto-calculated dosing for special populations l l l Weight-based formula incorporated for certain medications Correct dosage should appear in the directions field for specified patient weight must be documented in current encounter
Auto-calculated dosing: Impact of Intervention Ø Retrospective chart review looking rate of medication errors in our pediatric patients who were prescribed this medication before and after intervention l l N=316 (Pre) and 224 (Post) Number of medication errors • Pre: 103 (32. 7%) • Post: 46 (20. 6%) p=0. 002 l Significantly fewer strength overdosing errors in postintervention group • OR 0. 431 (95% CI: 0. 175 -0. 964) [p=0. 028] Ginzburg et al. Am J Health-Syst Pharm—Vol 66 Nov 15, 2009
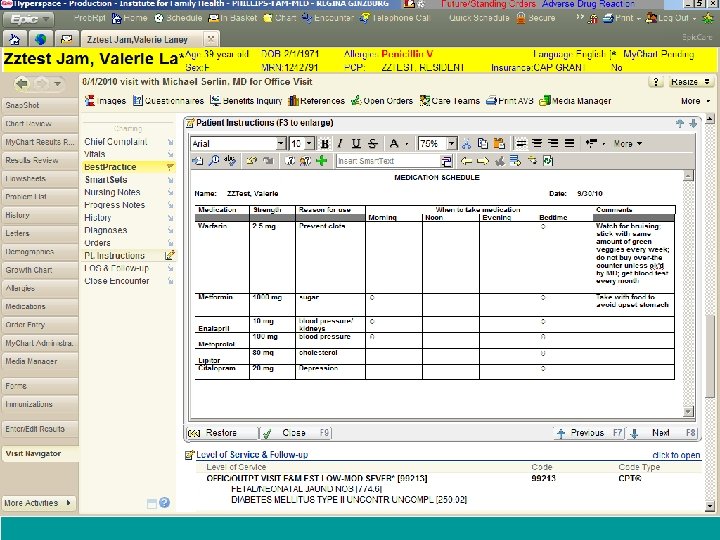
Effective Error-Prevention Strategies Ø Access to evidence-based references
Patient Safety Management Review new drug information from FDA Develop medicationrelated policies Pharmacy and Therapeutics Committee Review and update medication formulary Build “smartsets” within EHR to reflect policies
P&T Committee Ø Monitor medication effects and risk for use l l FDA warnings, latest guidelines/position statements, new major RCTs Committee’s decision based on levels • • Level 0 – no action Level 1 – “Inbasket” to all providers Level 2 - Inbasket + BPA Level 3 – advise HCP to cease prescribing
Monitoring Adverse Drug Reactions Provider detects an ADR event ADR diagnosis is entered during encounter Patient chart is flagged and sent to P&T Pharmacist reviews chart and determines if ADR needs to be submitted to Medwatch
Impact of Best Practice Alerts (BPAs) Ø Effort to decrease prescribing teratogenic medications to women of reproductive age l Phase I: • chart review determining the degree of need • 679 electronic charts reviewed • Primary outcome measure l l absence of a documented contraception plan or documentation that patient is low risk for pregnancy • Exclusion: Active contraceptive on medication list, IUD documented under procedure section, hysterectomy documented in surgical history
Results of Phase I Ø 51. 3% of women were prescribed a potential teratogen and were considered high risk for pregnancy Ø No easy way to see if discussion took place with patient regarding potential teratogenicity Ø
Implementation of BPA Ø BPA will alert providers that they are ordering a potential teratogen for a women who is b/w 14 -49 y/o Ø Exclusion criteria: l l Active contraceptive on medication list Has IUD documented under procedure Has hysterectomy documented in surgical history Has pregnancy or abortion diagnosis
BPA link to “smartset” Ø Progress note to blow in. Provider can choose 1 of 3 notes l Discussed risk and benefits. • Patient is sexually active, current method of contraception is document. • Patient understands risk if becomes pregnant. Patient is not currently sexually active. • Patient understands risk if becomes pregnant. Patient is only sexually active with women. Ø Link to contraceptive management diagnosis
Future needs to improve safety Ø How to improve integration of OTC meds/ supplements with the Patient’s EHR Ø Two way communication between providers and hospitals- Bronx RHIO project ongoing. Ø One patient one chart concept
The Unmarked Territory… Ø More research is needed for ambulatory care areas using HIT!!
Questions? ? ?