IMPROVING ACCESS TO BEHAVIORAL HEALTH ACCESS ADDICTIONS TREATMENT

IMPROVING ACCESS TO BEHAVIORAL HEALTH & ACCESS ADDICTIONS TREATMENT IN A RURAL CRITICAL ACCESS HOSPITAL DISTRICT ACCESS THROUGH COMMUNITY‐ACADEMIC PARTNERSHIPS Telehealth Alliance of Oregon 2019 Summit Program (Portland, OR) May 14, 2019 Wayne Pollard MSW LICSW Ryan Kimmel MD, Shane Mc. Guire, CEO Matt Iles-Shih, MD, MPH Anna Ratzliff MD, Ph. D Cara Towle RN MSN MA

DISCLOSURES ü No conflict of interest/disclosures

LEARNING OBJECTIVES Using the Columbia County Health System’s experience, this presentation explores: 1. An approach to envisioning & planning for systems change 2. Several options for integrating behavioral health & addictions treatment (BHAT) into general medical settings 3. Key components of & considerations in cross‐system implementation of BHAT 4. How this system’s experience with multilevel integration might inform your own efforts.

PRESENTATION OUTLINE • Background: – Behavioral health & addictions treatment in rural settings – Columbia County Health System, a case study • Pragmatic Innovation: – Developing a Vision, Identifying Needs & Service Goals – Inventory of local capacity, augmenting through partnership – Designing and implementing a program: • Inpatient • Outpatient

BACKGROUND Good News! Accessing behavioral health & addictions services improves many general health & mental health outcomes Integrating these services into general medical settings improves access and utilization Katon WJ. Clinical and health services relationships between major depression, depressive symptoms, and general medical illness. Biol Psychiatry. 2003; 54(3): 216 -26. Katon WJ, Lin EH, Von Korff M, et al. Collaborative care for patients with depression and chronic illnesses. N Engl J Med. 2010; 363(27): 2611 -20.

BACKGROUND A Challenge: • Access to Behav. & addictions services especially limited in rural areas • 75% WA’s counties & majority of its landmass is rural Thomas KC, Ellis AR, Konrad TR, Holzer CE, Morrissey JP. County-level estimates of mental health professional shortage in the United States. Psychiatr Serv. 2009; 60(10): 1323 -8. Andrilla CHA, Garberson LA, Paterson DG, Larson EH. The Supply and Distribution of the Behavioral Health Workforce in America: A State-Level Analysis. Data Brief #163. WWAMI Rural Health Research Center, UW, July 2017.
 Overview of CCHS Service Area §")
CASE STUDY – COLUMBIA COUNTY HEALTH SYSTEM (CCHS) Overview of CCHS Service Area § Region: Dayton, Waitsburg, Starbuck, & surrounding areas Ø Catchment : ~5, 600 residents § Demographics: Ø Older (median age = 50) Ø Rural (3 rd least populated county in WA, 4. 7 people/sq-mile)
 Overview of CCHS Service Area §")
CASE STUDY – COLUMBIA COUNTY HEALTH SYSTEM (CCHS) Overview of CCHS Service Area § Columbia County’s Health Ranking (out of 39 counties): Ø 37 th for longevity Ø 22 nd for aggregate health factors (e. g. , tobacco, diet, exercise, health care access & quality) Ø 14 th for social and economic health Ø 2 nd for physical environment § Mental/Behavioral Health: Ø 4. 2% describe MBH as poor (state ave = 3. 8%) Ø 29% of Medicare patients depressed, 14% dealing with anxiety Ø MBH provider-to-pt ratio = 440: 1 (state ave = 330: 1)
 Dayton General Hospital § Critical Access")
CASE STUDY – COLUMBIA COUNTY HEALTH SYSTEM (CCHS) Dayton General Hospital § Critical Access Hospital § Level V Trauma Center § Level III Cardiac & Stroke Center Booker Nursing Home § On Dayton Gen Hosp’s Campus Primary Care Clinics § Dayton § Waitsburg
 –OPPORTUNITIES System: § § Strong Leadership Dedicated & skilled clinical staff")
CASE STUDY (CCHS) –OPPORTUNITIES System: § § Strong Leadership Dedicated & skilled clinical staff Multiple care settings EHRs (inpt/outpt) Behavioral Health Care § Two MSWs LICSWs § No Psych ARNP or MD/DO
 –OPPORTUNITIES Addictions Treatment: § No specialists § 2 Buprenorphine-naloxone waivered providers")
CASE STUDY (CCHS) –OPPORTUNITIES Addictions Treatment: § No specialists § 2 Buprenorphine-naloxone waivered providers § Option for outpt psychosocial SUDs treatment at Blue Mountain Counseling Community/Pt Needs § Hosp-to-hosp transfers for multi-week IV abx (often due to IVSU) § Under-treated depression, bipolar, anxiety, OCD, PTSD, schizophrenia, addictions

DEVELOPING A VISION & PLAN FOR INTEGRATED CARE

CCHS’ VISION: REINFORCING GOALS Improved Access to Behavioral Health & Addictions Care Financial Sustainability & Resource Stewardship Improved Patient Experience Improved Patient Outcomes Improved Provider Experience, Support, Efficacy, & Productivity High Quality of Care

GOALS Now Future Patients in crisis and distress +/- + Patients with common chronic mental illnesses such as depression and anxiety. +/- + + - + +/- + Which patient populations are we targeting? Patients needing support to manage serious, chronic and persistent mental illness. Patients in the Inpatient Setting What capacities do we have and need to develop? Measurement‐based treatment to target Commitment to population‐level outcome improvement www. safetynetmedicalhome. org/sites/default/files/GROW-Pathway-Planning-Worksheet. doc

RESOURCES Geography What resources does CCHS have? What resource challenges need to be addressed? Care team and workforce development CCHS (hosp, rehab, ED, PC, palliative care, PCBH), Limited access to other specialty care Blue Mt Counseling, hospice, referral to Tri-Cities PC clinic, nursing home, ED, Hosp on same No concerns/new space requirements campus; distant satellite PC clinic Engaged, willing to innovate/experiment Continued support ($, messaging, coordinating process changes) Stable, dedicated teams Training & incorporation of any new approaches, staff Shared workflows Inpt (limited BH workflow); PC (screening, PCBH) Depends upon mix of BH approaches Available technology/ HIT 2 EHRs, small onsite IT dept Possible telehealth, registry functions Financial resources Some support from ACO, ACH, WRHAP; prior budget for co-located psychiatrist Financial Plan for (1) program devel. & then (2) ongoing clinical care Physical space Support of leadership
: PRIOR & CURRENT SERVICES Existing & Previous Behavioral Health & Addictions Treatment")
RESOURCES (CONTINUED): PRIOR & CURRENT SERVICES Existing & Previous Behavioral Health & Addictions Treatment § Co-located outpatient psychiatrist – Long-term Psychiatric Care (2016 -2018) § Co-located outpatient MSW LCSW - Brief Interventions & Longer-term Therapy (9/2017 -Present) § Dedicated inpatient and outpatient clinical staff, without specialty training § A local community behavioral health service, providing primarily psychotherapy
: NEEDS Needs Identified (by patients, clinical staff, administration): § Support for Addictions")
RESOURCES (CONTINUED): NEEDS Needs Identified (by patients, clinical staff, administration): § Support for Addictions Treatment (Inpatient and Outpatient) § PCP access to consultation regarding management of psychiatric disorders § Patient interest in direct access to both therapist & psychiatrist § Managing no only acute events but treating a population over time § Integrating care across clinical settings (inpatient, outpatient, residential/nursing home)

OPTIONS Potential strategies & their challenges: • Facilitated referrals – Patients’ access a challenge • Optimize use of existing local resources – Largely optimized • Develop local resources, de novo – Expensive, logistically challenging • Hire new on‐site providers – Historically, a significant challenge (for psychiatric ARNPs, MDs, psychologists), +/- costeffective • Find an External Partner: – Limited local partners – No established model for integrated services across the inpatient consult and outpatient within a Critical Access Rural Hosp District

OPTIONS: EXPLORING APPROACHES TO INTEGRATION Building a Community‐Academic Partnership – CCHS reached out to & partnered with University of Washington Collaborative Exploration: – What approaches exist & which facilitate: • Rapid access to assessment & short-term management of acute issues • Longitudinal care • Population-based care – Which are evidence-based? – Which are viable in the CCHS contexts? • Inpatient vs. Outpatient
 Co‐Located Consultation (in‐person or telemedicine)")
APPROACHES TO INTEGRATION: INPATIENT Peer‐to‐Peer Consultation (formal & informal) Co‐Located Consultation (in‐person or telemedicine) Full Consult‐Liaison Service Variable access More regular access Good access & communication, regular follow‐up Only indirect assessment Direct assessment Team‐based, often multispecialty Low Cost Potential for waitlists and provider availability issues Expensive Often One Pass Variable ability for follow‐up Strong evidence base
 Limited Access Primary Care")
APPROACHES TO INTEGRATION: OUTPATIENT Traditional Consultation / Referral Co‐Location (Often) Limited Access Primary Care Behavioral Health Collaborative Care Management Access and interaction Solidly grounded in a clinical practice culture Requires shifts in practice Limited feedback Better communication Embedded BHP & Psychiatrist Expensive (in aggregate) Can “fill, ” develop long waitlists limited access Rapid access to brief behavioral interventions Pop. ‐based, treat‐to‐ target, medium‐ duration, mixed behav/rx interventions +/‐ One Pass +/‐ Limited ability for follow through Evolving evidence base Solid evidence base (in‐person or telemedicine)

OPTIONS: EXPLORING APPROACHES TO INTEGRATION Collaborative Exploration: – What mix of approaches would be feasible, efficacious, cost-effective? …and in which contexts? – Inpatient psychiatric & addictions needs • Telepsychiatry • Clinical Peer-to-Peer (zoom, phone, email) – Outpatient psychiatric & addictions needs: • • Continued PCBH functions Collaborative care Telepsychiatry Clinical Peer-to-Peer (phone, email) – Other: • Booker Nursing Home: access to PC services plus psychotropic review

WORKFLOW Identifying changes needed in order to deliver integrated behavioral health Does staff need to be hired? What types of staff? Do existing or new staff need to be trained? Training for Co. CM; 1 new BHC What facilities, HIT, and other resources are required to implement the integrated workflow? TM hardware, Zoom, Patient Registry What internal communication materials and protocols, and practice‐specific guidelines and protocols for psychiatric emergencies do we need? Protocols for patient screening, enrollment, scheduling, conducting visits; clarify protocols for psych emergencies How will our physical space foster collaboration? No concerns/needs identified Fliers for staff and patients; Staff/provider meeting with UW partners (site visits) New schedule for BHCs (controlled by BHCs), with changes in appnt/blocks distribution What materials do we need to introduce the new care delivery pathway to patients and practice clinicians and staff? How will we schedule visits? Will we schedule follow‐ups interspersed with open access appointments to facilitate time for just‐in‐time consultations and warm handoffs? When and how will we evaluate our progress? What would be the next step if we don’t reach our goal? How will we know we are not just going through the motions? New quality metrics, patient symptoms and outcome tracking through outpt registry

ADMINISTRATIVE & TECHNICAL • Credentialing & Privileging – With direct pt care (i. e. , telemedicine), full credentialing & privileging for all CCHS sites where pts where seen. • Liability – Covered by UW (CCHS sites designated “site of practice” • HIT – 2 EHRs (hospital & clinic) - Consultants trained, granted remote access – EHR privileges: • Unrestricted “read” capacity • Ability to generate documents within medical record • No orders, prescribing – New HIT • Registry (Patient Tracker), Zoom, TM Laptop & Cart

FINANCES ‐ BILLING CCHS payers/insurance – UW consultants needed to be credentialed with insurers – Telepsychiatry: • G-codes – Collaborative Care • Fee for Service • Co. CM G-codes (not used to date) UW CCHS – Administrative (Devel / Implementation Support): – Clinical: • Inpatient Clinician-to-Clinician & Telemedicine: – Fee for service hourly rate • Collaborative Care: based on panel size and number of BHCs – 1 full panel (30 -80 pt), 1 BHC = 3 hrs of Co. CM plus 1 hr of telepsychiatry per week • 4 hr at standard hourly rate

CCHS INPATIENT INTEGRATED CARE APPROACH

INPATIENT CONSULTATION • Access: – M-F, 9 AM-5 PM – Contact: • 1 hr/day Hospitalist-to. Consultant “curbside” (9 AM 5 PM) • 1 hr/day Direct Pt-toconsultant Telemedicine Visit

INPATIENT TELEMEDICINE • Equipment: – UW Consultant: • desktop computer • Logitech C 920 camera/microphones • Zoom software – Dayton Gen. Hosp: • Laptop computer with builtin camera & microphone • Zoom software • Mobile cart

INPATIENT TELEMEDICINE • Process: – Pt ID-ed by Hospital Team – Hospitalist & Psychiatrist • discuss case (phone) • confirm plan for TM visit – Appnt sched by Hosp staff – RN & psychiatrist join secured Zoom meeting
: – RN: • Moves TM cart to patient room")
INPATIENT TELEMEDICINE • Process (continued): – RN: • Moves TM cart to patient room • Provides intro • Remains present for clinical encounter – Psychiatrist: • Conducts assessment, discusses dx impressions & treatment recs w/pt before visit ends • Contacts Hospitalist to discuss dx & treatment recs, completes noted in EHR

CCHS OUTPATIENT INTEGRATED CARE APPROACH

PHQ‐ 9 SCREENING WORK FLOW ‐ EXAMPLE Patient checks-in for PC or BH related appointment. Initial identification: – Universal screening (PHQ 9) – Targeted screening – Clinical presentation Front Desk Staff · Hands out PHQ 9 form to patients 18 and older Nurse/Medical Assistant Collects, scores, and data enters the PHQ-9 and GAD scores Score is: 10+ Score is: 0 -9 Nurse/Medical Assistant · If patient interested in IBH services, give PHQ-9 to BH care manager and have patient schedule appt. put PHQ-9 in BHC’s inbox · If patient not interested, give PHQ-9 to PCP to review · MA contacts BHC for a team hand-off if pt interested · If BHCM is available, give PHQ-9 to BHC, BHC to enter special populations patients into registry · If BHCM is not available, give PHQ-9 to PCP to review and have patient schedule f/u with BHC if interested. BHC is available. Behavioral Health Consultant (BHC) · Adds patient to their schedule & completes BH visit · Adds patient to registry and has patient schedule follow up appointment as needed BHC is not available. PCP · Reviews the form with patient • Assesses for suicidality and recommends follow-up appointment with BHCM

PRINCIPLE: POPULATION‐BASED CARE Caseload Overview – Utilizing a Registry © University of Washington Free UW AIMS Registry: (https: //aims. uw. edu/resource-library/patient-tracking-spreadsheet-example-data) • Proactive monitoring & engagement (“no one falls through the cracks”) • Shows who needs attention, prompting treatment adjustment • Facilitates communication among team 34

PRINCIPLE: MEASUREMENT‐BASED TREATMENT TO TARGET • Regular use of behavioral health measures to track response to treatment • Use of psychiatrists to help intensify treatment • Stepped care makes efficient use of behavioral health resources

WHY TRACK OUTCOMES • Proactive treatment adjustment – Avoid Patients staying on ineffective treatments for too long – Treatment plan “shelf life” = 10 -12 weeks max – Full, partial, no response • Know when to refer for consultation/get help 36

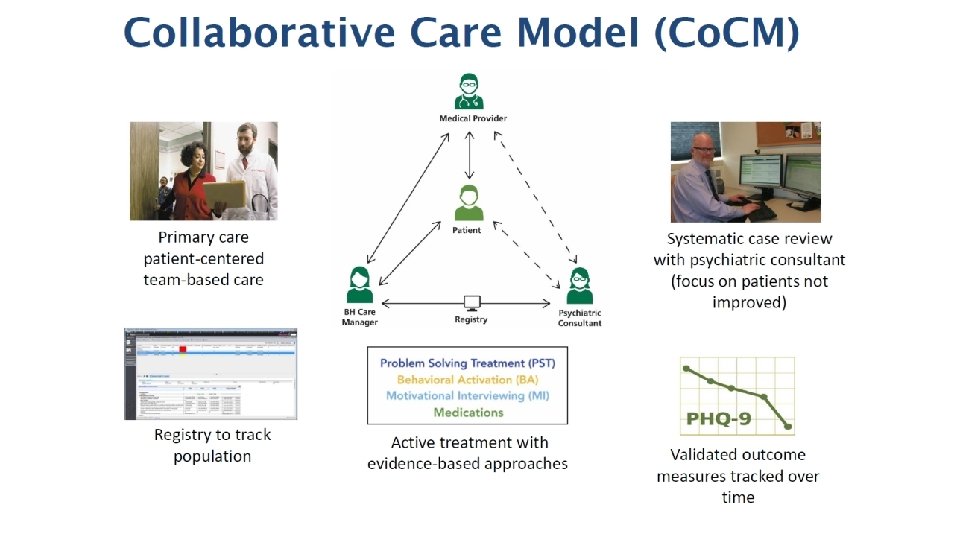
PATIENT‐CENTERED COLLABORATIVE TEAM Telemedicine PCP / MAT Prescriber Core Program New Roles Beh. Health Consultant / Care Manager Patient Additional Clinic Resources Other Community Resources Psych & Addictions Consultant

PATIENT‐CENTERED TEAM – PRIMARY CARE PROVIDER • Primary treatment relationship • Prescribes medication (including MAT) • Monitors medication management, together with care manager • Supports treatment plan • Consults with Collaborative Care team • Supports system change 38

PATIENT‐CENTERED TEAM – BEHAVIORAL HEALTH CONSULTANT • • Assesses & addresses urgent issues Facilitates patient engagement Performs systematic initial and follow‐up assessments Evidence‐based psychotherapy – Individual • Other functions – Behavioral health interventions focused on health behaviors – Addressing substance use – Coord of psychosocial services/interventions • Systematically tracks treatment response • Supports treatment plan with PCP • Reviews patients with the psychiatric consultant weekly 39

PATIENT‐CENTERED TEAM – PSYCHIATRIC CONSULTANT • Engage & Support PCP and Team • Review cases with BHC using registry – Scheduled (ideally weekly) – Prioritize patients that are not improving • Consult urgently (as needed) with PCP or BHC • Educational Components 40
 – Shared with inpt addictionfocused telemedicine")
OUTPATIENT TELEMEDICINE • Two hours per week (M/Th) – Shared with inpt addictionfocused telemedicine – Can be (1) Pt-to-Psych or (2) PCP-to-Pysch • Complex diagnostic or treatment

OUTPATIENT TELEMEDICINE • Prior to visit – Pt Identification & Prioritization • BHC, PCP, Pt referral • BHC controls schedule – Pt consented & appnt set by BHC • Day of Visit: – BHC & Consultant open Zoom Meeting – BHC greets, rooms, & introduces pt & consultant – Consultant consents pt to use of telemedicine, conducts assessment (45 min) – BHC joins final 10 -15 min; reviews dx, treatments recs – Consultant enters note in EHR

INTERLUDE: INTEGRATED ADDICTIONS …TREATING PEOPLE WHERE THEY’RE AT

BARRIERS TO ADDRESSING SUDS Resource Limitations: – Time (e. g. , not enough of it) – Other: treatment availability Comfort with… – Asking about SU: • Stigma (ours &/or out pts) • “It’ll undermine our relationship” – Treating SU (“great…now what do I do? ”) – “Opening Pandora’s Box” Assumptions: – “There’s no way Jenny’s an addict” – “Addiction is a personal failing, not a medical problem” – My pt’s not ready/able to change; my doctor will judge/misunderstand/be disappointed
 q. HR Goals:")
HARM REDUCTION q“Abstinence only” approaches don’t reach everyone (probably a minority) q. HR Goals: –Reduce harm from high-risk behaviors –Improve quality of life

ETOH: ALCOHOL WITHDRAWAL MANAGEMENT & Withdrawal Management: ØDoes pt need med‐managed withdrawal? § Currently has/likely to develop w/d syndrome Ø If “yes”, which setting? § Hx of complicated w/d, hx of recent use, CIWA, comorbidity Ø If ambulatory withdrawal rx appropriate, which rxs, follow‐up? Then what? Ø Develop and enact a recovery plan (psychosocial, MAT)

OUD TREATMENT: Where To Begin? Indications & Conditions for Rx: • Screen & dx opioid use disorder • Pt’s preferences & engagement • Clinical factors ID‐ed in Evaluation Rxs (MAT): • Buprenorphine • Methadone • XR-Naltrexone Potential treatment contexts: • Hospital • Residential Treatment • Specialty outpt addictions • Primary Care / general MH Psychosocial Tx: • MET, CMT, CBT, NA …& Rescue Kits: • Naloxone kits (Prescribe them!)

PATIENT‐CENTERED TEAM – HOLISTIC CARE PLAN • Whole person treatment Bio • Evidence‐based Medications – Bio. Psycho. Social • The treatment that WORKS is the best one Psycho • Evidence‐based Psychotherapeutic Interventions – Review all evidence-based tx options – Weigh pros & cons Social • Social support • Create shared care plan – Clear goals, roles, priorities 48
 – 50%-70% of patients need")
TYPICAL DURATION OF CARE MANAGEMENT • 6 Months (average) – 50%-70% of patients need at least one change in treatment to improve – Only 30 -50% patients respond fully to first treatment – Each change of treatment moves an additional ~20% of patients into response or remission 49

LESSONS FROM AN EXPERIMENT IN WHOLE SYSTEM INTEGRATION

OUTCOMES – PRIMARY CARE • Co. CM: – – Caseloads: 2 BHCs sharing 112 pts Early & Sustained Engagement: ~80% returning for f/u care, >90% in-clinic visits Symptom Response (Dep/Anxiety, snapshot of the active panel): 40%-50% Psychiatric Caseload Consultation: 1 hr per BHC per week (7 -12 pts/wk) • Telepsychiatry: – Access: 2 hours per week (2 pts/wk) • Booker Nursing Home: – Monthly 1 -hour team-based psychotropic review (5 -6 pts) • PCP‐to‐Psychiatrist Consultation: – Earlier, several calls per week; once Co. CM and TM established, now every other wk

CHALLENGES & OPPORTUNITIES: OUTPATIENT • Facilitating pt engagement/outreach – Phone visits, home visits • Psychosocial Interventions: – Linking to community services – Additional training in psychotherapy modalities • Optimize utility of TM time – Office hours with providers? • Monitoring: – Treatment plan implementation & adherence – SUDs screening and monitoring

CHALLENGES & OPPORTUNITIES: OUTPATIENT • Struggling Patients: – Early ID, more aggressive monitoring, treatment escalation for pts w/more severe symptoms/conditions – Clearer pathways & thresholds for referral to specialty care • More innovative approaches to enhancing provider skills • Further increasing capacity in Co. CM? • Closer work with community partners, relationships/coordination with non‐CCHS specialist

OUTCOMES – INPATIENT • Direct to Patient Telemedicine – More freq over time (1/mo 5/mo) – Reasons for Consult: initially SUDs-focused, increasing general psychiatric • Hospitalist‐to‐Psychiatrist Consultation: – Frequency: variable • Training/Education – Annual site visits

CHALLENGES & OPPORTUNITIES: INPATIENT • Defining optimal use of inpatient consultation: – Conditions/severity – Direct pt eval vs. peer-to-peer • Monitoring inpt treatment plan implementation & adherence • Ensuring smooth transitions in care; full system integration • Need new approaches to supporting providers – Targeted education – Finer gradation of clinical support (brief calls, email) – Development of resource libraries – Annual Site Visits quarterly video conf

WHAT QUESTIONS DOES THIS RAISE FOR YOU? What has been your experience with integration? Where might you go from here?
 Ryan Kimmel MD, Shane Mc.")
THANK YOU! (and our colleagues at CCHS and UW) Ryan Kimmel MD, Shane Mc. Guire, CEO Anna Ratzliff MD, Ph. D Cara Towle RN MSN MA …………. . .

RESOURCES – AN OUTLINE FOR IMPLEMENTING WHOLE SYSTEM INTEGRATION 1. Planning for Integrating Behavioral Health • Develop a shared vision for integrating behavioral health & addictions care across the organization. • Establish an integration planning and implementation team. • Develop an integrated care implementation plan. • Goals, Resources, Options, Workflow (GROW) planning process 2. Establish Operational Systems to Support Integration • Define types of patients who will receive integrated care. • Define roles for clinicians and staff in integrated care team. • Foster ongoing administrative support to integration. • Establish clear mechanisms for regular and effective communication among team members. • Design workspaces that maximize contact between behavioral health providers and medical clinicians. • Ensure appointment scheduling system allows patients to see integrated care team in timely manner. • Ensure a common medical record for behavioral health and medical care. • Begin to develop quality measures.

RESOURCES – AN OUTLINE FOR IMPLEMENTING WHOLE SYSTEM INTEGRATION Plan for Financial Sustainability • Ensure billing tools, payment systems in place for reimbursement. • Develop plan for sustained financing of integrated care. Obtain Behavioral Health Expertise and Build a Culture of Integration • Identify type of behavioral health services needed. • Identify skill sets and personnel needs and ensure these are met (e. g. , training or new hires/contracts) in a timely manner. • Train primary care and behavioral health providers to work as a team to provide integrated care. • Develop and maintain a culture of collaboration and teamwork. Tailor the Care Team to Meet the Needs of Patients Identified for Integrated Care • Develop an integrated care team designed to match the patients’ needs (composition and process. ) • Identify supervision and training needs and develop plan for meeting these.

RESOURCES – AN OUTLINE FOR IMPLEMENTING WHOLE SYSTEM INTEGRATION Establish Protocols to Identify Patients Who Could Benefit from Integrated Care • Develop and use a protocol (validated screening and initial diagnostic assessment) to identify patients who could benefit from integrated care. Develop Shared Care Plans for Patients in Need of Integrated Care • Develop protocol for creating shared care plans with & for patients in need of integrated care. • Ensure shared care plan is located in a single medical record. • Ensure processes are in place to primary care and behavioral health providers both work from the shared care plan. Educate Patients and Families about Integrated Services • Develop and rollout plan to educate all patients in need of integrated care (and their family members, where appropriate) integrated behavioral health care services.

RESOURCES – AN OUTLINE FOR IMPLEMENTING WHOLE SYSTEM INTEGRATION Provide Patient‐centered Integrated Care to Identified Patients • Perform behavioral health assessment • Provide caseload‐focused psychiatric consultation • Provide in‐person psychiatric assessment of complex patients • Patient education about symptoms & treatment options • Collaboratively develop, execute, & update Behavioral Health Treatment Plan – Brief Counseling, Activity Scheduling, Behavioral Activation – Evidence-based Psychotherapy (e. g. , PST, CBT, IPT) – Prescribe Psychotropic Medications

RESOURCES – AN OUTLINE FOR IMPLEMENTING WHOLE SYSTEM INTEGRATION Track Patients Identified for Integrated Care and Monitor Their Outcomes • Develop & utilize protocol to quickly identify patients not improving with treatment. • Develop & utilize protocol to adjust the care plan for patients who are not improving. • Develop & utilize protocol to identify patients who are struggling to engage or follow treatment plan. – – Reach out to Patients who are Non-adherent or Disengaged Track Patients’ Symptoms (e. g. , PHQ-9) Track Medication Side Effects & Concerns Track Outcome of Referrals & Other Treatments • Develop process for educating patients who have improved to recognize risk factors for and signs/symptoms of relapse as well as strategies to address these. • Develop criteria and process for program completion and mechanisms for monitoring post‐discharge status.

RESOURCES – AN OUTLINE FOR IMPLEMENTING WHOLE SYSTEM INTEGRATION Collect and Use Data for Quality Improvement • Systematically collect & track data on all patients identified to receive integrated care services. • Systematically track health outcomes for all patients receiving integrated care services. • Use collected data to improve workflow, processes, treatment approaches, to enhance quality of care provided to all patients in integrated care.

FINANCES: SUSTAINABILITY OF INTEGRATE CARE PROGRAM Full financial assessment complex & needs to be individualized: – What mix of services offered? – What mix of payers and payment arrangements? • Fee for service, case rate, fully capitated? • What reimbursement for which services requiring what clinical credentials? – Phases of Development/Service: • Startup Costs: existing vs. required resources, infrastructure, personnel, etc? • Ongoing care delivery costs – Differences in cost/benefit from using different combinations of professionals, partners/consultant? – How is team time and effort allocated; what are the program’s visit statisics? – Myriad possible indirect costs and benefits?

FINANCES: BILLING FOR TELEMEDICINE Key variables of payer policies include: • Telehealth modality (i. e. audio, video, store and forward, etc. ) • Originating site/location of patient (i. e. healthcare facility or clinic, rural, in home, etc. ) • Provider type (i. e. physician, nurse practitioner, clinical social worker, genetic counselor, etc. ) • Type of service – in some cases only certain CPT codes are allowed • Location of the provider (office, clinic, etc. ) • Individual’s plan (e. g. , Private, Medicare, Medicaid)

FINANCES: BILLING FOR COLLABORATIVE CARE Primary Funding Mechanisms • Traditional CPT Codes – Psychiatry, Psychotherapy, Health and Behavior, Screening, SBIRT – All require specific credentialing, licensure, and setting (varies by service and insurance) • Value‐based payments and pay for performance contracting with health plans – Accountability to metrics • Bundled Payment Models – Medicare and WA Medicaid CMS Payments for Psychiatric Collaborative Care (Co. CM) Differences in licensure, tx setting, & other billing requirement among payers

67
- Slides: 67