Implementing an Integrated Care Management Model in Vermont


 This project was supported by Funding Opportunity")
 (3) nonprofit organization designated by")











 ICM Conventional Care focused on social determinants of")


















- Slides: 38
Implementing an Integrated Care Management Model in Vermont: A Statewide Learning Collaborative to Improve Care Coordination for Persons with Complex Needs Bruce Saffran, BS, RN Vermont Program for Quality in Health Care, Inc.
No financial relationships to disclose
Integrated Communities Care Management Learning Collaborative (ICCMLC) This project was supported by Funding Opportunity Number CMS-1 G 1 -12 -001 from the U. S. Department of Health & Human Services, Centers for Medicare & Medicaid Services. The contents provided are solely the responsibility of the authors and do not necessarily represent the official views of HHS or any of its agencies. The research presented here was conducted by the awardee. These findings may or may not be consistent with or confirmed by the independent evaluation contractor. – Nationally-recognized initiative that helps health care providers meet the medical and social needs of people in their communities – State agency with regulatory authority over health care quality and pricing – State designated contractor/partner for health care quality and safety oversight, supporting health care reform initiatives
Vermont Program for Quality in Health Care, Inc. 501(c) (3) nonprofit organization designated by the Vermont Legislature in 1988 as an independent, non-regulatory, peer review committee. Our organization brings together the entire spectrum of health care voices to focus on quality analysis and improvement. Primary VPQHC staff that worked with the ICCMLC: Bruce Saffran, BS, RN – QI Facilitator worked directly with state agencies and 11 communities implementing ICM to develop and test tools and methods, collect, analyze and present data, develop and present learning materials Elizabeth P. Winterbauer, MPH, CPHQ – Epidemiologist provided detailed data analysis, technical, and reporting assistance
Background: Vermont’s Health Care Population • Rural state: mostly small and medium hospitals – smallest has 19 beds! • 14 public hospitals in Vermont, including one American College of Surgeons (ACS) Verified Level 1 Trauma Center (UVMMC) • Population 626, 042 (2015) • Aging/disabled residents are growing segments of the demographic • 35% of Vermonters have some kind of Medicaid benefit • Declining numbers of Primary Care Physicians and workforce in general • Long waiting times (days) in Emergency Departments for many Psych patients
Vermont Mental Health Provider Capacity Designated Hospitals • Adult – Level 1 involuntary: 45 beds Ø nationally 11. 7 “State Hospital Beds” per 100, 000 population, VT has about 7 per 100, 0002 • Adult – Non-Level 1 (involuntary and voluntary): 143 beds • Children and Youth: 28 beds Designated (Mental Health) Agencies • Adult Crisis Beds: 38 beds • Youth Crisis Beds: 12 beds • Adult Intensive Residential: 42 beds Peer Service Agencies • Adult Crisis Beds: 2 beds • Adult Intensive Residential: 5 beds State Secure Residential • Middlesex Therapeutic Community Residence: 7 beds Source: VT Department of Mental Health, January 12, 2017 2 Fuller, D. A. , Sinclair, E. , Geller, J. , Quanbeck, C. , & Snook, J. (2016). Going, gone: Trends and consequences of eliminating state psychiatric beds, 2016. Arlington, VA, Treatment Advocacy Center.
Background of the Problem:
Background of the Problem:
The Significance of Social Determinants of Health Bradley EH, Taylor LA, Rogan E. American Health Care: Spending More, Getting Less. Vermont Blueprint Annual Meeting, South Burlington, VT. 12 April 2016. Keynote Address.
Disruption: Tropical Storm Irene August, 2011
Disruption: Waterbury State Office Complex August, 2011 Post Tropical Storm Irene
Disruption: Vermont State Hospital, Waterbury Post Tropical Storm Irene
Selection of Tools, Methods, Protocols and Faculty • Vermont’s Practice Transformation Workgroup considered “how to improve team-based care coordination in Vermont? ” • Literature review to identify key best practices • Goal identified to use the PDSA model of QI to test methods to coordinate an individual’s care across a diverse team • A planning group comprised of local partners in each of the pilot communities met to identify key deliverables • Tools, workflows and methods were developed and customized at the local community level • National experts and local expert faculty identified and engaged
Project Objectives • Use data/intuition to identify persons with complex needs and/or high risk for ED/hospital use • Develop, test and implement promising tools and methods for Integrated Care Management • Enroll complex needs participants throughout the state • Measure the impact of the program • Provide ongoing support and training to engaged communities • Development of toolkit for communities and partners: http: //blueprintforhealth. vermont. gov/about-blueprint/integrated-communitiescare-management
Using Data to Identify Complex Needs Healthcare Hotspotting: Camden, New Jersey
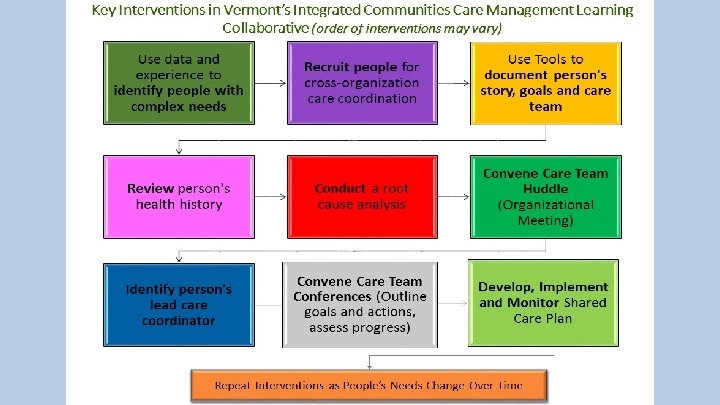
Benefits of Integrated Care Management (ICM) ICM Conventional Care focused on social determinants of health Medical / Clinical Bias-based Participants help plan their own care Directive / Proscriptive / Depersonalized Coordinated interdisciplinary community teams formed around each participant Siloed / Uncoordinated / Redundant / Confusing to the Person Participant priorities and relationships guide goal setting Formulaic / Non-engaging Recurring care conferences and shared care planning Siloed services and multiple care plans Chart review and root cause discovery No Coordinated Review of Root Causes
Process for Engaging Participants: Tools and Methods • Program description – what’s different? • Agreement to participate and Interagency Communication Consent • Appointment of Lead Care Coordinator (LCC) • Initial meeting for Eco-mapping and domain priority identification • Shared Care Conferences • Shared Care Plan (SCP)
Encouraging Involvement of Participants in Planning Their Own Care / Supporting Shared Care Planning Across Multiple Organizations
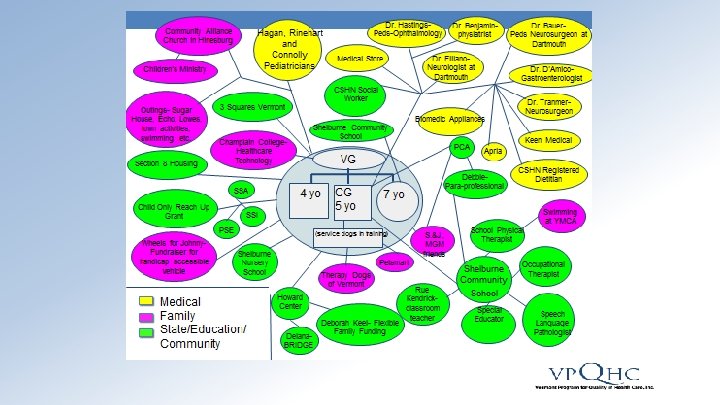
Tools and Methods: Eco-mapping
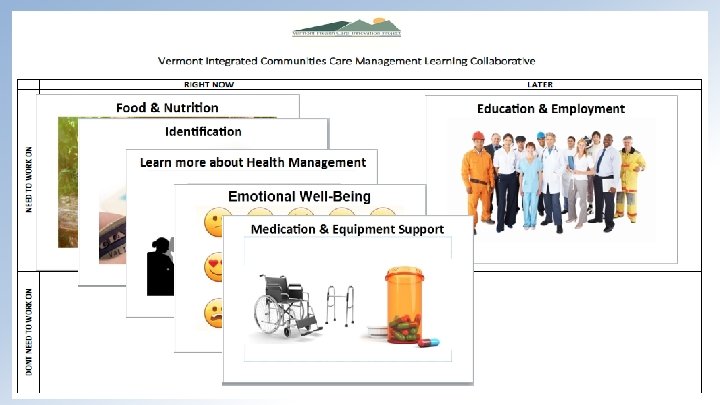
Tools and Methods: Participant Domain Cards “What matters to you? ”
Using the Tools: A Case Study Description of Dave: 54 year old man, paraplegic, living in subsidized housing at one of the SASH (Support and Services at Home) hub sites. Primary issue is wound care that is long standing and he is currently using a wound vac. Very upbeat positive person who is in need of a strong circle of support. Identified by Community Health Team as high utilizer of services, complex care needs, multiple agency assist.
Tools and Methods: Domain Card Planning Board
Chart Review and Root Cause Discovery
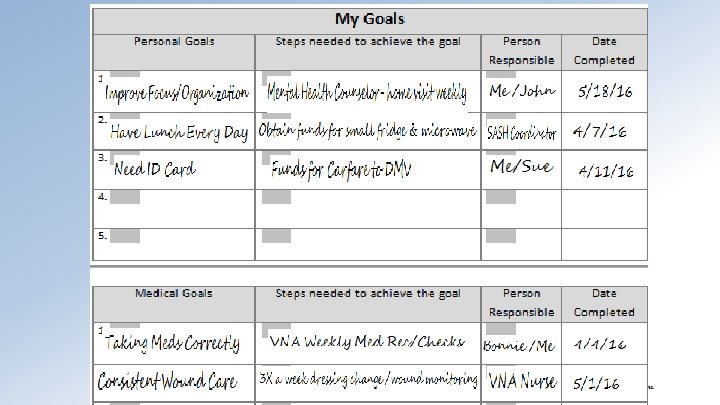
Heart of a Shared Care Plan: Goals and Accountabilities
Case Study Outcomes • Secured funds for a small fridge and microwave for his room, Care Attendant filled with ready-made meals weekly • Secured funds for a non-medical ride to DMV to get an ID, opened a local bank account, obtained meds at pharmacy • Addressed concerns of ADD with mental health counselor and physician • Obtained seat cushion for wheelchair that will help him to sit in electric wheelchair more comfortably • Shared care plan with all medical and non-medical providers
SCP Team Communication and Sharing PCP Person = Owner of SCP ED LCSW LCC = Write/Update SCP Housing Agency
Ongoing Support and Training for Engaged Communities: Learning Collaborative Sessions and ICM Education • Identifying and Engaging People in Cross-Organizational Care Management • Care Coordination Framework for People with Complex Needs: Identifying Lead Care Coordinators and Developing Shared Plans of Care • Understanding the Population and Root Cause Analysis • Conducting Effective Care Conferences
Impact of ICM 2016 ICCMLC Statewide Progress 350 300 250 200 150 100 50 0 January March # With LCC May July # With SCP September # Enrolled November
Impact of ICM • 91% of responding participants agree that their LCC talks with them about what they want for their future • 87% of responding participants chose the goals for their Shared Care Plan • Decreased ED utilization by 50% or more in some communities
Brattleboro Memorial Hospital ICM Participants’ Decreased ER Utilization 10 9 8 7 6 # of ER Visits 5 4 3 2 1 0 Number of ER Visits before ICM Number of ER Visits After ICM 1 2 3 4 5 6 7 8 Participant # 9 10 11 12
2017 YTD Progress on ICM
Continuing and Scaling the Work • Elevator speeches and brochures • Local education sessions for new partners • Continued enrollment of complex needs participants • Adoption of single electronic Shared Care Plan platform statewide • Continued data collection and analysis of process and outcome data
Feedback from Participating ICCMLC Agency Partners • Best practice tools, using Eco maps and Camden cards and care plans, have improved the quality of information, goal setting and care planning and communication with both patients and health and human service partners • Patients are viewed as experts and central in decision-making, i. e. shifting focus to patient centered approach • New funding sources and resources have been discovered for patients when working in partnership • Patients are empowered and are able to accomplish realistic goals when they have an active role in the care plan • Staff participating on shared care teams and in collaborative planning meetings note improved job satisfaction and decreased feeling of burnout
Thank you! Bruce Saffran, BS, RN Vermont Program for Quality in Health Care, Inc. Bruce. S@VPQHC. org (802) 262 -1306