Implementation of a Quality Improvement Project to Improve



 and the American")





")

")
 was made. • No")


















. (2004). Closing the quality gap:")
. Improving diabetes patient outcomes: Framing")
.")
. Non-adherence to diabetes guidelines in primary")
- Slides: 40
Implementation of a Quality Improvement Project to Improve Provider Adherence to American Diabetic Association Standards of Care Ashley Marreel DNP Scholarly Project Creighton University College of Nursing
Disclaimer • This presenter has no financial interest, arrangement or affiliation that would be considered a conflict of interest for this project.
Objectives • At the end of this presentation, participants will be able to: o Identify the four components of the Plan Do Study Act (PDSA) model. o Describe how a tracking tool improves provider adherence to evidence based standards of care.
Background According to the Centers for Disease Control and Prevention (CDC) and the American Diabetes Association (ADA): o o Diabetes affects ~ 29. 1 million/9. 3% of the U. S. Population. 7 th leading cause of death. Total direct/indirect cost = 245 billion dollars (2012). Minorities are more prone to diabetes and the complications.
Literature Review • Guidelines for Diabetes o Standards of Medical Care in Diabetes (ADA, 2014) o Providers must choose to integrate the standards into their treatment and management of diabetes (ADA, 2014). o Essential in achieving quality care for all individuals with diabetes (IDF, 2013). • Adherence to Guidelines o Adherence to tracking tools does make a positive impact in the care of diabetes (Davidson, 2010). o Poor adherence to recommended guidelines is common by health care providers (Their et al. 2008). o Adherence to guidelines was positively related to better prognoses for diabetic patients (AHRQ, 2004).
Literature Review • Diabetes in Minority Populations o Minorities with diabetes are less likely to receive the accepted standards of care (ADA. 2013). o Racial and ethnic minorities are treated differently than whites in the U. S. health care system (IOM, 2003). o Rodriquez et al. (2014) note there is a lack of resources for patients including affordable provider visits and medications. • Diabetes in Free Clinics o Treatment of diabetes among the underserved is difficult in safety net clinics (Rodriquez et al. , 2014). o Care was comparable between insured patients and uninsured patients receiving care from a free clinic (Eldakroury et al. , 2013). o Free clinics can provide high-quality treatment and management (Eldakroury et al. , 2013).
Problem Statement One safety net primary care clinic in the midwest that serves minority and underserved populations currently lacks an effective mechanism to track the ADA Standards of Care within their current charting system.
Purpose • Develop, pilot, evaluate and implement a tracking tool to increase provider adherence to the ADA Standards of Care in a mid-western safety net clinic. • The evaluation included the tracking tool’s content validity and content usefulness.
Theoretical Framework
Chronic Care Model (ICIC, 2014)
Clinical Information Systems • Reminders for providers and patients for the management of their disease (diabetes). • Identify populations for proactive care. • Facilitate care planning. • Share information with patients and providers to coordinate care. • Monitor performance of the practice team and care system. (ICIC, 2014)
PDSA Model (IHI, 2014)
Ethical Approval • Application to Creighton’s Institutional Review Board (IRB) was made. • No IRB approval was necessary.
Design, Setting and Sample • Pilot quality improvement project with four specific aims. • Convenience sample.
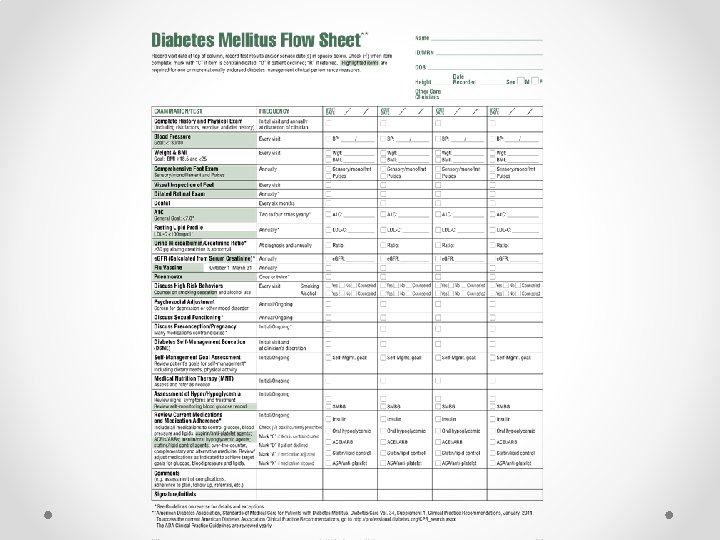
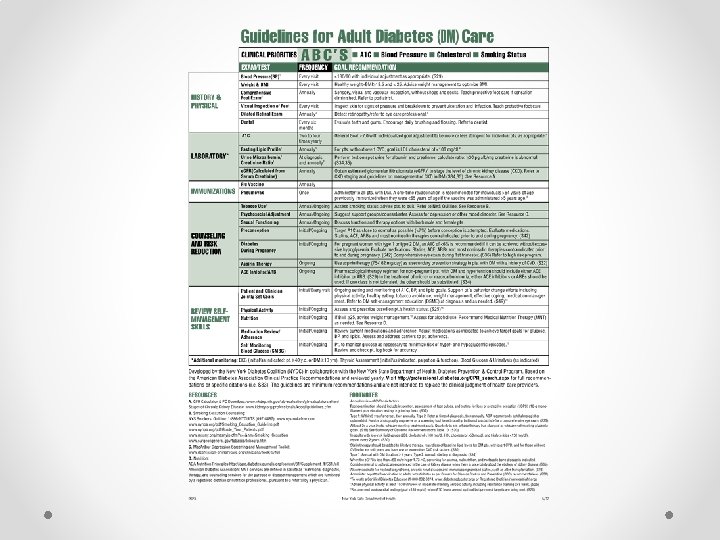
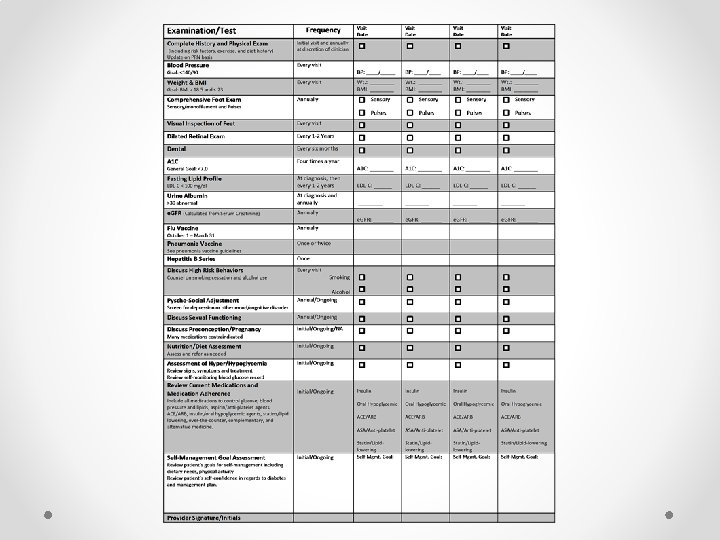
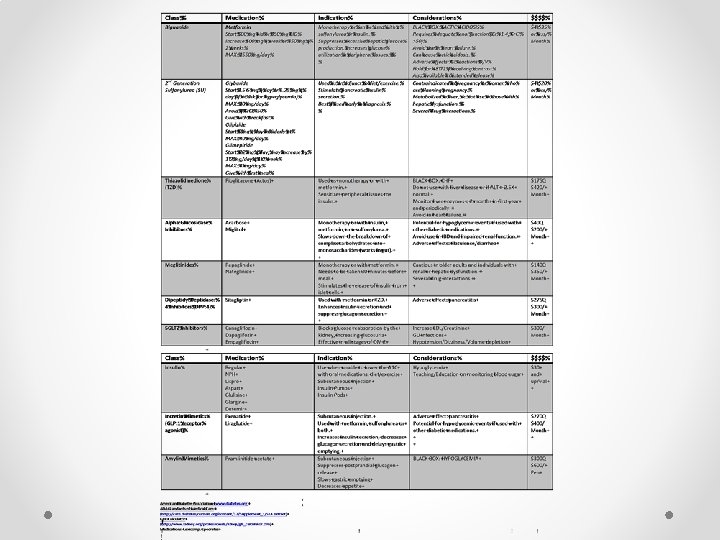
Aim I Develop a tool to track the ADA Standards of Care for diabetics. • Using the CCM and PDSA model a tracking tool was developed and piloted. • Done in collaboration with clinic providers and staff. • Adapted and developed with permission from a tool provided by the New York State Department of Health.
Aim II Pilot and implement a tracking tool following ADA Standards in a Midwestern safety net primary care clinic • Used for diabetic patients seen in the clinic from October 15, 2014 to December 10, 2014 (9 weeks). • After December 10, 2014 the pilot of the tool was discussed, studied analyzed.
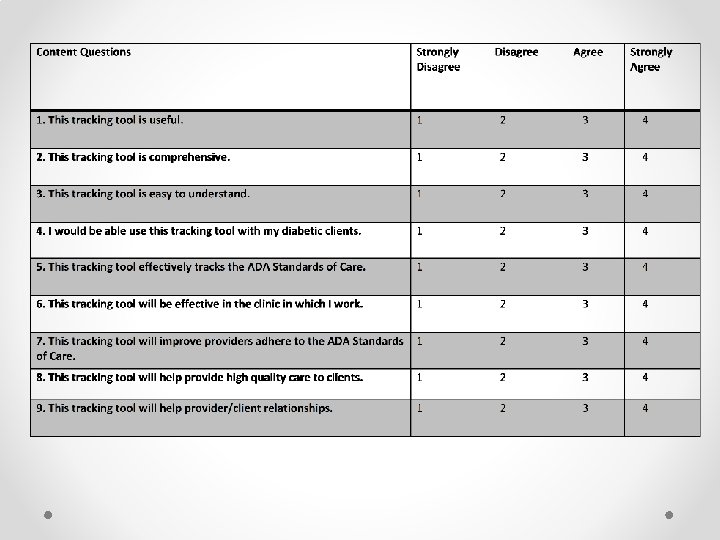
Aim III Analyze content validity of tracking tool using Likert type scale. • Panel of nurse practitioners using a Likert type scale assessed the validity of the tracking tool after the pilot. • No true middle forcing the participants to either agree or disagree. • Seven nurse practitioners participated o 3 have experience in safety net clinics o 4 work in primary care clinics
Aim IV Evaluate the content usefulness of the tracking tool. • The content usefulness was assessed by nurse practitioners/students that volunteer at the clinic. • After the pilot, one nurse practitioner and one nurse practitioner student filled out the content usefulness evaluation.
Statistical Analysis • Descriptive statistics were used to analyze the data obtained from the Likert type scale administration. • Assisted by Chris Wichman, Ph. D
Content Usefulness • The tracking tool was found to be: o o o Useful. Efficient. Easy to use. Visually appealing. Comprehensive in relation to the ADA Standards of Care.
Findings • Quantitative and qualitative data collected established the content validity and usefulness of the diabetic tracking tool. • Using all data collected the final tracking tool was formed and implemented.
Limitations • The tracking tool will need to be updated yearly • Small study and small sample size • One clinic • Very specific population
Discussion • Adherence to the documentation was improved. • Adherence was found to be difficult due to lack of resources. • Provider and patient obstacles were identified. • Throughout the project and residency resources within the community were identified.
Relationship to Literature • Tracking tools do improve provider adherence to standards of care. • Use of the CCM for diabetic patients yields positive results. • Ensures standards of care being tracked and monitored within one place, making the care of diabetic patient less fragmented, cutting down on duplicate services and enhancing the quality of a chronic condition.
Implications for Nursing Practice and Education • APRNs need to be well educated and informed in regards to the ADA Standards of Care. • Educational resources were provided for the clinic to help enhance care of diabetics.
Recommendations for Future Research • Will improved provider documentation and adherence to the standards of care yield better patient outcomes? • Determine if care for diabetic patients in safety net clinics is comparable to other clinics. • Identify more resources within the community.
Conclusions • Content validity and usefulness established. • Provider documentation was improved in this setting. • Specific gaps were identified in assessment, care and resources for diabetics. • The tracking tool may improve provider adherence to the guidelines through a comprehensive and systematic approach for documentation of clinical information.
Acknowledgements • I would like to acknowledge and thank all individuals involved within the project. • A special thank you to: o o o Maribeth Hercinger, Ph. D, RN (Committee Chair) Ann Laughlin, Ph. D, RN (Committee Member) Martha Todd, Ph. D, APRN-NP (Committee Member) Chris Wichman, Ph. D (Statistician) All individuals that volunteer and work at the Porto Urgent Care Clinic All of the individuals that agreed to participate within this project. • I would also like to thank Creighton University’s College of Nursing for all of its support.
THANK YOU! QUESTIONS? ?
References • Agency for Healthcare Research and Quality (AHRQ). (2004). Closing the quality gap: diabetes care strategies. U. S. Department of Health and Human Services. Retrieved from: http: //www. ahrq. gov/research/findings/factsheets/diabetesgap/index. html • Agency for Healthcare Research and Quality (AHRQ). (2008). Module 5: improvement – developing a strategy for diabetes quality improvement. U. S. Department of Health and Human Resources. Retrieved from: http: //www. ahrq. gov/professionals/quality-patient-safety/quality-resources/tools/diabguide/diabqguidemod 5. html • American Diabetes Association (ADA). (2015). Standards of medical care in diabetes 2015. Diabetes Journal, doi: • American Diabetes Association (ADA). (2014). Standards of medical care in diabetes 2014. Diabetes Journal, doi: 10. 2337/dc 14 -SO 14. Retrieved from: http: //care. diabetesjournals. org/content/37/Supplement_1/S 14. full#sec-229 • American Diabetes Association (ADA). (2013). Who is at greater risk for diabetes? Retrieved from http: //www. diabetes. org/diabetes-basics/prevention/risk-factors/ • Centers for Disease Prevention and Control (CDC). (2014). National diabetes factsheet: national estimates and general information on diabetes and pre-diabetes in the United States, 2014. U. S. Department of Health and Human Services. Retrieved from: http: //www. cdc. gov/diabetes/risk/index. html • Centers for Disease Prevention and Control (CDC). (2014). Diabetes: Who is at risk? U. S. Department of Health and Human Services. Retrieved from: http: //www. cdc. gov/diabetes/risk/index. html • Chow, E. , Foster, H. , Gonzalez, V. , Mc. Iver, L. (2012). Disparate impact of diabetes on racial/ethnic minority populations. Clinical Diabetes. 30 (3), 130 -133, doi: 10. 2337/diaclin. 30. 3. 130
References • Dancer, S. , & Courtney, M. (2010). Improving diabetes patient outcomes: Framing research into the chronic care model. Journal of the American Academy of Nurse Practitioners, 22(11), 580 -585. doi: 10. 1111/j. 1745 - 7599. 2010. 00559. x • Davidson, J. A. (2010). The increasing role of primary care physicians in caring for patients with type 2 diabetes mellitus. Mayo Clinic Proceedings, 85(12), S 3 -S 4, doi: 10. 4065/mcp. 2010. 0466 • Eldakroury, A. , Olivera, E. , Bicki, A. , Martin, R. , De. Groot, A. (2013). Adherence to American diabetes association guidelines in a volunteer-run free clinic for the uninsured: better than standards achieved by clinics for insured patients. Rhode Island Medical Journal, 4; 96 (1): 25 -29. • Gonzalez, A. (2012). Vulnerable populations and diabetes preface. Diabetes Spectrum. American Diabetes Association. 25 (1). 6 -7. doi: 10. 2337/diaspect. 25. 1. 6 • Hahn, K. , Ferrante, J. , Crosson, J. , Hudson, S. , Crabtree, B. (2008). Diabetes flow sheet use associated with guideline adherence. Annals of Family Medicine. 6(3): 235 -238, doi: 10. 1370/afm. 812 Improving Chronic Illness Care. (2014). The chronic care model. Group Health Research Institute. Retrieved from: http: //www. improvingchroniccare. org/index. php? p=The_Chronic_Care. Model&s=2 • • International Diabetes Federation. (2013). IDF clinical practice guidelines. International Diabetes Federation. Retrieved from: http: //www. idf. org/guidelines • Institute for Healthcare Improvement. (2014). How to improve. Retrieved from: http: //www. ihi. org/resources/Pages/Howto. Improve/default. aspx • Institute of Medicine. (2003). Unequal treatment: confronting racial and ethnic disparities in healthcare. National Academy of Sciences. Retrieved from: https: //www. iom. edu/~/media/Files/Report%20 Files/2003/Unequal-Treatment-Confronting-Racialand-Ethnic-Disparities-in-Health-Care/Disparities. Admin 8 pg. pdf
References • Kirkman, S. , Caffrey, H. , Williams, S. , Marrero, D. (2002). Impact of a program to improve adherence to diabetes guidelines for primary care physicians. Diabetes Care, 25 (11): 1946 -51. Retrieved from: http: //www. ncbi. nlm. nih. gov/pubmed/12401737 • National Association of Free and Charitable Clinics. (2013). What is a free or charitable clinic? National Association of Free and Charitable Clinics. Retrieved from: http: //nafcclinics. org/about-us/what-is-free-charitable-clinic • National Committee for Quality Assurance (NCQA). (2011). Addressing the quality gaps in diabetes prevention and care. Retrieved from: http: //www. ncqa. org/Publications. Products/Other. Products/Quality. Profiles/Focuson. Diabetes/Addressingthe. Quality. Gaps. aspx • National Diabetes Education Program. (2014). Transform practices to improve care. U. S. Department of Health and Human Services. Retrieved from: http: //ndep. nih. gov/hcp-businesses-and-schools/practice-transformation/improve-practice-quality/transform-practices. aspx • New York Department of Health. (2013). Diabetes prevention and management toolkit. New York State. Retrieved from: https: //www. health. ny. gov/diseases/conditions/diabetes/toolkit_descriptions. htm • Oh, S. , Lee, H. , Chin, H. , Hwang, J. (2011). Adherence to clinical practice guidelines and outcomes in diabetic patients. International Journal for Quality Health Care. 23 (24): 413 -419, doi: 10. 1093/intqhc/mzr 036 • Piatt, G. , Orchard, T. , Emerson, S. , Simmons, D. , Songer, T. , Brooks, M. , Kortykowski, M. , Siminerio, L. , Ahmad, U. , Zgibor, J. , (2006). Translating the chronic care model into the community. Diabetes Care, 29 (4): 811 -817, doi: 10. 2337/diacare. 29. 04. 06. dco 5 -1785 • Regenstein, M. , Huang, J. , Cummings, L. , Lessler, D. , Reilly, B. , Schillinger, D. (2005). Caring for patients with diabetes in safety net hospitals and health systems. The Commonwealth Fund. Retrieved from: http: //www. commonwealthfund. org/usr_doc/826_Regenstein_caringpatientsdiabetes. pdf? section=4039 • Rodriquez, J. , Campbell, K. , Kirksey, O. (2014). Improving diabetes care for minority, uninsured and underserved patients. Immigrant Minority Health. 16: 747 -750, doi: 10. 1007/s 10903 -013 -9965 -7.
References • Seidu, S. , Khunti, K. (2012). Non-adherence to diabetes guidelines in primary care- the enemy of evidence based practice. Diabetes Research and Clinical Practice. 95: 301 -302, doi: 10. 1016/j. diabres. 2012. 015 • Sheehy, A. , Pandhi, N. , Coursin, D. , Flood, G. , Kraft, S. , Johnson, H. , Smith, M. (2011). Minority status and diabetes screening in an ambulatory population. Diabetes Care. 34: 1289 -1294, doi: 10. 2337/dc 10 -1785 • Siminerio, L. , Drab, S. , Gabbay, R. , Gold, K. , Mc. Laughlin, S. , Piatt, G. , Solowiejczyk, J. , Weil, R. (2007). AADE position statement: diabetes educators: implementing the chronic care model. The Diabetes Educator, 34(3); 451 -456, doi: 10. 1177/0145721708316627 • Stellefson, M. , Dipnarine, K. , Stopka, C. (2013). The chronic care model and diabetes management in US primary care settings: a systematic review. Preventing Chronic Disease: Public Health Research, Practice, and Policy, 10: 120180, doi: 10. 5888/pcd 10. 120180 • Their, S. , Yu-Isenberg, K. , Leas, B. , Cantrell, R. , Debussey, S. , Goldfarb, N. , Nash. (2008). In chronic disease, nationwide data show poor adherence by patients to medication and by physicians to guidelines. Managed Care, 17(2): 48 -52, 55 -57.