IMPACTED TEETH Contents n n n n n





 Orthodontic theory : Jaws develop in downward and")
 Phylogenic theory: Nature tries to eliminate the disused organs i. e. , used")
 Mendelian theory: Heredity is most common cause. The hereditary transmission of small jaws")

 Prenatal causes – Hereditary Misagenation b) Post natal causes – All")

 described first classification system which is based on")



 by Pell and Geogory :")
 Based on angulation and position: Same as George Winters.")

 Indications: Ø")






 Spatial Relationship Value - Mesioangular - Horizontal / transverse -")
 Category Score 1. Winters classification Horizontal Distoangular Mesioangular")


 Local anesthesia (vi) needle holder (ii) 15 no. blade (vii) suture material")



 Advantages:")

 Employed to remove any partially formed unerupted")









: YAG laser [by M. Abu-Serriah / A. Ayoub")































")

- Slides: 84
IMPACTED TEETH
Contents n n n n n Glossary of Terms Theories of Impaction Causes Frequency Classification Rationale for Removal Clinical & Radiological Assessment Surgical Anatomy Removal Postoperative Care & Complications
Glossary of terms: n Impacted teeth: A tooth that has failed to erupt into normal functional position beyond the time usually expected for such appearance is impacted. Eruption is prevented by adjacent hard or soft tissue including overlying teeth, bone, or dense soft tissue.
n Partial impaction: A tooth that is incompletely erupted is a partial impaction may be seen clinically but is frequently malposed and always covered to some extent with soft tissue or bone.
n Unerupted teeth: A tooth that has not established normal full communication with the external environment of the oral cavity and remains contained within the hard or soft tissues of the jaw is referred to as Unerupted teeth.
Theories of Impaction By Durbeck 1) Orthodontic theory : Jaws develop in downward and forward direction. Growth of the jaw and movement of teeth occurs in forward direction any thing that interfere with such moment will cause an impaction (small jawdecreased space). A dense bone decreases the movement of the teeth in forward direction. Causes for increased density of bone a) Acute infection, b) Local inflammation of PDL c) Malocclusion, d) trauma, e) Early loss of primary teeth – arrested growth of the jaw.
2) Phylogenic theory: Nature tries to eliminate the disused organs i. e. , used makes the organ develop better, disuse causes slow regression of organ. [More-functional masticatory force – better the development of the jaw] Due to changing nutritional habits of our civilization have practically eliminated needs for large powerful jaws, thus, over centuries the mandible and maxilla decreased in size leaving insufficient room for third molars.
3) Mendelian theory: Heredity is most common cause. The hereditary transmission of small jaws and large teeth from parents to siblings. This may be important etiological factor in the occurrence of impaction.
Causes of Impaction Local causes: n Irregularity in the position and pressure of an adjacent tooth. n The density of overlying or surrounding bone. n Long continued chronic inflammation with the resultant increase in density of the overlying mucous membrane. n Lack of space due to under develop jaws. n Prolong retention of the primary teeth. n Premature loss of primary teeth. n Acquired diseases – such as Necrosis due to infection or abscess and inflammatory changes in the bone due to exanthematous diseases in child.
Systemic causes: a) Prenatal causes – Hereditary Misagenation b) Post natal causes – All the conditions that may interfere with development of child. - Ricketts - Anaemia - Congenital syphilis - Tuberculosis - Endocrinal disfunction c) Rare conditions - Cleidocranial dysostosis - Oxycephaly - Progeria - Achondroplasia - Cleft palate
Frequency of impaction in following order - Mandibular third molars - Maxillary cuspids - Mandibular bicuspids - Mandibular cuspids - Maxillary bicuspids - Maxillary central incisors - Maxillary lateral incisors
Classification Angulation – George Winter (1926) described first classification system which is based on the angulation of the long axis of the impacted third molar with respect to the long axis of the second molar. Mesioangular Horizontal
Vertical Distoangular
In addition impacted teeth also can be angled in buccal and lingual direction. Buccal direction – Bucco version Lingual direction – Lingual version Unusual position – torsiversion
Relationship to the anterior border of the ramus of the mandibular. Another method of classifying impacted third molar is based on the amount of impacted teeth that is covered with the bone of the mandibular ramus. [by Pell & Gregory] Class I : Class III:
n Relative depth of the third molar (Vertical plane) by Pell and Geogory : In this classification the degree is measured by the thickness of overlying bone, the degree of difficulty increases as the relative depth of third molar increases. Position A: Position B: Position C:
Killey & Key’s classification a) Based on angulation and position: Same as George Winters. b) Based on the state of eruption: - Completely erupted - Partially erupted - Unerupted c) Based on pattern of roots: 1) - Fused roots. - Two roots and multiple roots 2) Root pattern may be – - Surgical favourable - Surgical unfavourable
ADA classification: - Soft tissue impaction - Partial bony impaction - Complete bony impaction with unusual complications
Rationale for removing impacted tooth. by Larry J. Peterson (JADA/Vol 123/1992 July) Indications: Ø Preventing and treating pericoronitis. Ø For prevention of dental caries. Ø Orthodontic considerations. Ø To prevent pathosis. Ø Prevention of root resorption. Ø Impacted teeth and dental prosthesis. Ø Prevention of dental diseases.
Contraindications: Ø Extremes of age. Ø Medically compromised patient. Ø Probable excessive damage to the adjacent structures. Ø Prevention of fracture of jaws.
Clinical Examination History: n Most patients are symptomatic. n If so then associated with- n (Pericoronitis / pain / swelling of the face / trismus / enlarged tender lymph nodes) Intraoral examinationn Size of oral cavity. n Degree of mouth opening. n Size of tongue. n Palpation for external oblique & internal oblique ridge in relation with 3 rd molar.
Widely used radiographs: Periapical / OPG / Occlusion. Radiological assessment: Ø Orientation of the tooth. Position and depth of the tooth Winter lines.
White line: Amber line Red line: As a general rule any tooth with redline 5 mm or more is better remove under GA. If redline is 9 mm or more in length the inferior surface of crown of impacted 3 rd molar may be in level or even below the apex of 2 nd molar
n n n Root pattern: Either Favourable Unfavourable Shape of the crown. Texture of investing bone. Position and root pattern of 2 nd molar. Relationship of 3 rd molar to the inferior dental canal.
Darkening of roots Dark & Bifid apex Deflection of roots Interruption of white line of canal Diversion of canal Narrowing of roots Narrowing of canal
DIFFICULTY INDEX Classification: A) Spatial Relationship Value - Mesioangular - Horizontal / transverse - Vertical - Distoangular 1 2 3 4 B) Depth - Level A - Level B - Level C C) Ramus relationship - Class III Example: Mesioangular tooth Difficulty scores: Very difficult 7 -10 1 2 3 Moderately 5 -7 Minimally 3 -4 1 2 3 1 difficulty score is Level B 2 5 -7 Class III 3 Moderately difficult
WHARFE’ ASSESSMENT by Mc. Gregor (1985) Category Score 1. Winters classification Horizontal Distoangular Mesioangular Vertical 2 2 1 0 2. Height of mandible 1 -30 mm 31 -34 mm 35 -39 mm 0 1 2 3. Angulation of 3 rd molar 1° - 50° 60° - 69° 70° -79° 80° - 89° 90°+ 0 1 2 3 4 4. Root shape Complex Favourable curvature Unfavourable curvature 1 2 3 5. Follicles Normal Possibly enlarged Enlarged 0 1 2 6. Path of exit Space available Distal cusp covered Mesial cusp covered Both cusp covered 0 1 2 3 Total 33
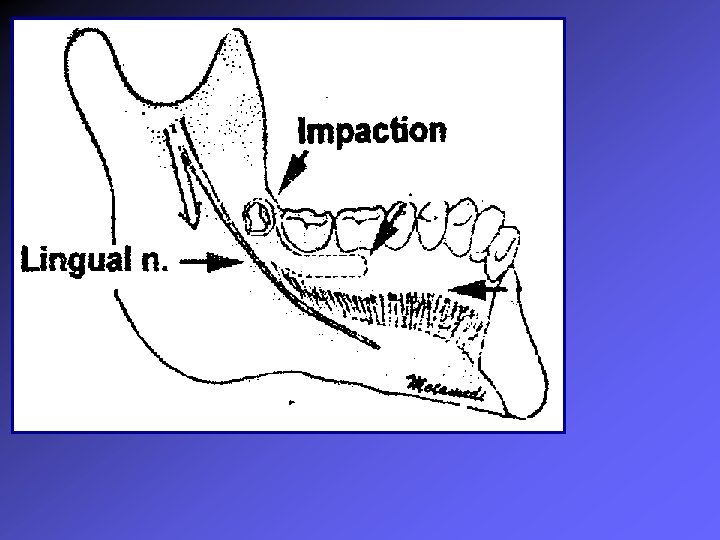
SURGICAL ANATOMY OF MANDIBULAR 3 RD MOLAR Temporalis muscle Buccinator Retro molar foramina
Surgical Removal Following Steps: Ø Anaesthesia Ø Incision and mucoperiosteal flap. Ø Removal of bone. Ø Tooth removal. Ø Wound debridement. Ø Arrest of haemorrhage. Ø Wound closure. Ø Post operative followup.
Armamentarium (i) Local anesthesia (vi) needle holder (ii) 15 no. blade (vii) suture material (iii) Tweezers (viii) scissors (iv) Curette (ix) chisels (v) Elevators (x) mallet (xi) cross bars (xii) retractors
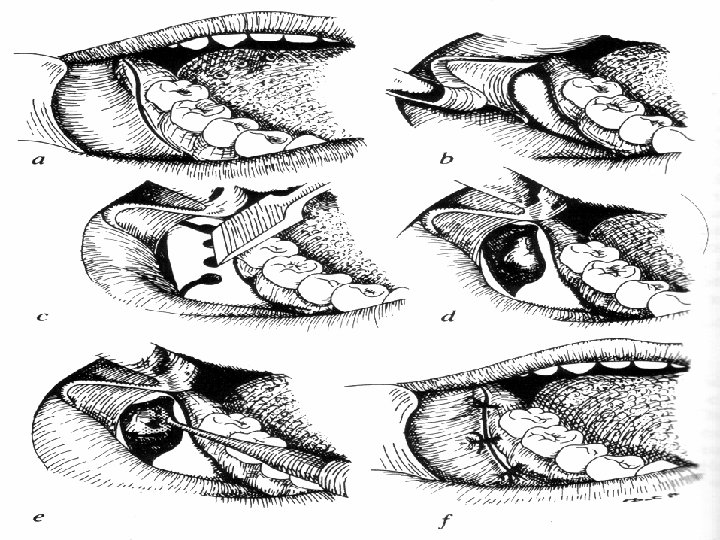
Various incisions / Approaches Ø Standard Wards incision. Ø Modified Wards incision. Ø Envelope flap. Ø L-Shaped flap. Ø Comma incision.
Ward’s incision: Modified Ward’s incision:
Envelop incision: L-shaped flap:
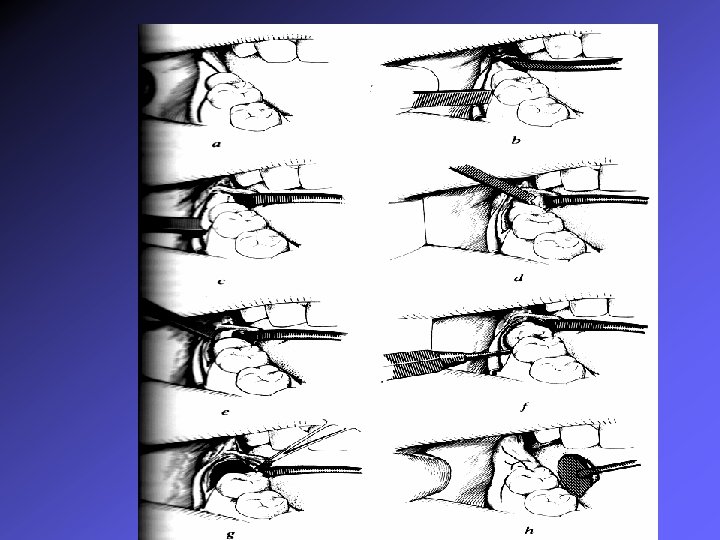
REMOVAL OF OVERLYING BONE I. Lingual split bone tech (Sir William Kelsey Fry) Advantages: 1) Quick & clean 2) Reduces the size of blood clot by means of saucerization of socket. Disadvantages: 1) Only suitable for young adults therefore Elastic Bone. 2) More chances of getting post operating lingual nerve parasthesia. 3) Patients inconvenience.
II. Moor / Gillbes Collor tech: - Conventional tech of using bur. - Similar amount of bone is sacrificed same as split bone technique. - Can be used in old patient with. - Convenient for patient. - Is to create a gutter along buccal side & distal surface of tooth. - And a point of elevation is created with bur.
III. Lateral Trephination tech: - (Bowdler Henry) Employed to remove any partially formed unerupted third molar that has not breached the hard & soft tissues overlying it. Advantages: Bone healing is excellent and here is no loss of alveolar bone around 2 nd molar.
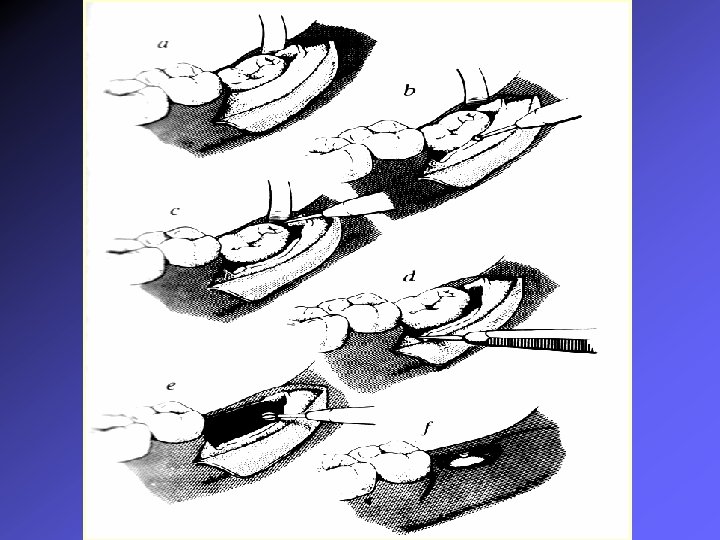
Sectioning TECHNIQUE The tooth is sectioned in different ways.
Horizontal impaction The tooth is sectioned in different ways.
Vertical impaction
Root abnormalities & different techniques of removal
Delivery of sectioned tooth from socket By using appropriate elevators. Straight elevator Warwick James Straight / Curved Coupland’s Cryer’s Cross bar Excessive force should be avoided to prevent injury Soft tissues Adjacent tooth / bone inferior dental canal / lingual nerve
Debridement of wound & closure n n Thorough debridement of the socket by Periapical curette Smoothening of sharp bony margins by Bone file / round burs Thorough irrigation of the socket Betadine solution / Saline Initial wound closure is achieved by Just distal to 2 nd molar Posterior relieving incision Inter dental area mesial to 2 nd molar 3 -4 are usually sufficient
Post-operative care n Pressure pack n Ice pack n Avoid gargling / spitting n Soft diet n Warm water saline gargling after 12 hrs n Maintain oral hygiene n Proper medication
Complications Intra-operative § Soft tissue injuries : § Hard tissue injuries : Ø facial vessels Ø Osseous structures Ø Soft tissues Ø Lingual nerve Ø Inferior dental nerve Ø Bleeding – bone / soft tissue Ø Fracture of mandible Ø Injury to adjacent tooth
Post-operative § Immediate § Late Ø Pain Ø Infection Ø Hemorrhage Ø Dry socket Ø Swelling Ø Osteomylelitis Ø Trismus Ø Secondary Hemorrhage Ø Parasthesia Ø Pain in TMJ
Recent advances Use of Erbium (Er): YAG laser [by M. Abu-Serriah / A. Ayoub : Bjoms 2004; 42: 203 -208] Adv: Ø Less stressful Ø Less unpleasant Ø No vibrations & sound Ø Sharp clean cut through the bone & tooth Ø Can used anxious patients Disadv: Ø Compensate for tactile feedback compare to bur. Ø Trismus is more Ø Time consuming Ø Costly
Thank you
MAXILLARY IMPACTED TEETH
Contents n Maxillary impacted 3 rd molar / impacted canine n Glossary of Terms n Classification n Rationale for Removal n Clinical & Radiological Assessment n Surgical Anatomy n Removal n Postoperative Care & Complications
Glossary of terms: n Impacted teeth: A tooth that has failed to erupt into normal functional position beyond the time usually expected for such appearance is impacted. Eruption is prevented by adjacent hard or soft tissue including overlying teeth, bone, or dense soft tissue.
n Partial impaction: A tooth that is incompletely erupted is a partial impaction may be seen clinically but is frequently malposed and always covered to some extent with soft tissue or bone.
n Unerupted teeth: A tooth that has not established normal full communication with the external environment of the oral cavity and remains contained within the hard or soft tissues of the jaw is referred to as Unerupted teeth.
Impacted Maxillary 3 rd Molars Classified according to the: Ø Position of long axis. Ø Relative depth. Ø Sinus approximation.
POSITION OF LONG AXIS Mesioangular Distoangular Vertical Can be Buccally tilted Palatally tilted Horizontal
ACCORDING TO RELATIVE DEPTH Class A Class B Sinus approximation Class C No sinus approximation
ACCORDING to Killey & Kay n Ø Ø Ø - Upper third molar may be: Unerupted - Within the bone - In soft tissues Partially erupted Fully erupted. Any of these teeth may be Mesioangular/Vertical Laterally displaced & crown facing towards cheek. Distally displaced. Aberrant position. Roots may be Fused (conical). Multiple – Favourable Unfavourable
Indications for Removal Ø Pericoronitis. Ø Dental caries. Ø Pathosis. Ø Root resorption of 2 nd molar. Ø Under dental prosthesis. Ø Causing chronic cheek biting. Ø Impinging on coronoid process. Ø Non-functional (when opposite tooth is removed). Contraindications: Ø Extremes of age. Ø Deep seated tooth with no signs of pathosis.
SURGICAL ANATOMY
SURGICAL STEPS: Ø Anaesthesia Ø Incision and mucoperiosteal flap. Ø Removal of bone. Ø Tooth removal. Ø Wound debridement. Ø Arrest of haemorrhage. Ø Wound closure. Ø Post operative followup.
Factors complicating the removal of tooth n n n n Maxillary sinus approximation. Impacted upper 3 rd molar just above the roots of 2 nd molar. Fusion of 3 rd molar with roots of 2 nd molar. Hypercementosis. Extreme bone density in elderly patients. Difficult access. Abnormal roots.
Approaches Envelope incision Conventional incision
Technique of removing 3 rd molar
Debridement of wound & closure n Thorough debridement of the socket by Periapical curette n Smoothening of sharp bony margins by Bone file n Thorough irrigation of the socket Betadine solution / Saline n Initial wound closure is achieved by
Post-operative care n Pressure pack n Ice pack n Avoid gargling / spitting n Soft diet n Warm water saline gargling after 12 hrs n Maintain oral hygiene n Proper medication
Complications Intra-operative § Ø Ø Ø Soft tissue injuries Soft tissues Injury to vessels / nerves Bleeding – bone / soft tissue Herneation of buccal fat Dislodgement of tooth/ root into Maxillary antrum Soft tissue (infratemporal fossa) Oroantral communication § Ø Ø Hard tissue injuries Fracture of tuberosity. Damage to adjacent tooth
Post-operative Ø Pain Ø Hemorrhage Ø Swelling Ø Infection Ø Dry socket Ø Osteomylelitis Ø Secondary Hemorrhage
Accidental displacement of impacted maxillary 3 rd molar into infratemporal fossa (by M. Patel & Down) BDJ, 1994. n Frequently mentioned but rarely reported.
Action list for prevention of displacement
MANAGEMENT OF IMPACTED MAXILLARY CANINE TEETH n Classification Class I – located in palate – horizontal / vertical semi vertical Class II – located in the labial or buccal surface of the maxilla – horizontal/vertical/semivertical Class III – Crown on palatal side and root on buccal side or vice versa. Class IV – located in alveolar process between incisor and first premolar (usually vertical) Class V – located in edentulous maxilla [ or can be located in unusual position – nasoantral wall or infraorbital margin]
Anatomy
Dowels discussion of etiological factors of canine impaction Ø Ø During the development of the crown of the permanent cuspid lies immediately lingual to the primary canine root. Any change in position of primary canine or premature loss of primary molar. The hard palatal bone offers more resistance to the erupting canine. The mucoperiosteal tissues covering anterior third of the palate are repeatedly subjected to stress and pressure during mastication becomes very dense thick and resistant. Eruption of teeth is dependent to some extent of an associated increase in apical development. This aid to erupting canine is minimized because root normally / more fully formed at the time of eruption.
Ø The tooth must travel at the greater distance from its point of development. Ø Delayed resorption of primary canine root. Ø Canines are the last permanent tooth to erupt in between the teeth already in occlusion. Ø Permanent canine is preceded by primary canine whose M-D is much lesser.
Clinical examination n Intraoral Ø Bulge can be palpable on buccal / lingual side. Ø If impacted canine crown is in contact with apical 3 rd of lateral incisor can cause deflection of tooth.
Radiographic Examination IOPA radiograph Occlusal radiograph
Techniques for removal of impacted canine Semilunar incision Angulated flap incision
Techniques for removal of impacted canine Buccally placed Bilaterally palatally placed
Technique for removal of mandibular impacted canine
Complications n Damaged to adjacent tooth n Perforation of the palate (if placed buccally) n Perforation of nasal mucosa / floor n Perforation of anteral mucosa n Dislodgement of root into maxillary sinus n Haematoma
References n Harry Archer – Oral & Maxillofacial Surg. Part 1 n Geoffery Howe – Minor Oral Surg. n Killey & Kays - Outline of Oral Surg. n Daniel E. Wait – Textbook of Practical Oral & Maxillofacial Surg. n Peterson – Contemporary Oral & Maxillofacial Surg. n Dental Clinics of North America n Killey & Kay – The Impacted Wisdom tooth n Accidental displacement of impacted maxillary third molars (M. Patel, K. Down, Br. dent journal 1994 vol, 177/57 -59)