IMPACTED MAXILLARY THIRD MOLAR PART 1 ZOHAIB ROSHAN
 ZOHAIB ROSHAN SR, OMFS")
IMPACTED MAXILLARY THIRD MOLAR (PART 1) ZOHAIB ROSHAN SR, OMFS

CONTENT 1. Intoduction 2. Anatomy 3. Order of frequency 4. Classification 5. Etiology 6. Indication & contraindication 7. Degree of difficulty

INTRODUCTION • In 1979, a consensus development conference practicing dentists and scientists, on third molar removal was sponsored by national institute of health, USA. J oral surgery…vol 38, march 1980. • The third molar has been the most widely discussed tooth in the dental literature, and the debatable question “…. . to extract or not to extract” seems set to run into the next century. • - Faiez N. Hattab, JOMS, 57: 389 -391 (1999)

DEFINATION • Impaction is the cessation of the eruption of a tooth caused by a clinically or radiographycally detectable physical barrier in the eruption path or by an ectopic position of the tooth. Andreasen et al (1997). • Archer (1975) defines impacted tooth as one which is completely or partially unerupted and is positioned against another tooth or bone or soft tissue so that its further eruption is unlike

• WHO : - An impacted tooth is the one that is unable to fully erupt in its normal functional occlusion / location by its expected age of eruption, because it is blocked by overlying soft tissue or bone or another tooth. • More common in females than males, in maxilla than in mandible and on right side than left.
 • 2 nd largest bone of face • 2 maxillae forms whole")
ANATOMY (MAXILLA) • 2 nd largest bone of face • 2 maxillae forms whole of upper jaw • Each maxilla contributes in formation of 1. 2. 3. 4. 5. 6. Face Nose Mouth Orbit Infratemporal fossa Pterygopalatine fossa

• Shape – pyramidal Each maxilla has – • A body • 4 processes – frontal • zygomatic alveolar palatine It has – • Base – directed medially at nasal surface • Apex - directed laterally at zygomatic process • 4 surfaces – anterior / facial • posterior / infratemporal medial / nasal • superior / orbital Encloses a cavity – maxillary sinus

SURGICAL ANATOMY

FREQUENCY OF IMPACTION mandibular 3 rd molars maxillary cuspid mandibular bicuspids Maxillary bicuspids Mandibular canine maxillary central and lateral incisors

CLASSIFICATION 1. Based on state of eruption Fully erupted Partially erupted Unerupted • Within the bone • Immediatey beneath the soft tisses
 - Vertical – 63 % Mesioangular - 25 %")
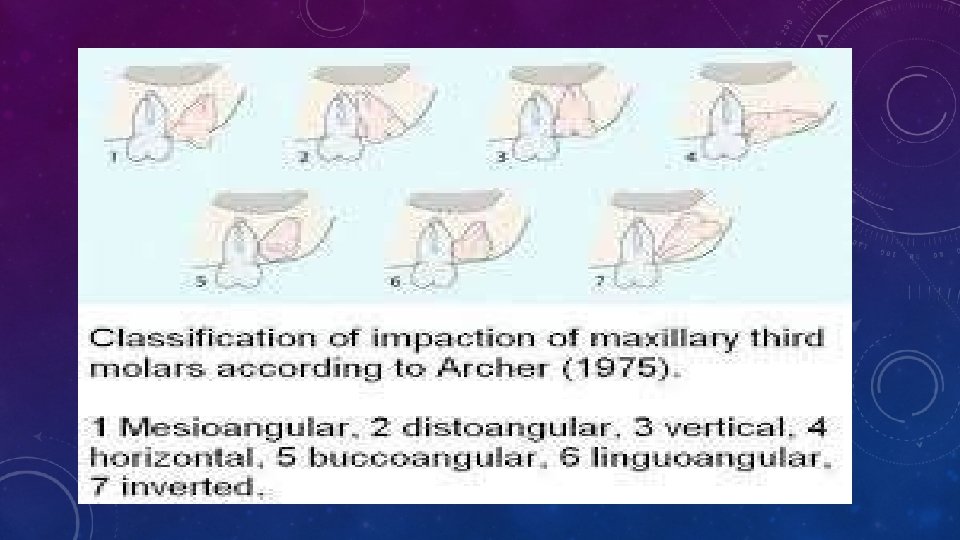
2. BASED ON ANGULATION (ARCHER) - Vertical – 63 % Mesioangular - 25 %

DISTOANGULAR- 12% • Laterally displaced with the crown facing the cheek, horizontal, inverted, and transverse positions <1% • Aberrant position associated with pathologial condition such as cyst.
 � Position A - highest point(occlusal")
3. BASED ON THE DEPTH: (PELL AND GREGORY) � Position A - highest point(occlusal surface) of 2 nd molar and highest point(occlusal surface)of impacted 3 rd molar is in same line. � Position B - highest point of 3 rd molar is in between plane of occlusion and cervical line. � Position C - highest point of 3 rd molar is below cervical line.

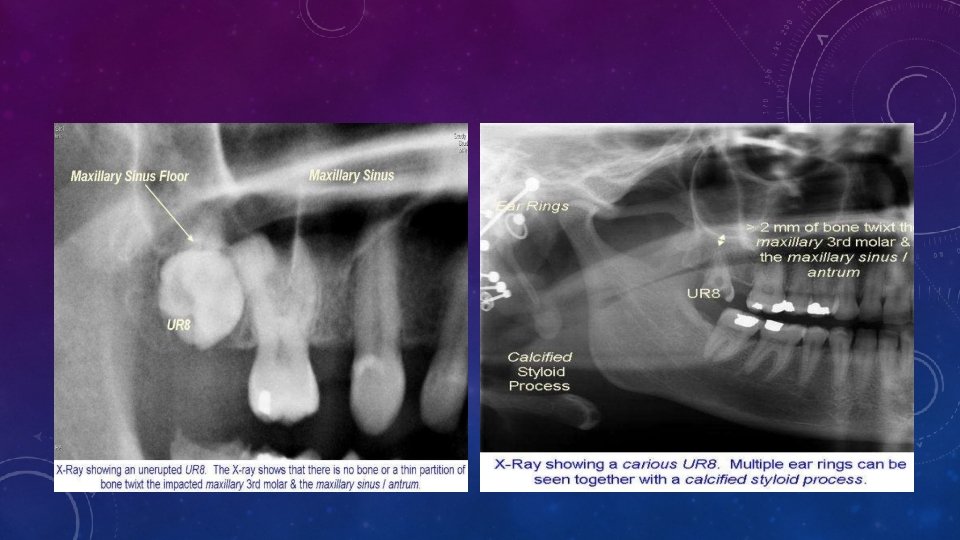
4. Based On Relationship Of Impacted Max 3 rd Molar To The Max Sinus • Sinus Approximation (S. A) no bone or a thin partition of bone between the impacted tooth and the maxillary sinus. • No Sinus Approximation (N. S. A) 2 mm or more bone present 5. Based on nature of roots • Fused • Multiple

ETIOLOGY LOCAL CAUSES: 1. 2. 3. a. b. c. 4. 5. Density of overlying bone Lack of space due to undedeveloped jaws Obstruction. Over-retained deciduous tooth Thick fibrous alveolar mucosa Cyst/tumors Dialceration Ectopic tooth eruption

SYSTEMIC CAUSES: 1. 2. a. b. c. 3. a. b. Pre-natal: heredity Post-natal: factors that interfer with development. Rickets Malnutrition anaemia Rare conditions: Cleft lip osteoporosis

INDICATIONS FOR REMOVAL • Extensive caries • Recrrent pericoronitis • Malplaced tooth which causes the patient to adopt a convenience bite to avoid cheek biting. • Tooth involved in pathogical process like cyst, • Buccaly erupting tooth which causes impinging on the coronoid process. • Interference with placement of prosthesis.

LOCAL CONTRAINDICATIONS FOR REMOVAL • Symptomless tooth completely embedded in bone • Tooth positioned high in alveolus-Risk of displacing tooth into max antrum • Deeply impacted tooth – removal may cause damage to adjacent structures.

DEGREE OF DIFFICULTY • Angulation - opposite to mandibular 3 rdmolar. • Distoangular < Vertical< Mesioangular impaction • In MA impactions, bone in distal region is more and dense with less accessability. • Buccoangular position: more buccal more easy, less bone removal needed. • Type of overlying tissue - Easier if soft tissue covering only. • Sinus poximity – Chance of oro antral communiation. • Poximity to tuberosity – chance of fracture.

OTHER FACTORS • Tooth with thin, curved, hypercementosed roots difficult. • Tooth wider periodontal space, follicular space – easier • Difficult access • Presence of large restoration on second molar. • Bone density

THANK YOU
- Slides: 23